Muscles Of The Pectoral Region – Full Notes Pectoral Region Introduction
- The pectoral region lies on the front of the chest.
- It consists of structures that connect the upper limb to the anterolateral chest wall.
Pectoral Region Question And Answers
Question 1. Briefly mention the superficial fascia of the pectoral region.
Answer:
Superficial Fascia
- It lies under the skin of the pectoral region and is continuous with surrounding superficial fascia. Its contents are:
- Moderate amount of fat
- Cutaneous nerves derived from the cervical plexus and intercostal nerves
- Cutaneous arterial branches from internal thoracic and posterior intercostal arteries
- Platysma muscle
- Breast/mammary gland.
Read And Learn More: Upper Limb
Question 2. Write a short note on platysma muscle.
Answer:
Platysma Muscle:
 Pectoral Muscles Anatomy Short Essay
Pectoral Muscles Anatomy Short Essay
Question 3. Explain in detail about the breast under the headings—situation and structure, blood supply, nerve supply, and lymphatic drainage.
Answer:
- The breast is a modified sweat gland.
- It is present in both sexes but rudimentary in males whereas well-developed in females after puberty.
- It is an important accessory organ of the female reproductive system and provides nutrition to the newborn in the form of milk.
Situation, Relations, And Extent
- It is situated in the superficial fascia of the pectoral region except for the tail which pierces the deep fascia of the axilla through the ‘foramen of Langer’ and is called the ‘tail of Spence’
- Breast extends:
- Vertically: From 2nd to 6th rib
- Horizontally: Lateral border of sternum to midaxillary line.
- Superficial Relations: Skin and Superficial Fascia
- Deep Relations:
- Retromammary space: Loose areolar tissue separating the breast from the deep pectoral fascia, hence the breast is freely movable over the pectoralis major
- Pectoral fascia
- 3 muscles over which the base of the gland rests
- Pectoralis major
- Serratus anterior
- External oblique (a part)
- Structures deeper to them
- Clavipectoral fascia
- Pectoralis major
Pectoral Region Muscles Viva Questions and Answers
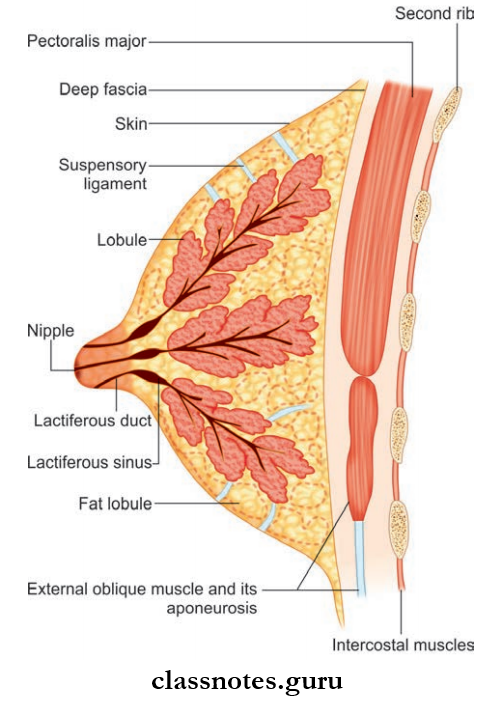
Structure Of the Breast
- The Structure consists of:
- Skin
- Areola
- Parenchyma
- Stroma
- Structure Of Breast Skin
- It covers the gland and presents the nipple and areola.
- The nipple is the conical projection situated usually at the
center of the breast corresponding to the 4th intercostal space. - It is pierced by 15–20 lactiferous ducts.
- It is rich in sensory nerve endings and very sensitive to touch.
- Structure of the Breast Areola
- It is the circular area of pigmented skin surrounding the base of the nipple.
- It is rich in sebaceous glands, especially in the outer margin, which produces oily secretion, preventing nipple and areola from drying and crusting.
- In pregnancy, the areola becomes darker and enlarged.
- Montgomery’s tubercles are the enlarged sebaceous glands around the nipple in pregnancy.
- Structure of Breast Parenchyma
- It is the glandular part of the mammary gland which secretes milk.
- It consists of 15–20 lobes arranged in a radial fashion around the nipple and opens into it through lactiferous ducts.
- Each lobe consists of lobules which are filled with clusters of acini-secreting milk.
- Lactiferous sinuses are dilated part of the lactiferous duct that helps to secrete milk.
