Growth And Development General Principles And Concepts Definitions
- Growth
- By Todd – An increase in size
- By Moyers – Quantitative aspect of biologic development per unit time
- Development
- According to Todd, development is progress towards maturity.
- Differential growth
- It means different organs grow at different rates, to different amounts, and at different times.
- Growth spurts
- A sudden increase in growth is called a growth spurt.
Growth And Development: General Principles And Concepts Important Notes
- Timings of growth spurts
- Just before birth
- One year after birth
- Mixed dentition growth spurts
- Boys – 8-11 years
- Girls – 7-9 years
- Pre-pubertal growth curve
- Boys- 14-16 years
- Girls – 11-13 years
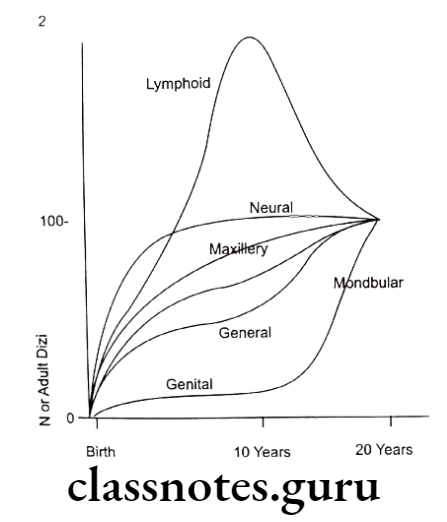
- Scammon’s growth curve
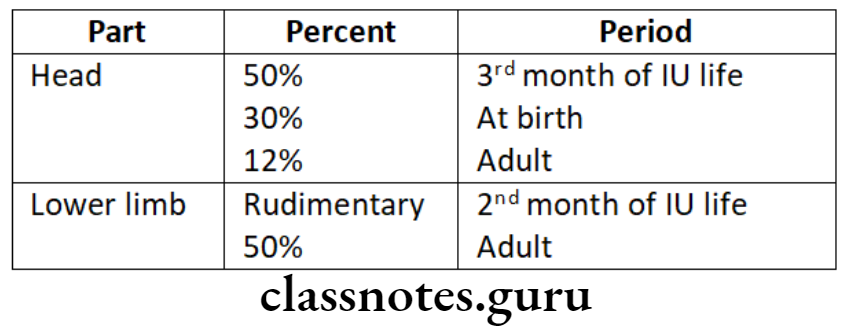
- Cephalo casual gradient of growth
- Growth of head
- During the third month of intrauterine life – 50% of the total body length
- At birth – 30% of total body length
- During adulthood – 12% of total body length
- Growth of lower limbs
- During the second month of intrauterine life – rudimentary
- During adulthood – 50% of body length
- Radio isotopes used for the study of growth are technetium 33, calcium 45, and potassium 32.
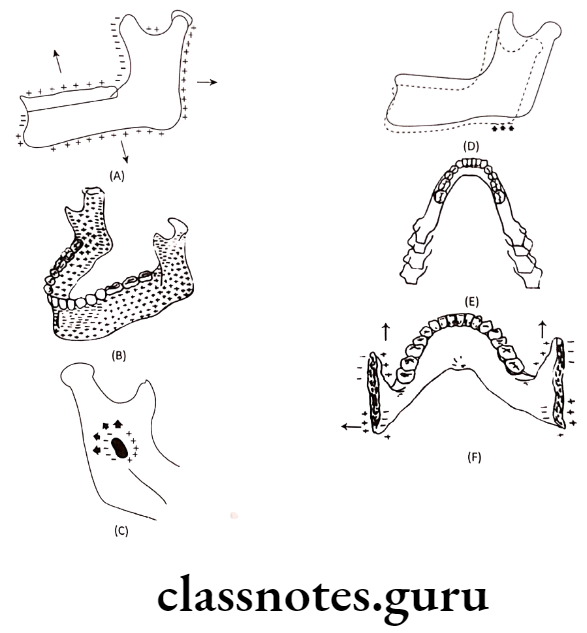
- Drift and displacement
- Drift
- The combination of deposition and resorption occurring in different bones of the skull resulting in growth movement towards the depositary surface is called drift.
- Displacement – It is the movement of whole bone as a unit
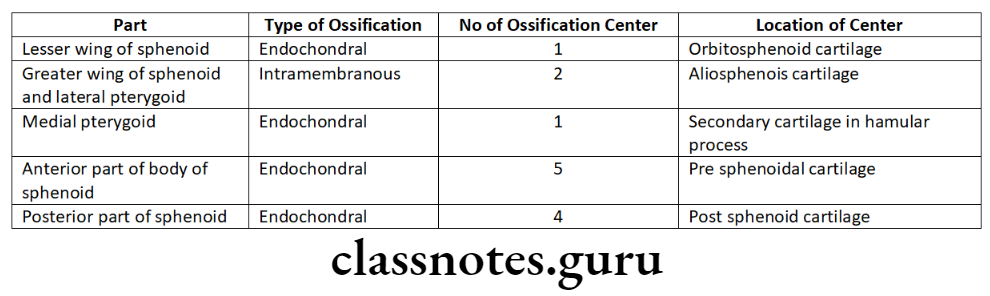
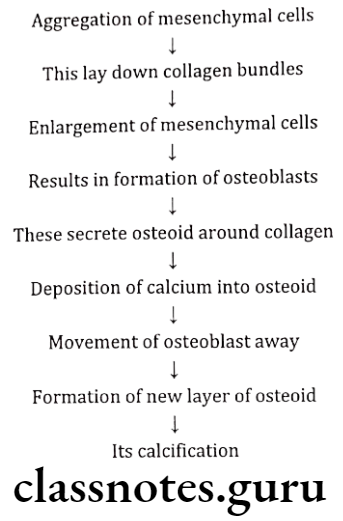
- Bone formation
- Endochondral bone formation
- Intra-membranous bone formation
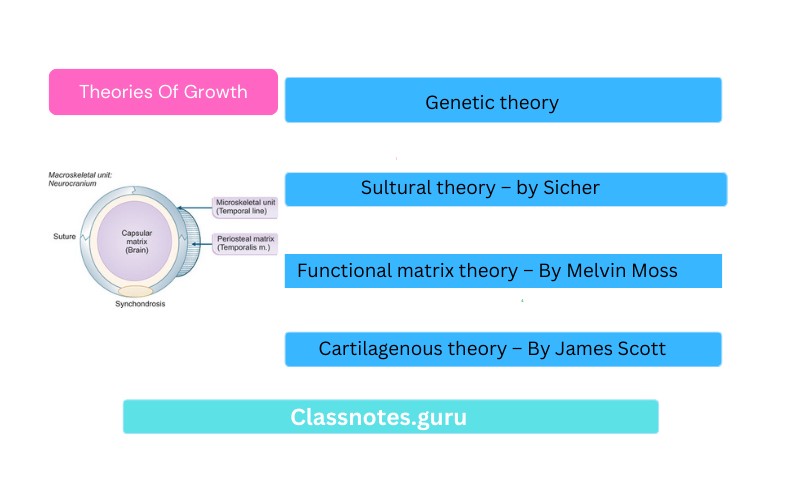
- Theories of growth
- Genetic theory
- Sutural theory – by Sicher
- Cartilaginous theory – By James Scott
Read And Learn More: Orthodontics Short And Long Essay Question And Answers
- Functional matrix theory – By Melvin Moss
- Van Limborgh’s theory – By Von Limborgh
- Functional matrices
- Functional matrix:
- Consists of muscle, glands, nerves, vessels, fat, teeth, and functional spaces
- Divided into
- Periosteal matrices
- Capsular matrices
- Acts indirectly and passively on bone
- Expansion of capsule
- Results growth of bones within it
Ex: Growth of facial bones due to expansion of oro-facial capsule
Growth And Development: General Principles And Concepts Long Essays
Question 1. Enumerate theories of growth explain functional matrix theory
Answer.
