
- Sterilisation and Infection Control Question and Answers
- Isolation Question and Answers
- Instruments Question and Answers
- Separation Question and Answers
- Matricing Question and Answers
- Dental Caries Question and Answers
- Pulp Protection Question and Answers
- Fundamentals of Cavity Preparation Question and Answers
- Amalgam Question and Answers
- Pin-Retained Restoration Question and Answers
- Direct Filling Gold Question and Answers
- Cast Metal Restorations Question and Answers
- Composite Restoration Question and Answers
- Glass Ionomer Cement Question and Answers
- Veneers Question and Answers
- Ceramics Question and Answers
- Bonding Question and Answers
- Non-Carious Lesion Question and Answers
- Dentinal Hypersensitivity Question and Answers
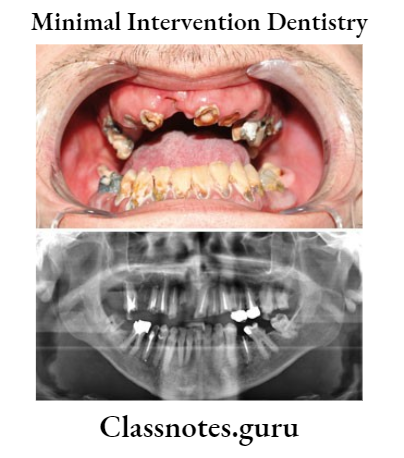
- Minimal Intervention Dentistry Question and Answers
- Conservative and Operative Dentistry Miscellaneous Question and Answers
Operative Dentistry
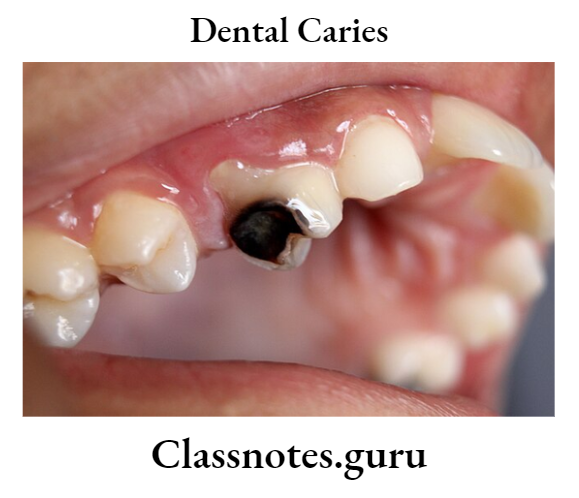
Dental Caries Question And Answers
Dental Caries Important Notes
1. Types Of Caries
- Pit And Fissure Caries
- It occurs in pits and fissures
- It is represented as a cone with a base towards DEJ and an apex towards the enamel surface
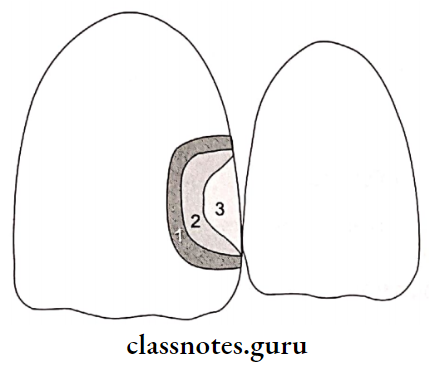
- Smooth Surface Caries
- It occurs in the unclean proximal surfaces
- The base of the cone is towards the enamel surface and the apex is towards the DEJ
- Residual Caries
- It is caries that remains in a completed cavity preparation by the operator intentionally or unintentionally
- Forward Caries
- When the caries cone in enamel is larger than that of dentin
- Backward Caries
- When the spread of caries along the DEJ exceeds caries in contagious enamel and caries extends into the enamel from DEJ
- Root/Senile Caries
- Occurs on the tooth that has been exposed to the oral environment
- Recurrent/Secondary Caries
- It occurs at the borders or underneath the restorations
- Acute/rampant caries
- The lesion is light-colored and infectious
- Chronic/Slow-Caries
- The lesion is discolored and fairly hard
2. Composition Of GIC
Powder:
- Silica 3540%
- Alumina 2030%
- Aluminum fluoride 1.52.5%
- Calcium and sodium fluorides 2025%
- Lanthanum, strontium, and barium in traces
Liquid:
- Polyacrylic acid 45%
- Water50%
- Itaconic acid, maleic acid, tricarballyic acid 5%
- Tartaric acid traces
3. Accelerators And Retarders Of ZOE Cement
Read And Learn More: Operative Dentistry Short And Long Essay Question And Answers
Accelerators
- Zinc acetate
- Alcohol
- Water
- Glacial acetic add
Retarders
- Cooling of glass slab
- Glycerine
- Olive oil
- Increasing liquid powder ratio
4. Hybrid or Resin-Modified GIC
- BISGMA and TEGDMA are added to GIC powder and HEMA to liquid
- They are usually light-cured, less technique-sensitive, and may be finished at the time of placement
- The properties are superior to GIC
- They are recommended for class V restorations and class I and II in primary teeth
5. Compomer
- Compomer is a combination of composite and GIC
- Glass particles are partially silanated and are added as fillers in the composite resin
- There is no water in the reaction
- The properties are inferior to composites but superior to GIC and resin-modified GIC
6. Cermet
- Glass and metal powders were sintered at high temperatures and made to react with liquid
- Cermet improves fracture toughness and wear resistance and maintains aesthetics
