Oral Medicine Infections Of Oral Cavity Important Notes
1. Theories Of Dental Caries Theory
2. Zones Of Dental Caries
- Enamel Caries
- Zone 1 – Translucent zone
- Zone 2 – Dark zone
- Zone 3 – Body of lesion
- Zone 4 – Surface zone
- Dentinal Caries
- Zone 1 – Zone of fatty degeneration
- Zone 2 – Zone of dental sclerosis
- Zone 3 – Zone of decalcification of dentin
- Zone 4 – Zone of bacterial invasion
- Zone 5 – Zone of decomposed dentin
Read And Learn More: Oral Medicine Question and Answers
3. Ludwig’s Angina
- It is a severe form of cellulitis
- Begins in submaxillary space and secondarily involves sublingual and submental spaces
- Mandibular molars are source of infection
- Manifests as rapidly developing broad-like swelling of the floor of the mouth
- Results in elevation of the tongue with difficulty in swallowing and breathing
- If the infection spreads to the neck it leads to edema of the glottis
- Suffocation may lead to death
- Emergency tracheostomy is done
Oral Medicine Infections Of Oral Cavity Short Essays
Question 1. Focal infection
Answer:
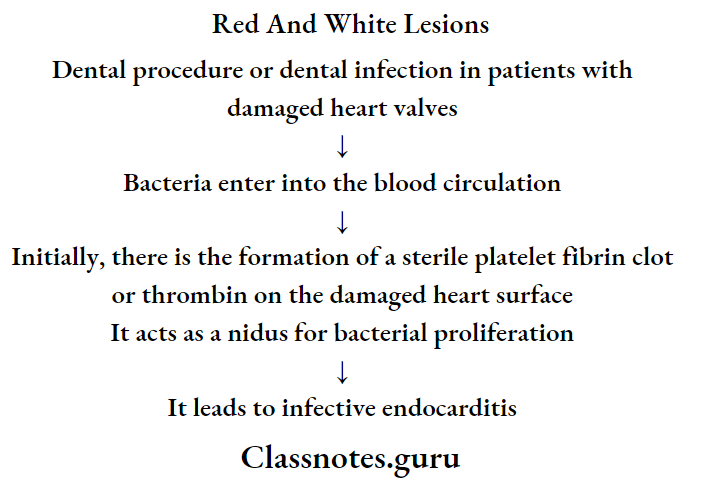
Focal Infection
Focal infection is a localized or general infection caused by the dissemination of microorganisms or toxic products from a focus of infection
Focal Infection Mechanism:
- Spread of pathogenic micro-organisms from their primary site of infection to the distant part of the body via blood vessels or lymphatics
- Spread of toxins liberated by the pathogenic microbes to distant organs either via blood vessels or lymphatics
Focal Infection Significance:
- It causes a great number of systemic diseases like
- Arthritis
- Valvular heart diseases
- Gastro-intestinal diseases
- Ocular diseases
- Skin diseases
- Renal diseases
Question 2. Dental fluorosis.