Growth:
It is defined as
- By Todd – An increase in size
- By Moyers – Quantitative aspect of biologic development per unit time
- By Meridith – Entire series of sequential anatomic and physiologic changes taking place from the beginning of prenatal life to senility
Theories Of Growth:
- Genetic theory
- Cultural theory – by Sicher
- Cartilaginous theory – By James Scott
- Functional matrix theory – By Melvin Moss
- Van Limborgh’s theory – By Von Limborgh
Functional Matrix Concept:
- Melvin Moss combined sutural theory and cartilaginous theory and introduced this concept
Hypothesis:
- It claims that the origin, form position, growth and maintenance of all skeletal tissues and organs are always secondary, compen-satory and necessary responses to chronologically and morphologically prior events or processes that occur in specifically related non-skeletal tissues, organs or functioning spaces
Components Of Growth:
- Skeletal Unit:
- Microskeletal
- Macroskeletal
- Functional Matrix:
- Periosteal Matrices
- It includes muscles, blood vessels, nerves and glands
- Capsular Matrices
- It includes neurocranial capsule and orofacial capsule
- Neurocranial capsule is made up of skin, connective tissue, aponeuritic tissue, loose connective tissue, periosteum and two layers of duramater
- Orofacial capsule surrounds and protects the oro-nosopharyngeal spaces which constitutes the orofical capsular matrix
Skeletal Unit:
- All skeletal tissues associated with a single function are called the skeletal unit