7. Sandwich or bilayered restorations
- Sandwich uses GIC as a liner under composite restoration
- Sandwich increases the retention form as GIC bonds to the tooth and the composite
- Fluoride content reduces secondary caries.
Dental Caries Long Essay
Question 1. Enumerate various tooth-colored restorative materials. Give manipulation, indication, and advantage of silicate.
Answer:
Various Tooth-Colored Restorative Materials:
Restorative Materials:
- Glass ionomers
- Composites
- Fused porcelain
- Acrylic resins
- Silicate cement
Various Tooth-Colored Restorative Materials Manipulation:
- Powder/liquid ratio 1.6g/4ml
- Dispensed on a thick, cool, dry glass slab
- Divide it in 2/3 increments
- Mix with agate spatula in a folded manner to obtain a homogenous mass
- Mixing time 1 minute
Various Tooth-Colored Restorative Materials Indications:
- For anterior restoration
Various Tooth-Colored Restorative Materials Advantages:
- An anti-cariogenic property
- Tooth color matching ability
- Ease of manipulation
- The coefficient of thermal expansion is approximately similar to enamel
- Good insulator
- Its compressive strength is higher than other cement
Dental Caries Short Answers
Question 1. Buccal Object Rule/Slob/Clark’s rule.
Answer:
Buccal Object Rule:
- A standard radiograph is taken
- Shift the cone medially/distally
- Take a second radiograph
- If the object is seen on the same side, the object is placed over the lingual side
- For object localization
Question 2. Caries detecting dyes.
Answer:
1. Dyes For Enamel Caries:
- Procion Staining is irreversible
- Reacts with nitrogen and hydroxyl groups
- Calcein Bounds with calcium
- Zyglo ZL22 Visible by UV illumination
2. Dyes For Dentin Caries:
- Infected and affected dentin layers are present
- Basic Fuschia in propylene glycol stains only the infected dentin
Dental Caries Viva Voce
- Double inverted cone type of penetration of dental caries is seen in smooth surface caries
- Pit and fissure lesions are represented by the base of the cone facing each other
- The cervical to-contact area is the common site for proximal caries
- Smooth surface caries is mainly caused by streptococcus mutans
- Patients with salivary levels of streptococcus mutans above 106 CFU/ml are considered at high risk for dental caries
- Remineralization of carious lesions occurs at a pH above 5.5
- Streptococcus mutants and lactobacillus are most strongly associated with the onset of caries and active progression of cavitated lesions
- Root caries is initiated by A.viscosus
- The surface zone of enamel caries is unaffected by caries attack
- The Dentinoenamel junction is the least resistant to caries
- Increased powder in zinc phosphate cement decreases the setting time and solubility and increases strength and film thickness
- Zinc polycarboxylate is the first cement to show adhesion with tooth structure
- pH of zinc polycarboxylate liquid is 1.7
- Mechanical properties of ZOE cement can be improved by adding alumina to the powder and orthodoxy benzoic acid to the liquid
- GIC lacks toughness, and wear resistance and cannot withstand high stress
- ZOE and silicate cement have high solubility and disintegration rate
- GIC and silicophosphate have low solubility
- Resin cement is the least soluble in the oral cavity
- The working time of zinc polycarboxylate is 25 min
- The working time of zinc phosphate is 5 min.