- Structure of Breast Stroma
- It is the supporting framework of the mammary gland.
- It is made up of fibrofatty tissue.
- The fibrofatty tissue is modified to form suspensory ligaments of cooper and suspends breast tissue to the skin and pectoral fascia.
Upper Limb Muscles – Pectoral Region Guide
Breast Blood Supply The breast is highly vascular. It is supplied by:
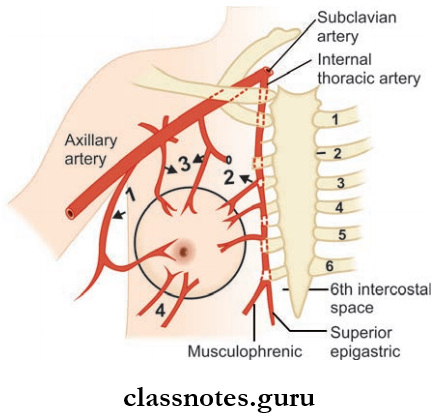
- Branches of lateral thoracic artery;
- Branches of internal thoracic artery;
- Branches of acromiothoracic and superior thoracic arteries
- Branches of 2nd, 3rd and 4th posterior intercostal arteries
- Arterial Supply
- Internal thoracic artery through its perforating branches
- Axillary artery through:
- Lateral thoracic
- Superior thoracic
- Acromiothoracic arteries
- Posterior intercostal arteries through lateral branches.
- Venous Drainage
- Axillary vein
- Internal thoracic vein
- Posterior intercostal vein.
- Nerve Supply
- Cutaneous supply by 4th, 5th, and 6th intercostal nerves.
- Lymphatic Drainage
- Lymphatic drainage of the breast is of great importance as they are the common channels through which metastasis of the breast cancer cells occurs to the opposite breast and other organs.
- The lymph nodes draining the breast are:
1. Axillary Lymph Node:
- They drain about 75% of the lymph from the breast.
- Among them, lymphatics end mainly in the anterior/pectoral group.
- Lymph from the anterior and posterior groups passes to central and lateral groups and through them to the apical group.
- Eventually, lymph reaches the supraclavicular lymph nodes.
2. Internal Mammary Nodes are arranged along the internal thoracic vessels.
- They drain about 20% of the lymph from the breast.
- They drain from both the inner and outer half of the breast.
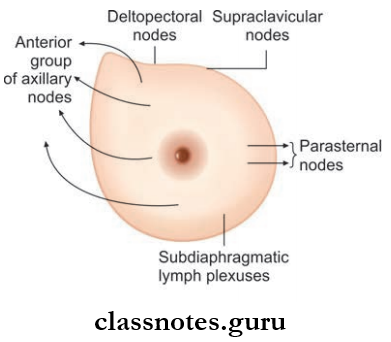
3. Supraclavicular Nodes.
4. Cephalic/deltopectoral Lymph Nodes.
5. Posterior Intercostal Nodes.
6. Subdiaphragmatic Lymph Nodes.
7. Subperitoneal Lymph Plexus.
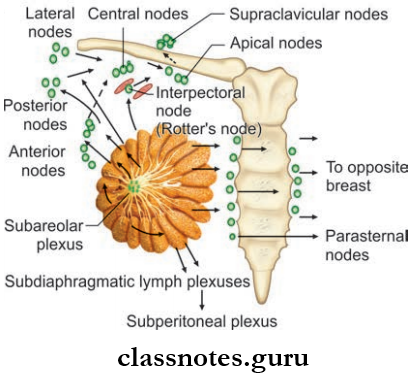
- Lymphatic Vessels draining the breast are:
- Superficial lymphatics drain the skin over the breast except for the nipple and areola to the surrounding lymph nodes (axillary, internal mammary, posterior intercostal nodes) radially.
- It is important to note that superficial lymphatics of the breast on one side communicate with those of the opposite side. So unilateral breast malignancies become bilateral through metastasis.
- Deep lymphatics drain the parenchyma of the breast along with the nipple and areola.
- The subareolar plexus of sappy is a plexus of lymphatics present deep in the areola. They drain into anterior axillary lymph nodes.
- Lymphatics from the deeper part of the breast drain directly into the apical group of axillary lymph nodes or to the internal mammary lymph nodes.
- Few lymph vessels from the inner part of the breast communicate with the subdiaphragmatic and subperitoneal lymphatic plexus.