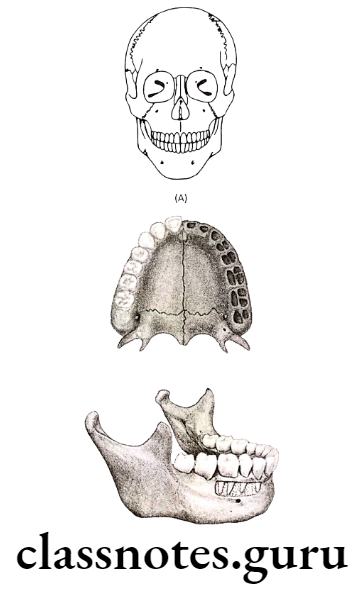
- When a bone is comprised of several contagious skeletal units, it is termed as “Micro skeletal units” Ex. Maxilla, Mandible
- When adjoining portions of a number of neighbouring bones are united to function as a single cranial component, termed as “macro skeletal unit” Ex. Calvarium
Functional Matrix:
- Consists of muscle, glands, nerves, vessels, fat, teeth and functional spaces
- Divided into
Periosteal matrices:
Capsular matrices:
- Acts indirectly and passively on bone
- Expansion of capsule
- Results growth of bones within it
Ex: Growth of facial bones due to expansion of oro-facial capsule
Growth And Development: General Principles And Concepts Short Essays
Question 1. Clinical application of growth and development.
Answer.
Clinical Application Of Growth And Development Includes:
- Growth Pattern:
- It can be defined as proportional relationship over time
- The patterns are controlling or restricting mechanisms to preserve the integration of parts of the body under varying conditions
- Differential growth:
- It means different organs grow at different rates, to a different amount and at different times.
- It is explained by two concepts namely – Scammon’s growth curve and Cephalocaudal gradient of growth
Scammon’s growth curve:
- It explains the growth of four different tissues – Lymphoid tissue, neural tissue, general tissue and genital tissue
Cephalocaudal gradient of growth:
- Represents axis of increased growth extending from head towards feet