Operative Dentistry
- Sterilisation And Infection Control Short And Long Essay Question And Answers
- Operative Dentistry Separation Short And Long Essay Question And Answers
- Matricing Operative Dentistry Question And Answers
- Bacterial Infections Operative Dentistry Short And Long Essay Question And Answers
- Pulp Protection Question And Answers
- Fundamentals Of Cavity Preparation Question And Answers
- Amalgam Operative Dentistry Question And Answers
- Pin Retained Restoration Operative Dentistry Short And Long Essay Question And Answers
- Operative Dentistry Direct Filling Gold Short And Long Essay Question And Answers

- Isolation Operative Dentistry Short And Long Essay Question And Answers
- Cast Metal Restorations Question And Answers
- Glass Ionomer Cement Short And Long Essay Question And Answers
- Ceramics Short And Long Essay Question And Answers
- Bonding Short And Long Essay Question And Answers
- Veneers Short And Long Essay Question And Answers
- Non-Carious Lesion Short And Long Essay Question And Answers
- Dentinal Hypersensitivity Question And Answers
- Minimal Intervention Dentistry Question And Answers
- Composite Restoration Question And Answers
- Dental Caries Question And Answers
- Operative Dentistry Miscellaneous Short And Long Essay Question And Answers
Operative Dentistry Miscellaneous Short And Long Essay Question And Answers
Miscellaneous Long Essays
Question 1. Discuss various restorative materials used to restore Class 2.
Answer:
Various Restorative Materials Used To Restore Class 2:
Various Restorative Materials Used To Restore Class 2 Materials Used:
- Composites
- Amalgam
- Direct filling gold
- Metal inlay
1. Composite:
Composite Definition:
- Composite is a compound composed of at least two different materials with properties that are superior or intermediate to those of an individual component
Composition:
- Organic matrix BisGMA or UDMA
- Fillers Silica, barium. Zinc, Zirconium
- Coupling agents organic silane
- Coloring agents Titanium oxide
- UV Absorber Benzophene
- Initiator Camphoroquinone
- Inhibitor Butylated hydroxyl toluene
Composite Properties:
- High coefficient of thermal expansion
- Composites with higher filler content exhibit lower water absorption
- Wear resistant
- Radiolucent
- Low modulus of elasticity
Read And Learn More: Operative Dentistry Short And Long Essay Question And Answers
- Water solubility 0.51.1 mg/cm2
- Polymerization shrinkage
- Esthetics
- Microleakage
- Biocompatible
2. Amalgam:
- Amalgam Composition:
- Alloy:
- Mercury
- Silver 40%
- Tin 32%
- Copper 30%
- Zinc 2%
- Indium traces
- Amalgam Mercury:
- Properties:
- Initially, a small amount of contraction followed by expansion
- Amalgam has a maximum compressive and tensile strength
- Creep It is a time-dependent response
- It leads to marginal deterioration
- Amalgam shows tarnish and corrosion
- Amalgam needs pulpal protection
- Amalgam transmits temperature changes
- It has a high coefficient of thermal expansion
- Microleakage
- Properties:
- Alloy:
3. Direct Filling Gold:
Direct Filling Gold Properties:
- Cohesiveness
- Softness during manipulation
- Malleability and ductility
- Brinell hardness number 25
- Tensile strength 19000 psi
- The coefficient of thermal expansion is 14.4 x 106/°C
- High thermal conductivity
- The density of gold is 19.3 gm/cm3
Direct Filling Gold Types:
- Gold Foil:
- Sheets
- Gold foil cylinder
- Gold pellets
- Platinized gold foil
- Corrugated foil
- Laminated foil
- Crystalline Gold:
- Mat gold
- Mat foil
- Electrically
- Powdered Gold:
4. Metal Inlay:
Metal Inlay Definition:
- Inlay is an indirect intracoronal restoration that is fabricated extra orally and cemented in the prepared tooth
Metal Inlay Advantages:
- Better reproduction of details
- More wear resistance
- Biocompatible
- Strengthen the weakened remaining structure
- Less chair side
- Less chances of voids
- Easy to polish
Metal Inlay Disadvantages:
- Require temporary restoration
- Expensive
- Technique sensitive
- Difficult to repair
- Weak bonding to tooth structure
- Unaesthetic
Miscellaneous Short Essays
Question 1. Interim restoration.