Clinical Anatomy
- Knowledge of lymphatic drainage of the breast is very important as lymphadenopathy is an early and important sign for staging, treatment, and prognosis of breast cancer.
- Though lymphatics cancer cells can communicate with the opposite breast and other organs in the body.
- Self-examination of the breast stands as the simplest, yet important, way to find malignancy in the early stage itself. On examination note:
- Symmetry of breast and nipple
- Change in the color of skin
- Retraction of nipple
- Discharge from nipple
- Any palpable lump
- Cancer cells from the breast can shed of to the peritoneal cavity and move to the ovary causing ovarian tumors known as Krukenberg’s tumor.
- Tubercle of Montgomery stands as an important medico-legal evidence of pregnancy.
- The suspensory ligament of Cooper degenerates with aging and the breast becomes pendulous as age advances.
- Gynecomastia is the development of breasts in males due to hormonal imbalance and other reasons.
Pectoralis Major and Minor – Short Answer Type Questions
Question 4. Write briefly about clavipectoral fascia. What are the structures passing through it?
Answer:
Clavipectoral Fascia is a fibrous sheet situated deep in the clavicular part of the pectoralis major muscle.
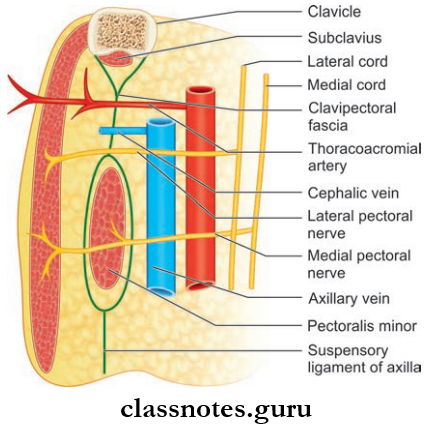
Clavipectoral Fascia Extend
- Vertically: From the clavicle above to the axillary fascia below.
- Medially: Attached to the first rib and costoclavicular ligament and blend with the external intercostal membrane of the upper two intercostal spaces.
- Laterally: Attached to the coracoids process and blends with coracoclavicular ligament.
- The clavipectoral fascia is split into two laminae in the upper part to enclose the subclavius muscle.
- The anterior lamina is attached to the clavicle while the posterior lamina is continuous with the investing layer of deep cervical fascia.
- It is split into two laminae in the lower part to enclose the pectoralis minor muscle.
- After enclosing the muscle, it extends downwards as the suspensory ligament of axilla which helps to pull up the dome of axillary fascia.
Structures Piercing the Clavipectoral Fascia
- Lateral pectoral nerve
- Cephalic vein
- Thracoacromial vessels
- Lymphatics from the breast and pectoral region to the apical group of axillary lymph nodes.
Question 5. Enumerate pectoral muscles.
Answer:
Enumerate Pectoral Muscles They are:
- Pectoralis major
- Pectoralis minor
- Known as the key muscle of the axilla as it divides the axillary artery into:
- Subclavius
- Serratus anterior (not strictly a muscle of the pectoral region).
Question 6. Write a short note on the pectoralis major muscle.
Answer:
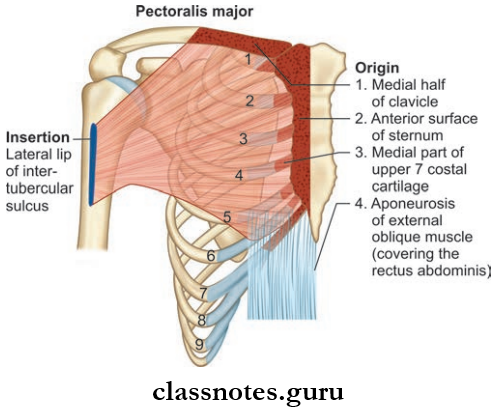
Pectoralis Major
Pectoralis Major Origin
- Small clavicular head: Medial half of anterior aspect of the clavicle
- Large sternocostal head:
- The lateral half of the anterior surface of the sternum up to the 6th rib
- The medial end of 2nd to 6th costal cartilages
- The aponeurosis of the external oblique muscle of the abdomen
Pectoralis Major Insertion
- Inserted into lateral lip of intertubercular sulcus by a U shaped bilaminar tendon
- Anterior lamina of tendon is formed by clavicular fiers
- Posterior lamina formed by sternocostal fiers
- Two laminas are continuous inferiorly
- Lower sternocostal and abdominal fibers are twisted in a way such that the lowest fibers are inserted highest
Pectoralis Major Nerve Supply
- Lateral pectoral nerve
- Medial pectoral nerve
Pectoralis Major Actions
- Clavicular Head: Flexes arm
- Sternocostal Head: Adducts and medially rotates the arm.