Variability of growth:
- No two individuals are alike
- No two individuals grow in the same pattern
- Causes for it are
- Hereditary
- Nutrition
- Racial differences
- Climate
- Exercise
- Socioeconomic class
- Psychological factors
- Size of family
- Hormonal changes
- Sex differences
- Growth spurts
- Timing variation in growth:
- Growth does not take place uniformly at all times
- There are certain periods when a sudden acceleration of growth occurs
- This sudden increase in growth is termed as growth spurt
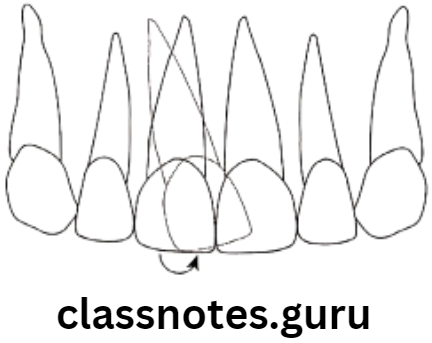
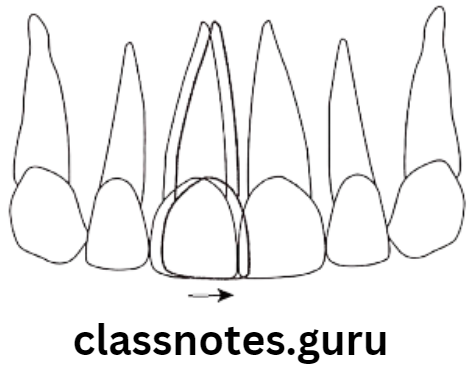
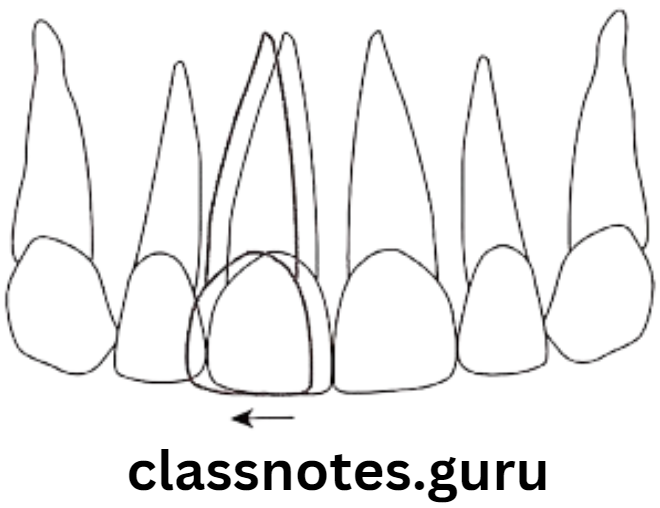
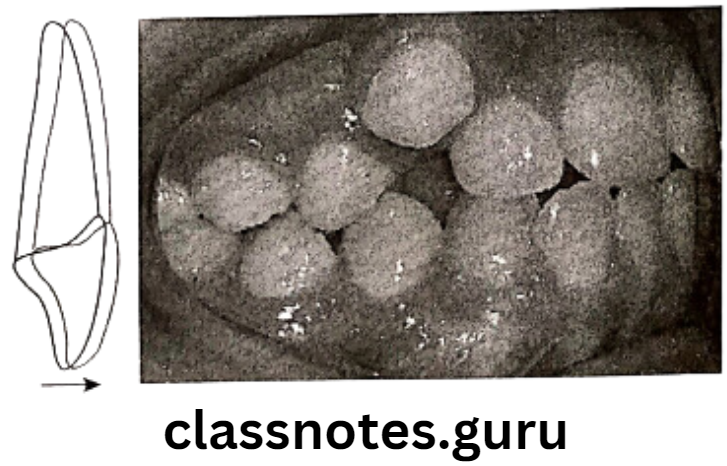
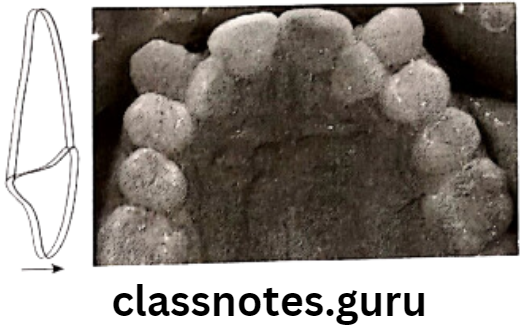
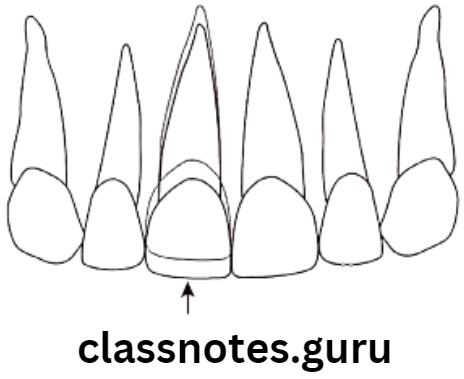
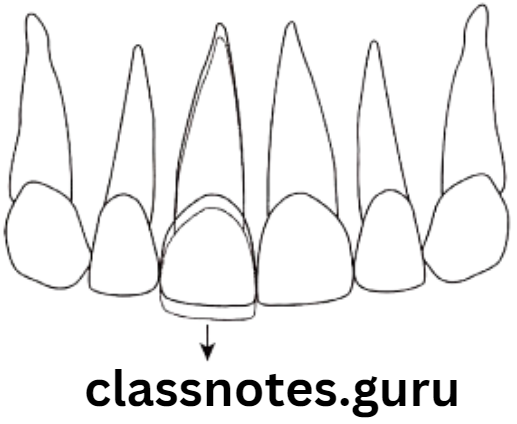
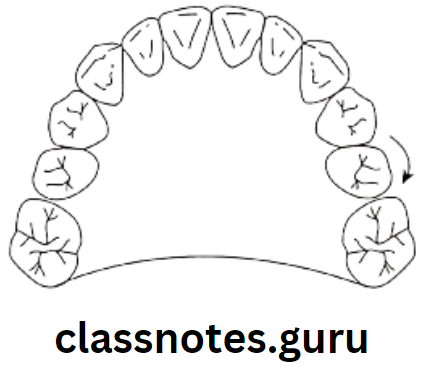
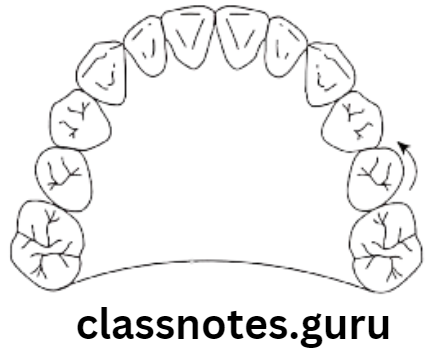
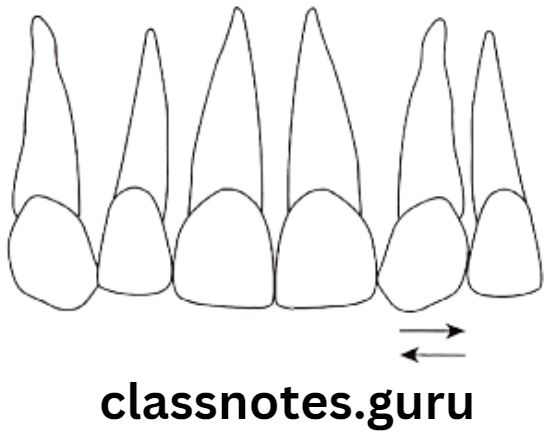
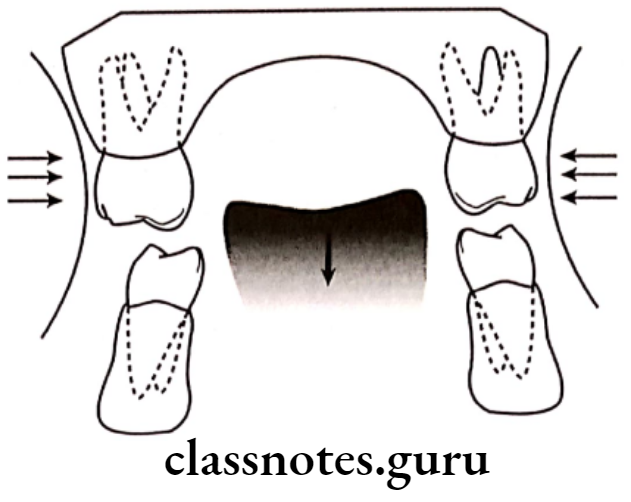
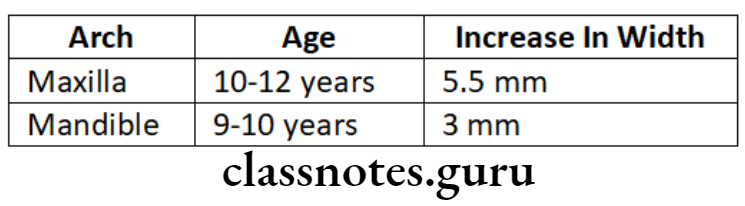
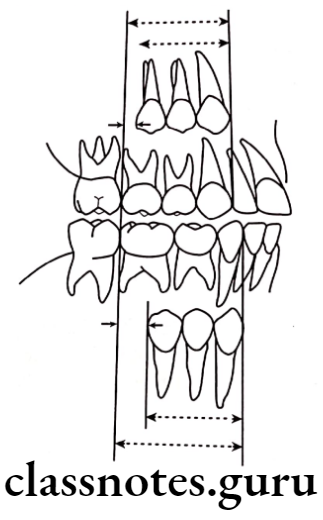
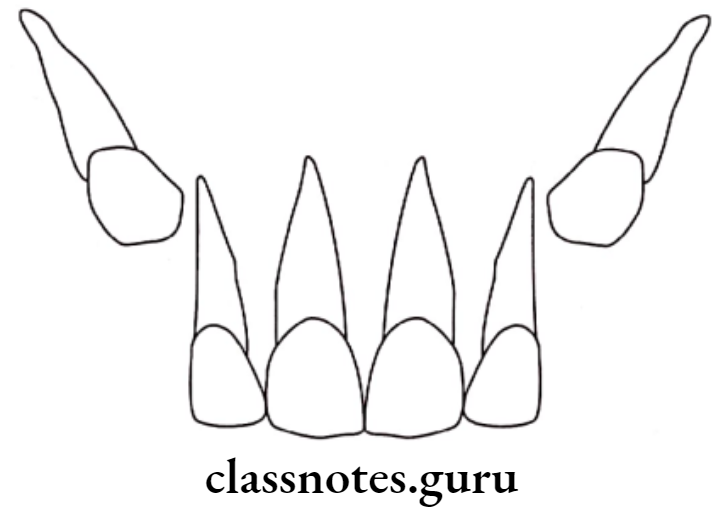
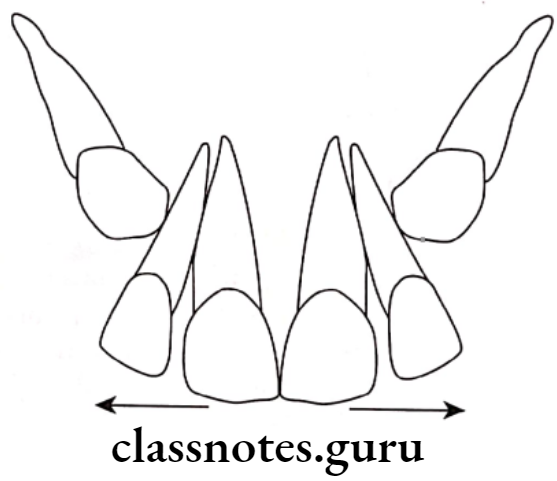
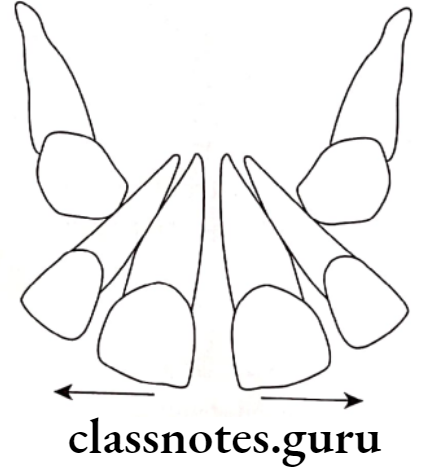
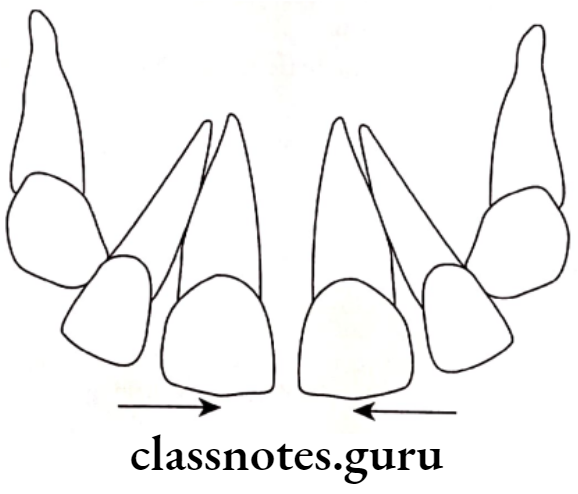
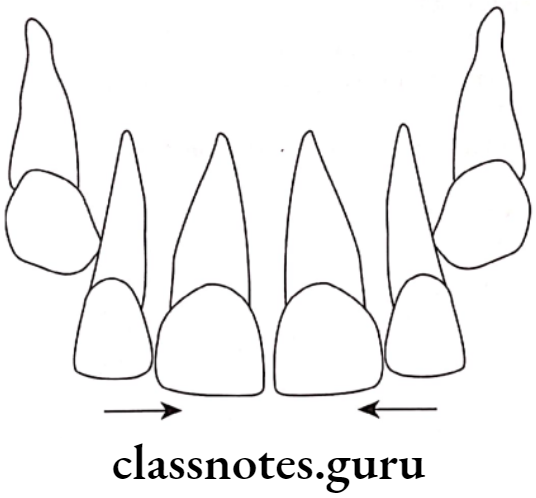
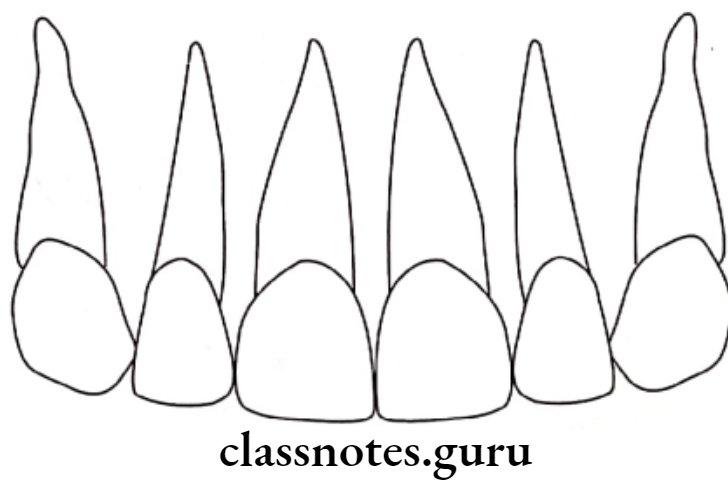
- Safety valve mechanism:
- It is maintain proper occlusion
- To compensate for the horizontal growth in mandible, the maxillary intercanine width serves as safety value
Question 2. Growth spurts.