Answer:
Interim Restoration:
Objectives:
- Maintain esthetics
- Act as space maintainers
- Allow functioning
- Determine occlusion
- Establish phonetics
- Seal and insulate the prepared tooth
- Prevent passive eruption of the tooth
- Prevent pathologic migration
Interim Restoration Requirements:
- Good marginal adaptation
- Optimal strength
- Plaque resistant surface
- Economical
- Easy to manipulate
- Dimensionally stable
Interim Restoration Purpose:
- Pulp protection
- Act as a sedative
- Soft tissue protection
- Protect weakened tooth protection
- Maintain the aesthetics
Interim Restoration Materials Used:
1. For Intra coronal preparation
- Guttapercha
- Zinc oxide eugenol
- Zinc phosphate
- Zinc polycarboxylate
- Glass ionomer
- Calcium hydroxide
2. For extra coronal
- Polycarbonate crowns
- Aluminum cylinder
- Stainless steel crowns
- Celluloid crowns
- Indirect acrylic restorations
Question 2. Resin Cement.
Answer:
Resin Cement:
Resin Cement Uses:
- For cementation of inlays/onlays
- For cementation of crown and bridge
- For bonding amalgam restoration
- For cementation of orthodontic brackets
- For cementation of endodontic posts
Resin Cement Types:
- Unfilled resin cement
- Filled resin cement
Resin Cement Available Forms:
- Powder and liquid
- 2 paste system
- Single paste with accelerator
Resin Cement Composition:
- Powder:
- Resin Matrix
- B1SGMA
- TEGDMA
- Fillersilica
- Zirconia
- Coupling Agent
- Organosilane
- Initiator And Activator
- Resin Matrix
- Liquid:
- Adhesive HEMA:
- Initiator:
- Benzoyl peroxide
- Inorganic Fillers:
- Silica
- Zirconia
- Means Of Polymerisation:
- Chemical cure
- Light cure
- Dual cure
- Commercial Names:
- PanaviaEx
- RelyX
- ARC Resin cement
- Commercial Names:
- Means Of Polymerisation:
Miscellaneous Short Answers
Question 1. Temporary restorative materials.
Answer:
Temporary restorative materials:
Temporary restorative materials is restoration given to the prepared tooth for the period between tooth preparation and cementing the restoration
Temporary restorative materials Features:
- Nonirritating
- Esthetics
- Easy to clean
- Maintain periodontal health
- Adequate strength and retention
Question 2. Secondary Dentin.
Answer:
Secondary Dentin:
- Secondary dentin is formed after the completion of root formation
- The direction of dentinal tubules is more asymmetrical and complicated
- Secondary Dentin is formed at a slower rate
Question 3. Tertiary Dentin/Reparative dentin.
Answer:
Tertiary Dentin:
- Tertiary Dentin is formed as a response to external stimuli
- Tertiary Dentin is irregular, with cellular inclusions
- Its tubular pattern ranges from an irregular to a tube-lar nature
- Reparative dentin has decreased permeability
- Tertiary Dentin is formed by secondary odontoblasts which are differentiated from mesenchymal cells of the pulp
- Reparative dentin helps in the prevention of diffusion of noxious agents from the tubules
Question 4. Universal Operator position.