Answer:
Dental Fluorosis
Dental Fluorosis is caused by excessive intake of fluoride during tooth development
Dental Fluorosis Clinical Features:
- Lustreless, opaque white patches in the enamel may become mottled, striated, or pitted
- Mottled areas may become stained yellow or brown
- Hypoplastic areas may also be present to such an extent in severe cases that normal tooth form is lost
- Enamel fluorosis is a developmental phenomenon due to excessive fluoride ingestion during amelogenesis
- Once crowns are formed no further fluorosis occurs
- The hypocalcified areas of the mottled enamel are less soluble in acids
- They have a greater permeability to dyes
- They emit fluorescence of higher intensity than normal enamel
- Fluorosis occurs symmetrically within arches
- The premolars are usually first affected followed by the second molar, maxillary incisor, canine, first molar, and mandibular incisors
Oral Medicine Infections Of Oral Cavity Short Answers
Question 1. Mucous patches
Answer:
Mucous Patches
- Mucous Patches is a feature of secondary syphilis
- Mucous patches develop over the oral mucosa
- They are painless, multiple, greyish-white plaques overlying the ulcerated surface
Question 2. Chemical burn
Answer:
Chemical Burn
- Chemical Burn is a burn caused due to caustic chemical agents
- Chemical Burn produces coagulation necrosis of the epithelium
Chemical Burn Causes:
- Aspirin and aspirin-containing compounds
- Hydrogen peroxide
- Silver nitrate- Used in the treatment of aphthous ulcers
- Toothache drop burns
- Ethyl alcohol burns- Topical application of ethyl alcohol solution
- Acid burns
- Ingestion- Due to ingestion of caustic chemicals
Chemical Burns Clinical Features:
- Painful lesion
- Appears as an irregularly shaped, white pseudomembrane-covered lesion
- Gentle lateral pressure causes the white material to slide away exposing painful central red ulceration
Chemical Burn Management:
- Topical application of dyclonine hydrochloride
- A protective coat of emollient paste
- Surgical debridement of necrosed tissue
Question 3. Causes for bleeding in the oral cavity
Answer:
Causes Of Bleeding From Mouth:
- Bleeding diathesis
- Carcinoma, squamous cell of head and neck – bleeding from the mouth
- Crown placement
- Dental caries
- Dental cleaning
- Dentures
- Hemophilia
- Idiopathic thrombocytopenic purpura
- Leukemia
- Pancytopenia
- Periodontal disease
- Plaque
- Post tonsillectomy bleeding
- Root canal
- Stomatitis
- Thrombocytopenia
- Tonsillar abscess
- Tooth extraction
- Trauma
- Viral Hemorrhagic Fevers
Question 4. Cellulitis
Answer:
Cellulitis Definition:
- Cellulitis is an acute, edematous, purulent inflammatory process that spreads diffusely through different tissue spaces
Cellulitis Sources Of Infections:
- Periapical abscess
- Pericoronitis
- Periodontal abscess
- Osteomyelitis
- Infected post-extraction wound
- Gunshot injuries
- Oral soft tissue infections
- Bloodborne infections
Cellulitis Clinical Features:
- Large, diffuse, painful swelling over the face or neck
- The overlying skin appears purplish
- Fever, chills
- Leukocytosis
- Regional lymphadenopathy
- Pus discharging sinuses
Cellulitis Complications:
- Trismus
- Dyspnoea
- Dysphagia
Question 5. Causes of Pigmentations
Answer:
Causes Of Pigmentations
- Exogenous Pigmentation
- Occupational
- Lead industry-lead
- Match industry- Phosphorous
- Fluorescent lamp industry- mercury
- Photography- Silver
- Habits
- Tobacco
- Pan
- Foodstuffs
- Therapeutic
- Drugs like anti-malarial drugs
- Metallic salts
- Others
- Amalgam tattoo
- Black hairy tongue
- Occupational
- Causes Of Pigmentations Endogenous
- Physiologic
- Racial variation
- Physiologic melanotic macule and papule
- Fordyce’s granules
- Pregnancy
- Pathological
- Addison’s disease
- Acromegaly
- Peutz-Jeghers syndrome
- Nevi
- Malnutrition
- Physiologic
Question 6. Caries vaccine
Answer:
Caries Vaccine
- Caries Vaccine is a suspension of an attenuated or killed micro-organism administered for the prevention, amelioration, or treatment of infectious diseases
Caries Vaccine Mechanism Of Action:
- When the tooth erupts serum antibodies i.e. IgA stimulate opsonization and phagocytosis
- These antibodies have an inhibitory effect on glucosyl transferase and acid production
- It results in the inhibition of the metabolic activity of mutants in teeth
Caries Vaccine Route Of Administration:
- Oral route
- Systemic route
- Active gingivo-salivary route
- Active immunization
- Synthetic peptides
- Coupling with cholera toxin subunits
- Fusing with avirulent strains of salmonella
- Liposomes- increases IgA antibodies
- Passive immunization
Oral Medicine Infections Of Oral Cavity Viva Voce
- Denture sore mouth is rarely found under the mandibular denture
- Minocycline produced oral pigmentation
- Amalgam tattoo is the most common source of focal pigmentation
- Strawberry tongue is the result of an infection caused by streptococcus pyogenes
- The critical pH of dental caries is 5.2
- Initiation of dental caries is caused by streptococcus mutans
- Progression of dental caries is by lactobacillus
- Pioneer bacteria is seen in the earliest stage of caries