Answer.
A sudden increase in growth is called growth spurts
Causes Of Growth Spurts:
Timings:
Just before birth:
- One year after birth
- Mixed dentition stage
- Boys – 8-11 years
- Girls – 7-9 years
- Pre-pubertal growth spurts
- Boys – 14-16 years
- Girls – 11-13 years
Significance Of Growth Spurts:
- Differs in boys and girls
- Effects the treatment planning
- During growth spurts – Myofunctional appliances are used
- After cessation of growth spurts – urgical correction
- During pubertal growth spurts there is change in growth direction form vertical to horizontal
- Periods of maximum growth are suitable for arch expansion and rapid skeletal expansion procedures
- Growth spurt period is best time for interceptive orthodontic procedures
Question 3. Micro-implants.
Answer.
- Introduced by Bjork in 1969
- Involves implanting inert alloys into growing bone
- Radiographs are taken
Size Of Implants:
- 1.5mm in length
- 0.5mm in diameter
Material:
Sizes In Maxilla:
- Behind deciduous canines
- Below anterior nasal spine
- Two on either side of zygomatic process
- Border between hard palate and alveolar process medial to first molar
Sites In Mandible:
- Anterior aspect of symphysis
- Two pins on right side of body
- One pin on external aspect of right ramus at the level of occlusal surface
Question 4. Differential growth.
Answer.
Differential Growth:
It means different organs grow at different rates, to a different amount and at different times.
Concepts:
Scammon’s growth curve:
- It explains the growth of four different tissues
Lymphoid tissue:
- Childhood – 20% of adult size
- Adult – Involution
- Significance – Increase during childhood helps to adapt for protection against infections
Neural tissue:
- 6-7 years – Adult size
- After – Little growth
- Significance – Facilities intake of further knowledge
General tissue:
- Until puberty – negligible growth
- At puberty – grow rapidly
Cephal – Caudal growth curve:
- Represents axis of increased growth extending from head towards feet
Examples:
Question 5. Methods of Studying growth.
Answer.
- Approaches:
- Measurement: Carried on humans
- Experimental: Carried on animals
- Experiments:
- Biometric test:
- Standard measurements regarding height, weight, ossification are compared
- Vital staining:
- By Belchier
- He identified alizarin from madden plants and used it for research
Technique:
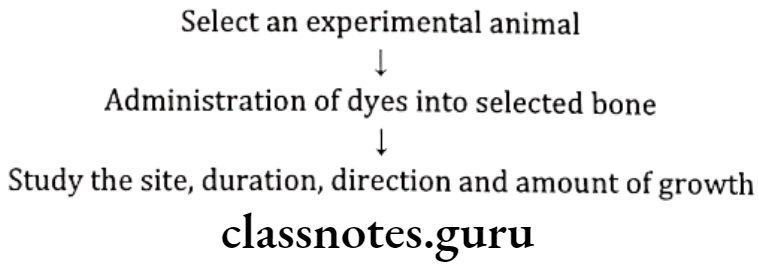
Dyes used:
- Alizarin red 5
- Acid Alizarin Blue
- Trypon Blue
- Tetracycline
- Lead acetate
Radioisotope:
- Inject radiosotope into tissue
- This gets incorporated into bone
- Act as vivo markers
Used:
- Technetium – 33
- Calcium – 45
- Potassium – 32
Implants:
- Introduced by Bjork in 1969
- Involves implanting inert alloys into growing bone
- Radiographs are taken
Size of implants:
- 1.5mm in length
- 0.5mm in diameter
Material:
Sites in Maxilla:
- Behind deciduous canines
- Below anterior nasal spine
- Two on either side of zygomatic process
- Border between hard palate and alveolar process medial to first molar
Sites in mandible:
- Anterior aspect of symphysis
- Two pins on right side of body
- One pin on external aspect of right ramus at the level of occlusal surface
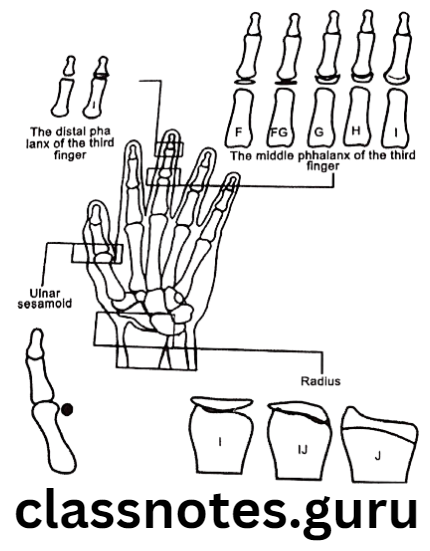
Radiographic techniques:
- Radiographs used
- Cephalometry
- Hand wrist
Natural Markers:
- Nutrient canals, lines of arrested growth and prominent trabeculae these are considered as natural markers
Use: To study bone deposition, resorption and bone remodeling
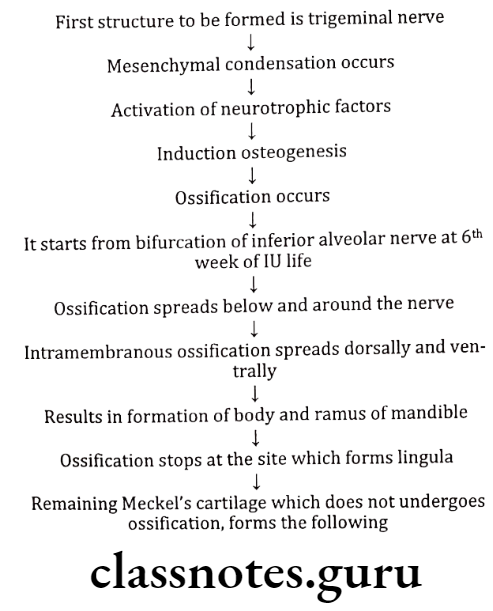
Question 6. Osteogenesis.
Answer.
It is the process of bone formation
Types Of Bone Formation:
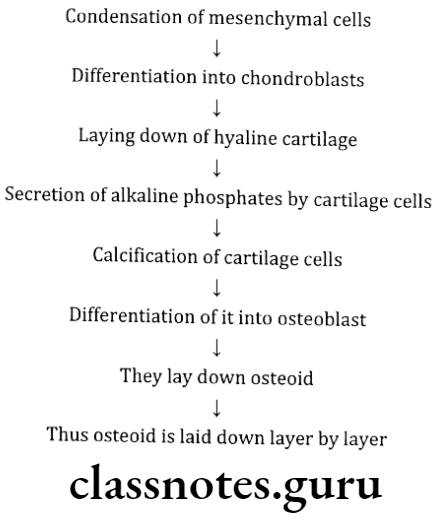
Endochondral bone formation:
Intra-membranous bone formation:
Question 7. Enumerate theories of growth explain functional matrix theory.