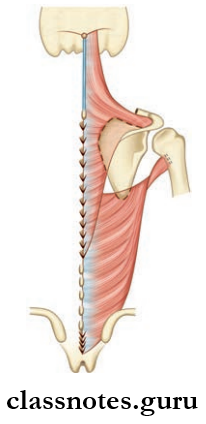
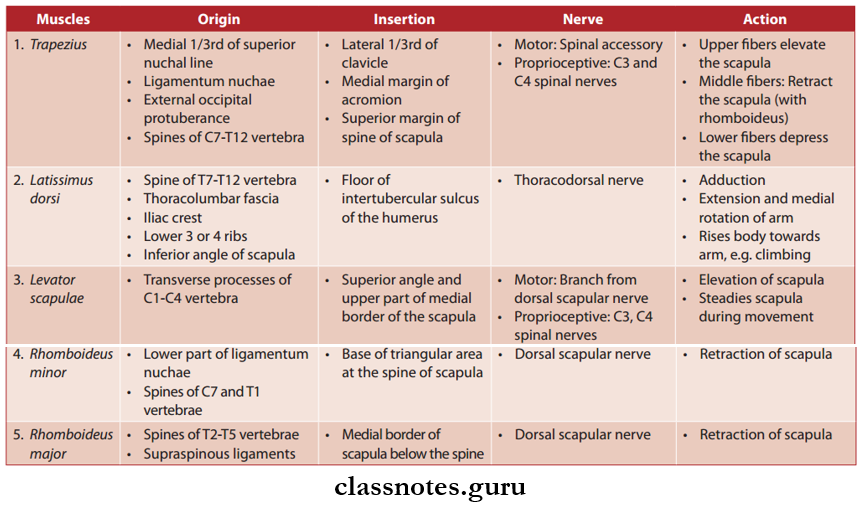
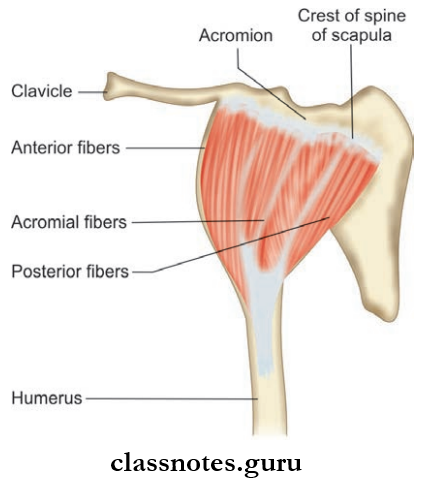
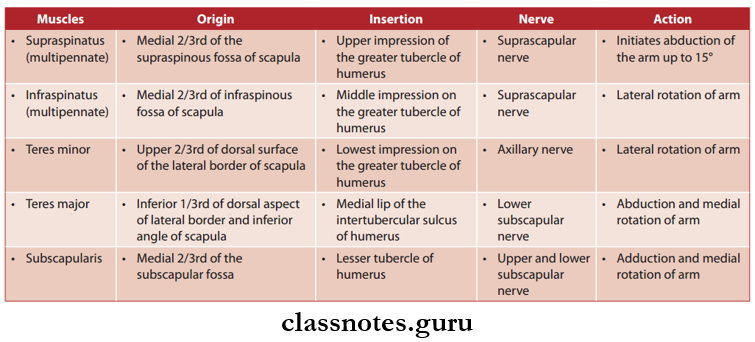
Question 7. Write about the origin, insertion, nerve supply, and actions of the remaining pectoral muscles.