Answer:
Universal Operator Position:
- 11 clock is considered a universal operating position
Position:
- The dentist sits behind slightly to the right of the patient and the left arm is positioned around the patient’s head.
Universal Operator Position Advantages:
- Most areas of the mouth are accessible from this position either using direct/indirect vision
Universal Operator Position Working Areas:
- Palatal and incisal/occlusal surfaces of maxillary teeth
- Mandibular teeth
Question 5. Transillumination and Magnification.
Answer:
Transillumination:
- Used for detection of caries
- Based on the difference in the refractory index of carious and sound normal tooth
- Carious tooth appears as a dark shadow when compared with the normal tooth
Magnification:
- Devices:
- Loupes
- Surgical telescopes
- Bifocal eyeglasses
- Advantages:
- Increases visibility of the operating area
- Easy to perform the delicate procedure
- Increases operator’s efficiency
- Protects eye from injury
Question 6. Soldering.
Answer:
Soldering:
- Soldering is the process of joining two metals together by adding the third metal
- The soldered metal should have a melting point equal to or lower than the two metals
- To increase the flow of solder, flux is added to it
- However, too much of flux leads to the flowing away of solder
- This is prevented by the addition of antiflux.
Question 7. Surface Hardness.
Answer:
Surface Hardness:
- Surface Hardness is the property that is used to predict the wear resistance of a material and its ability to abrade opposing dental structures
- Various hardness tests are used to determine the hardness of different dental materials
- They are
- Brinell hardness test
- Rockwell hardness test
- Knoop hardness test
Question 8. Modulus of elasticity
Answer:
Modulus Of Elasticity Definition:
- Modulus Of Elasticity is the relative stiffness or rigidity of material within the elastic range
Modulus Of Elasticity Measurement:
- Modulus Of Elasticity is the ratio of stress to strain and is described as E
Modulus Of Elasticity Importance
- Modulus Of Elasticity indicates that the less the strain, the greater will be the stiffness
- Elastic modulus has a constant value
- Modulus Of Elasticity is not affected by the amount of plastic and elastic stress that is induced in the material
- The modulus Of Elasticity is independent of the ductility of the material
- The modulus of elasticity of enamel and dentin describes that
- Enamel is stiffer and more brittle
- Dentin is more flexible and tougher
Modulus Of Elasticity Unit
- Giganewtons per square meter (GN/ m2)
- 2326 gauge needle is used to aspirate the contents of the lesion.
Question 9. Objectives of interim restorations.
Answer:
Objectives Of Interim Restorations:
- Interim restorations are often required before the placement of a permanent restoration
- They are expected to last for only a short period
- Zinc oxide eugenol is the cement of choice for it
Objectives Of Interim Restorations Objectives:
- Arrests caries process
- Protects the teeth till they get permanently restored
- Allows pulp to heal
Question 10. Zsigmondy Palmer system
Answer:
Zsigmondy Palmer System:
- Zsigmondy Palmer System was introduced by Adolph Zsigmondy of Vienna in 1861 for permanent dentition and modified for primary dentition in 1874.
For Permanent Dentition:
- As per this system, the oral cavity is divided into four quadrants and each permanent tooth has a specific number.
- Numbering progresses posteriorly from the midline.
- The central incisor was designated as 1 ending up with 8 for the third molar.
For Primary Dentition:
- The deciduous central incisors are designated A and progress posteriorly up to the 2nd deciduous molar alphabetically designated as E.
Composite Restoration Question And Answers
Composite Restoration Important Notes
1. Composite Restoration Disadvantages
- Gap formation due to polymerization shrinkage, microleakage
- Recurrent caries
- Time-consuming
- Technique sensitive
- Exhibit greater occlusal wear
2. Composite Restoration Indications
- Class 1, 2, 3, 4, 5, and 6 restorations
- Sealants and preventive resin restorations
- Foundations or core build-ups
- Luting agent
- Temporary restoration
- Esthetic procedures
- Partial veneers
- Tooth contour modification
- Full veneer
- Diastema closures
- Periodontal splinting
3. Composite Restoration Contraindications
- When isolation is not possible
- If all the occlusal forces will be on restorations
- Restorations that extend on the root surface
- Heavy occlusal stresses
4. Curing Lights Used For Composites
- Halogen bulb combined with filter
- Blue light emitting device
- Laser curing
5. Causes Of failures Of Composites
- Incomplete caries removal
- Incomplete etching
- Defective application of bonding agent
Read And Learn More: Operative Dentistry Short And Long Essay Question And Answers
- Contamination of composite
- Improper polymerization
- Incomplete finishing and polishing
Composite Restoration Long Essays
Question 1. Define composite. Classify and write its com¬position. Describe the management of media angular fracture of upper central right incisor not involving the pulp of a patient aged 14 years.