Answer.
Theories Of Growth:
- Genetic theory
- Sutural theory – by Sicher
- Cartilagenous theory – By James Scott
- Fuctional matrix theory – By Melvin Moss
- Van Limborgh’s theory – By Von Limborgh
Functional Matrix Concept
- Melvin Moss combined sutural theory and cartilaginous theory and introduced this concept
Hypothesis:
- It claims that the origin, form, position, growth and maintenance of all skeletal tissues and organs are always secondary, compensatory and necessary responses to chronologically and morphologically prior events or processes that occur in specifically related non-skeletal tissues, organs or functioning spaces
Components Of Hypothesis:
- Skeletal unit:
- Microskeletal
- Mactroskeletal
- Functional Matrix:
- Periosteal Matrices
- Capsular Matrices
Skeletal Unit:
- All skeletal tissues associated with a single function are called the skeletal unit
- When a bone is comprised of several cotagious skeletal units, it is termed as “Micro skeletal units” Ex. Maxilla, Mandible
- When adjoining portions of a number of neighbouring bones are united to function as a single cranial component, termed as “Macro skeletal unit” Ex. Calvarium
Functional Matrix:
- Consists of muscle, glands, nerves, vessels, fat, teeth and functional spaces
- Divided into
Periosteal matrices:
Capsular matrices:
- Acts indirectly and passively on bone
- Expansion of capsule
- Results growth of bones within it
Ex. Growth of facial bones due to expansion of oro-facial capsule
Question 8. Van Limborgh’s Theory.
Answer.
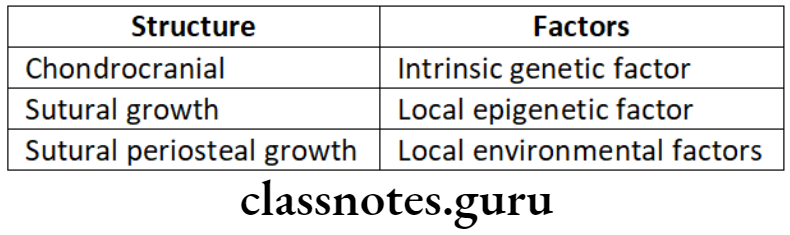
- By Van Limborgh in 1970
- He combines all the three existing theories
- He supports the functinal matrix theory of Moss, some aspects of Sicher’s theory and genetic theory
- He suggested 5 factors to control growth
Intrinsic Genetic factors: Genetic control of the skeletal units
Local Epigenetic factors: Genetic control originating from adjacent structures