Answer:
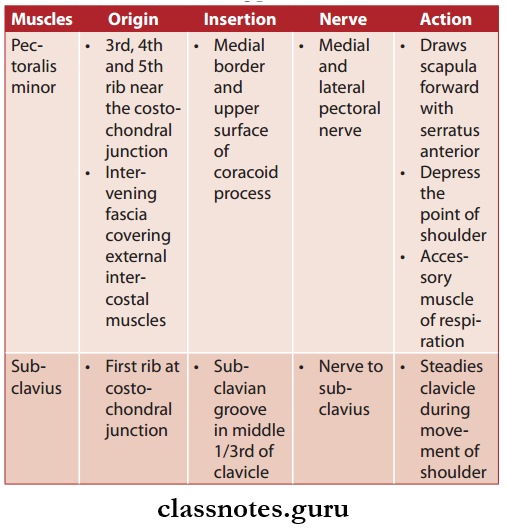
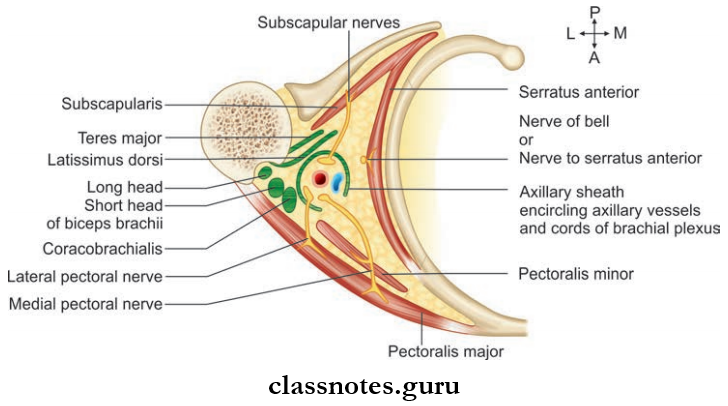
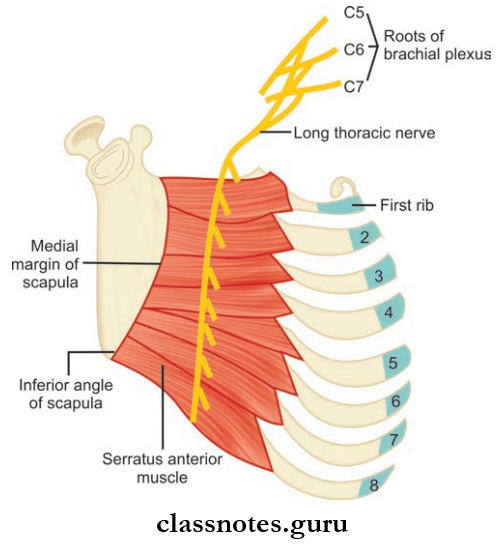
Question 8. Write a note on the serratus anterior muscle.
Answer:
Serratus Anterior Origin
- 8 digitations from the upper 8 ribs
- Fascia covering intervening intercostal muscles
Serratus Anterior Insertion: Costal surface of the scapula along its medial border
Serratus Anterior Nerve Supply: Nerve to serratus anterior (from the root of C5, C6, and C7)
Serratus Anterior Actions
- Pulls scapula forwards around the chest wall (along with pectoralis major)
- Keep the medial border of the scapula in firm contact with the chest wall
- Rotates scapula laterally and upwards during overhead abduction of arm
Mnemonic
- Serratus anterior: Innervation
- SALT: Serratus Anterior = Long Thoracic
Mnemonic Clinical Anatomy
- Injury to the long thoracic nerve (nerve of bell) can occur in:
- Stab wounds
- During the removal of a breast tumor
- Sudden pressure on the shoulder from above
- Carrying a heavy load on the shoulder
- It results in paralysis of the serratus anterior and results in winging of the scapula
Pectoral Region Multiple-Choice Questions
Question 1. On climbing a tree, which of these two muscles at together?
- Teres major and teres minor
- Latissimus dorsi and teres major
- Pectoralis major and latissimus dorsi
- Teres major and pectoralis major
Answer: 3. Pectoralis major and latissimus dorsi
Question 2. Ligaments of Cooper are modifications of:
- Axillary fascia
- Pectoral fascia
- The fatty tissue of the breast
- The fibrous stroma of breast
Answer: 4. Fibrous stroma of breast
Question 3. Which among these does not pierce clavipectoral fascia?
- Lateral pectoral nerve
- Cephalic vein
- Thracoacromial vessels
- Subclavian artery
Answer: 4. Subclavian artery
Question 4. Which among these are not an early warning sign of breast cancer?
- Change in the color of skin
- Gliding mass under the skin of the breast
- Retraction of nipple
- Discharge from nipple
Answer: 2. Gliding mass under the skin of the breast
Question 5. Which among these is not a pure pectoral muscle?
- Pectoralis major
- Pectoralis minor
- Serratus anterior
- Subclavius
Answer: 3. Serratus anterior