Or
Mention indications and contraindications of composite resin. Describe the procedure of restoring a fractured incisal angle in the maxillary incisor tooth.
Or
Classify composite resins. Discuss the composi¬tion and methods to reduce the polymerization shrinkage
Answer:
Definition Of Composite:
- Composite is a compound composed of at least two different materials with properties which are superior or intermediate to those of an individual component.
Composite Classification:
1. According To The Particle Size:
- Traditional composite – 8-12 pm
- Small-sized composite – 1-5 pm
- Microfilled composite – 0.4-0.9pm
- Hybrid composite – 0.6-1 pm
2. According To Filler Particles:
- Megafilled
- Macrofilled
- Midfilled
- Minifilled
- Microfilled
- Nanofilled
3. According To The Polymerization Method:
- Self-curing
- Ultraviolet light curing
- Visible light curing
- Dual curing
Composite Composition:
- Organic Resins – BisGMA/UDMA
- Fillers – Zinc, Silicates, Aluminium, Zirconium
- Coupling Agent – Organic silane
- Coloring Agents – Titanium oxide
- Initiator – Camphor quinone
- Inhibitor – Butylated hydroxyl toluene
Composite Indications
- Restoration of Class 1, 2, 3, 4, 5, 6
- Discolored tooth
- Midline diastema cases
- Veneers and laminates
- Bonding of orthodontic appliances
- Restoration of the non-carious lesions
- Core foundation
- As indirect restoration
- For periodontal splinting
Composite Contraindication:
- Difficult to isolate the area
- Patient with high caries index and poor oral hygiene
- Extensive caries, sub-gingivally
- Lesions over the distal surface of the canine

Methods To Reduce Polymerization Shrinkage
1. By The Addition Of Fillers
- Hybrid composites shrink- 0.6-1.4%
- Microfilled composites shrink – 2-3%
2. Incremental Placement Of Composites
- Shrinkage is allowed after the placement of increment before the next increment placement
- This controls polymerization shrinkage
Restoration Of Fractured Central Incisor:
Anesthetized and isolated the tooth
↓
Selection of proper composites
↓
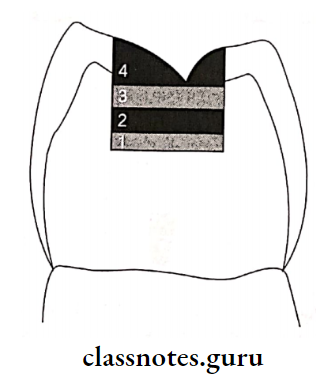
Shade selection – Done in natural daylight Dentin shade selected from
cervical 3rd Enamel shade selected from incisal 3rd
↓
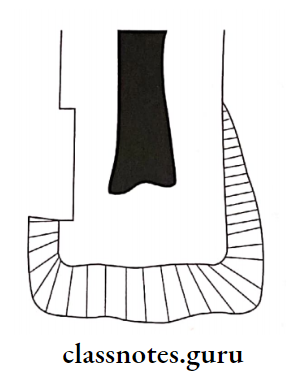
Tooth preparation
1. Enamel margins at 90°
2. Butt joint on root surfaces
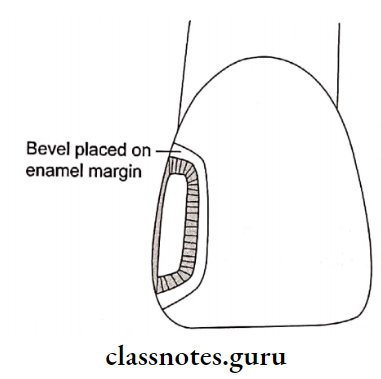
3. Enamel bevel
4. Roughening of tooth surfaces
↓
Bonding – Etching, priming and bonding with bonding
agents
↓
Composite placement – In increments along with curing
↓
Carving
1. Attain proximal contour
2. Remove excess material
↓
1. Finishing with diamond points
2. Polishing with rubber points, abrasive discs
Question 2. Enumerate various uses of composite. Describe the restoration of class 2 cavity preparation.