General Epigenetic factors: Genetic control originating from distant structures
Local Environmental factors: Non-genetic factors from local external environment
General Environmental factors: General non-genetic influences
Examples:
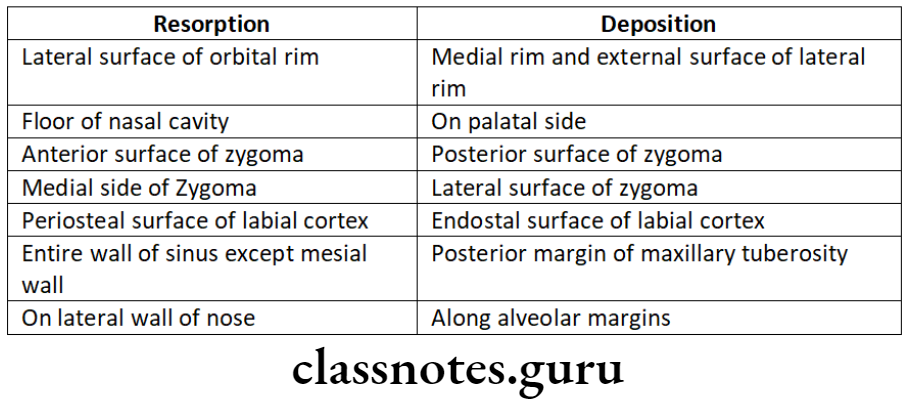
Question 9. Enlow’s principle.
Answer.
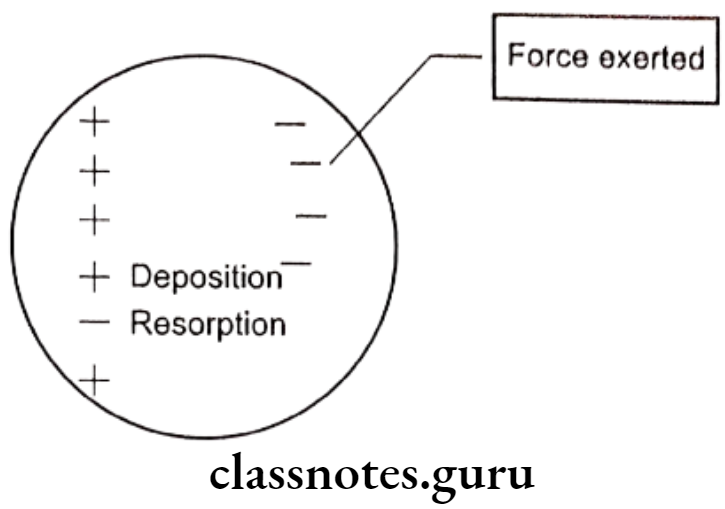
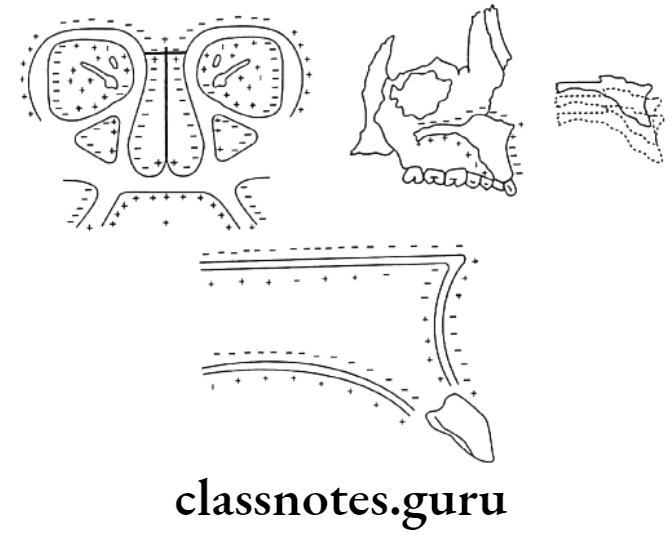
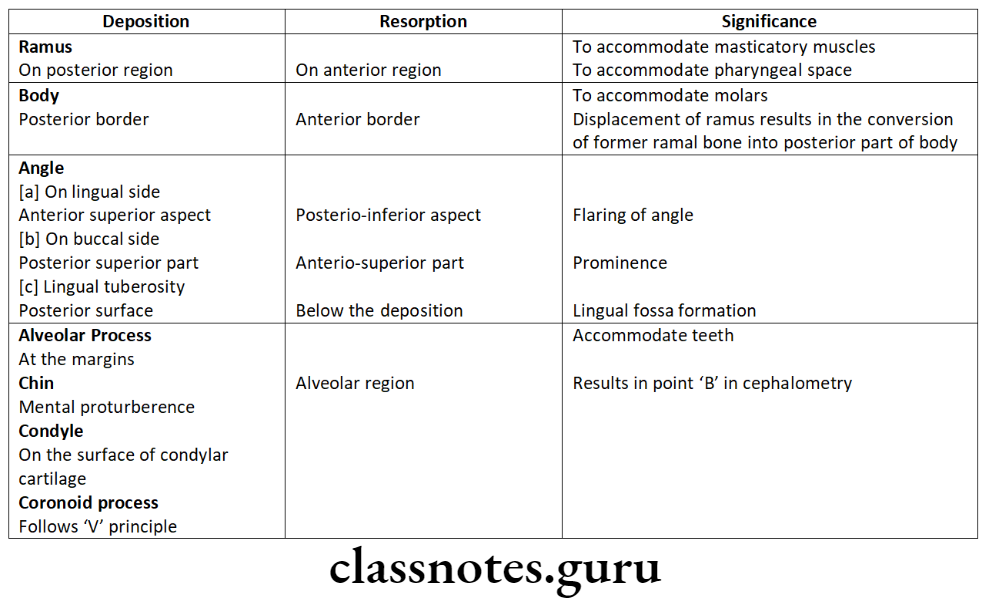
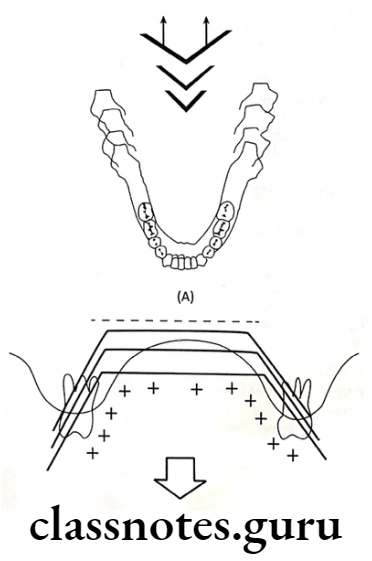
Enlow’s expanding V principle:
- Explains bone remodeling of facial bones
- Growth and enlargement of bones occurs as a result of selective deposition and resorption
Deposition: Inner side of wide end of ‘V’
- At the ends of arms of ‘V’
Resorption: On the outer surface
Regions: Base of mandible
- Ends of long bone
- Mandibular body, palate etc,
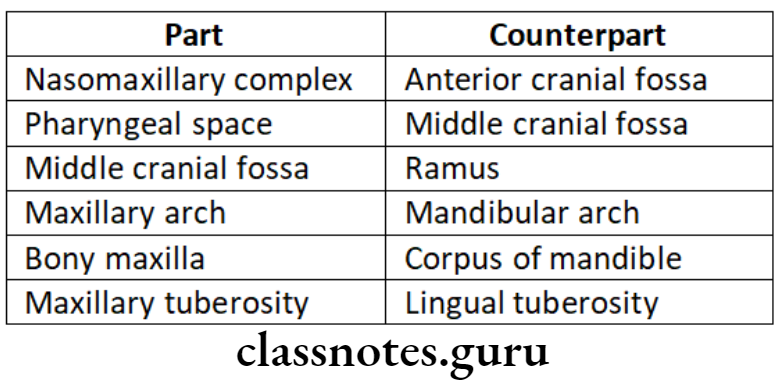
Enlow’s Counter part principle:
- It states that the growth of any given facial or cranial part relates specifically to other structural and geometric counter part in the face and cranium
- If each regional part and its particular counter part enlarge to the same extent, balanced growth occurs.
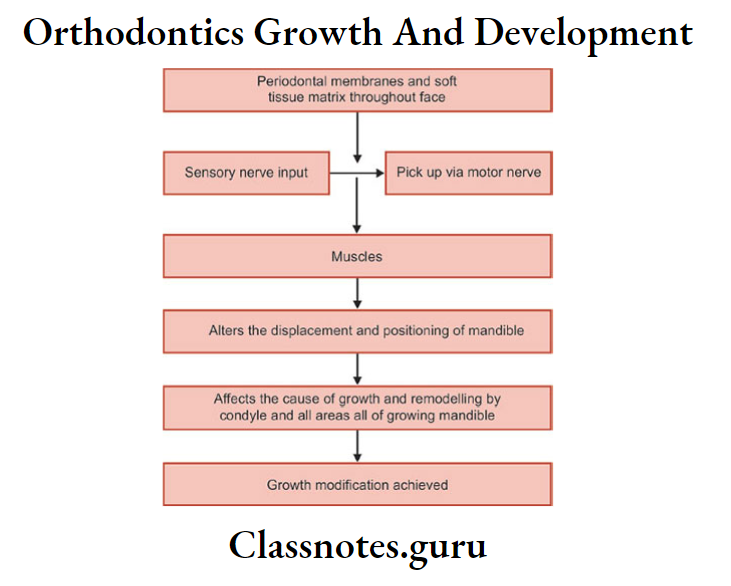
Question 10. Neutrophism/Neurotrophic theory.
Answer.
It is a non-impulse transmitting neural function that involves axoplasmic transport and provides for long term interaction between neurons and innervated tissues that homeostatically regulates the morphological compositional and functional integrity of tissues.
Types Of Neurotrophic theory:
Neuro-epithelial trophism:
Neuro muscular trophism: At the myoblastic stage of differentiation, neural innervations is established
Neuro-Visceral trophism: Salivary glands, fat tissue and other organs are trophically regulated
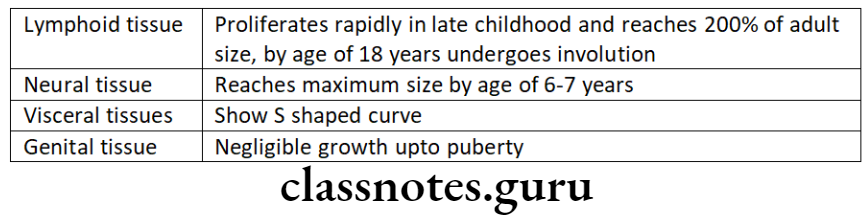
Question 11. Scammon’s Growth Curve.