Or
Composite as a posterior restorative material.
Answer:
Various Uses Of Composite:
Composite Indications:
- Small, incipient lesions
- Possible to control moisture
- As core foundation
- Patient with low caries index
Composite Contra-Indications:
- Difficult to control moisture
- Extensive lesion
- High occlusal stresses
- Presence of parafunctional habits
- Patients with high caries index and poor oral hygiene
Composite Disadvantages:
- Polymerization shrinkage
- Technique sensitive
- Time-consuming
- Expensive compared to amalgam
Composite Restoration
1. Tooth Preparation
- Use small round bur, initially
- Extend preparation using fissure bur
- Maintain minimal depth
- Faciolingual dimension l/4th of intercuspal dis¬tance
- No need of retentive features
- Converging occlusal walls
- Rounded line angles
- Bevelling of enamel margin
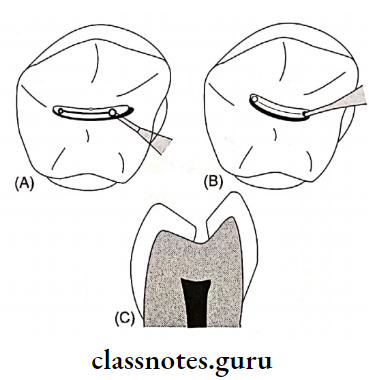
- (A) Preparation of outline usinground bur
- (B) Excavation of caries, keeping the pulpal floor shallow
- (C) Completed class I tooth preparation
2. Matrix placement in Class 2
3. Etching the preparation with 37% phosphoric acid
4. Application of primer and adhesive
5. Pulp Protection
- Use of calcium hydroxide as base
- GIC as liner
6. Composite Placement
- In increments and subsequently curing it
7. Finishing And Polishing
Composite Restoration Short Essays
Question 1. Methods of curing composites.
Answer:
Methods Of Curing Composites:
1. Tungsten Quartz Halogen Curing Unit
- It is conventional
- Uses visible light in the range of 410-500 nm
- Limited lifetime of 100 hours
- Starts curing cycle at a low power density
- Time-consuming
- Plasma arc curing unit
- Use of high-frequency electrical field
- This field ionizes xenon gas into a mixture of ions, electrons, and molecules
- Results in the release of energy in the form of plasma
- Uses 450-500 nm wavelength
- Expensive
2. Light-Emitting Diode Unit
- Have long life i.e. approximately 10,000 hours
- A wavelength of 400-500nm is used
- Suitable for composite with camphor-quinone photoinitiator
3. Argon Laser Curing Unit
- Uses a wavelength of 470 nm
- Monochromatic in nature
- Produces intensity of 200-300 mW
- May cause pulpal damage
- Has a higher degree of polymerization
Question 2. Visible Cured Composite.
Answer:
Visible Cured Composite:
Wavelength – 460-470 nm
Visible Cured Composite Mechanism:
On activation, photoinitiator combines with amine accel-
orator
↓
Release of free radicles
↓
Polymerization
Visible Cured Composite Advantage: Improved color stability
Visible Cured Composite Photoinitiator Used: Camphoroquinone
Composite Restoration Short Answers
Question 1. Packable composite.