Answer.
It explains the growth of four different tissues
Lymphoid Tissue:
- Childhood – 20% of adult size
- Adult – Involution
- Significance – Increase during childhood helps to addapt for protection against infections
Neural Tissue:
- 6-7 years – Adult size
- After – Little growth
- Significance – Facilities in take of further knowledge
General Tissue:
- Exhibits ‘S’ shaped curve
- 2-3 years – rapid growth
- 3-10 years – slow growth
- Upto 18-20 years – rapid growth
General Tissue:
- Until puberty – negligible growth
- At puberty – grow rapidly
Question 12. Functional matrix theory
Answer.
Functional Matrix Concept:
- Melvin Moss combined sutural theory and cartilaginous theory and introduced this concept
Hypothesis:
- It claims that the origin, form, position, growth and maintenance of all skeletal tissues and organs are always secondary, compensatory and necessary responses to chronologically and morphologically prior events or processes that occur in specifically related non-skeletal tissues, organs or functioning spaces
Components Of Functional matrix:
- Skeletal Unit:
- Microskeletal
- Macroskeletal
- Functional Matrix:
- Periosteal Matrices
- Capsular Matrices
Skeletal Unit:
- All skeletal tissues associated with a single function are called the skeletal unit
- When a bone is comprised of several contagious skeletal units, it is termed as “Micro skeletal units”
- When adjoining portions of a number of neighbouring bones are united to function as a single cranial component, termed as “Macro skeletal unit” Ex. Calvarium
Functional Matrix:
- Consists of muscle, glands, nerves, vessels, fat, teeth and functional spaces
- Divided into
Periosteal matrices:
Capsular matrices:
- Acts indirectly and passively on bone
- Expansion of capsule
- Results growth of bones with in it
Ex. Growth of facial bones due to expansion of oro-facial capsule
Question 13. Cartilaginous theory of growth.
Answer.
- Cartilaginous theory was put forward by James Scott
- According to him intrinsic growth factors are present in cartilage and periosteum with sutures being secondary
- Nasal septal cartilage is considered to be pacemaker for the growth of entire naso-maxillary complex
- Mandible is considered as diaphysis of long bone
- This theory was supported due to following observations:
- In many bones cartilage growth replaces bone
- If a part of an epiphyseal plate is transplated to a different location it will continue to grow in the new location
- Nasal septal cartilage shows innate potential of growth
- In rabbits removal of nasal septal cartilage showed retarded mid face development
Growth And Development: General Principles And Concepts Short Questions And Answers
Question 1. Neurotrophic theory.
Answer.
It is a non-impulse transmitting neural function that involves axoplasmic transport and provides for long term interation between neurons and innervated tissues that homeostatically regulates the morpho-logical compositional and functional integrity of tissues.
Types Of Neurotrophic:
- Neuro-epithelial trophism
- Neuro-muscular trophism
- Neuro-Visceral trophism
Question 2. Define Growth.
Answer.
- An increase in size – Todd
- Entire series of sequential anatomic and physiologic changes taking place from the beginning of prenatal life to seenlity – By Meridith
Question 3. Development.
Answer.
Development is progress towards maturity.
According To Todd:
- According to Moyers, development refers to all the naturally occuring unidirectional changes in the life of individual from its existence as a single cell to its elaboration as a multi functional unit terminating in death.
Question 4. Enumerate factors effecting growth.
Answer.
- Hereditary
- Nutrition
- Illness
- Race
- Socio-economic
- Family size and birth order
- Secular trends
- Climatic and seasonal effects
- Psychological disturbances
- Exercise
Question 5. Natural markers.
Answer.
Nutrient canals, lines of arrested growth and prominent trabeculae these are considered as natural markers
Uses of Natural markers: To study bone deposition, resorption and bone remodeling
Question 6. Enumerate theories of growth.
Answer.
Theories Of Growth.
- Genetic theory
- Sutural theory – by Sicher
- Cartilagenous theory – By James Scott
- Functional matrix theory – By Melvin Moss
- Van Limborgh’s theory – By Von Limborgh
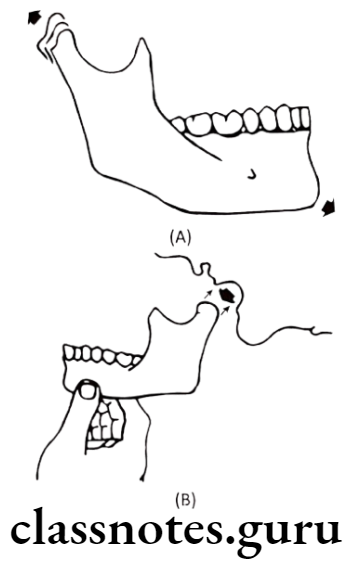
Question 7. Displacement.
Answer.
It is the movement of the whole bone as a unit
Types Of Displacement:
Primary Displacement:
- When bone gets displaced as a result of its own growth
Ex. Displacement of maxilla due to growth at its tuberosity region
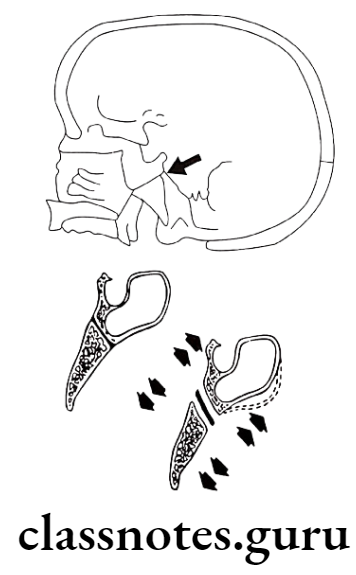
Secondary Displacement:
- When bone gets displaced as a result of growth and enlargement of its adjacent bone
Ex. Displacement of maxilla due to growth of cranial base
Question 8. Differential growth.
Answer.
- It means different organs grow at different rates, to a different amount and at different times.
- It is explained by two concepts namely – Scammon’s growth curve and Cephalocaudal gradient of growth
- Scammon’s growth curve
- It explains the growth of four different tissues Lymphoid tissue, neural tissue, general tissue and genital tissue
- Cephalocaudual gradient of growth
Growth And Development: General Principles And Concepts Viva Voce
- In Scammon’s growth curve, S shaped curve indicates growth of muscles and bone tissues, genital tissues shows negligible growth upto puberty.
- Implants and vital staining techniques are used to study dynamic changes of growth, radiographs shows static changes
- Arthropometry is the measurement of skeletal dimensions on living individuals
- The adult human body contains 206 bones, 33 vertebrae, 12 pairs of cranial nerves, 31 pairs of spinal nerves, 12 pairs of rib.
- Stains used in vital staining are Alizarin, trypton blue, tetracycline, lead acetate.