Answer:
Packable Composite:
- The basis is Polymer Rigid Inorganic Matrix Material (PRIMM)
- Components – Resin and ceramic inorganic fillers in-corporates in a silanated network of ceramic fibers
- Filler content – 48-65% by volume
- Particle size – 0.7-20 pm
Packable Composite Indications:
- Stress bearing areas
- Class 2 restoration
Packable Composite Advantages:
- Increased wear resistance
- Better reproduction of occlusal anatomy
- The deeper depth of cure
- High flexural modulus
- Decreased polymerization shrinkage
Question 2. Failure in Composite Restoration.
Answer:
Failure In Composite Restoration:
Causes:
- Incomplete caries removal
- Incomplete etching
- Defective application of bonding agent
- Contamination of composite
- Improper polymerization
- Incomplete finishing and polishing
Failures Seen:
- Discoloration
- Marginal fracture
- Secondary caries
- Restoration fracture
- Post-operative sensitivity
- Plaque accumulation
Question 3. Fillers in Composites.
Answer:
Commonly Used Fillers:
- Silica, aluminium, zinc, barium, zirconium
- Boron silicate
Fillers Effects:
- Reduces thermal expansion
- Reduces polymerization shrinkage
- Reduces water sorption
- Increases abrasion resistance
- Increases strength
- Improves handling properties
- Increases translucency
Question 4. Microfilled Composite.
Answer:
Microfilled Composite:
- Particle size – 0.04 – 0.1 micrometer
- Filler content-35-50% by weight
Microfilled Composite Properties:
- Low modulus of elasticity
- Excellent translucency
- Low fracture toughness
- Marginal breakdown
Microfilled Composite Indication:
- Anterior teeth restoration
- Cervical abfraction lesions
Question 5. Hybrid Composite.
Answer:
Hybrid Composite:
- Made up of polymer groups reinforced by an inorganic phase
- Particle size – < 2 nm
- Filler content- 75-80% by volume
Generations Particle size (pm)
Nanofill – 0.04-0.1
Nanohybrid – 1-3
Microhybrid – 0.4-0.8
Hybrid Composite Indications:
- Posterior restoration
- Class 3, 4, and 5 restoration
- Direct veneer
- Discoloration of teeth
Question 6. Light Cured Composite.
Answer:
Light Cured Composite:
- Polymerization is towards the light source
- Material is placed in increments
Light Cured Composite Advantages:
- Adequate working time
- Good color stability
- Aesthetically good
- Less polymerization shrinkage
- More abrasion resistance
Light Cured Composite Activator Used:
- Ultraviolet – 0.1% Benzoin methyl ether
- Visible light-Camphoroquinone
Question 7. Coupling agents.
Answer:
Coupling agents Coupling Agents:
- The coupling agent bonds the filler particles to the resin matrix
- The most commonly used coupling agent are organosilanes
- In the presence of water, the methoxy group of it forms an ionic bond with the filler particle
- On the other end, methacrylate group forms a covalent bond with resin when it is polymerized
Coupling agents Functions:
- Transfers stress to filler particles
- Improves physical and mechanical properties
- Inhibits leaching by preventing water from penetrating along the filler resin interface
Question 8. Nanocomposite restoration.
Answer:
Nanocomposite Restoration:
- Nanocomposites contain filler particles that are extremely small [0.005-0.01 micrometer]
- They may be clustered or aggregated into large units that can be blended with nanoparticles to produce nanohybrids
Nanocomposite Restoration Advantages:
- Good physical properties
- Improved esthetics
- Small particle size
- Highly polishable
Question 9. Resin matrix in restorative resin
Answer:
Resin Matrix In Restorative Resin:
- Matrix of composite resin consists of BisGMA, urethane methacrylate, or TEGDMA
- Bis-GMA is a difunctional monomer produced as the reaction product of bisphenol*A and glycidyl methacrylate
Resin Matrix In Restorative Resin Functions
- Reduces polymerization shrinkage
- Increases strength and rigidity
- Increases viscosity
Composite Restoration Viva Voce
- The color matching for composites when done in a dry state would make the tooth appear lighter than the adjacent teeth
- BIS-GMA and UDMA are extremely viscous
- Conventional composites have a higher amount of ini¬tial wear at occlusal contacts
- Microfill composites are used for restoring class 5 cervical lesions
- Flowable composites should never be placed in areas of occlusal stress
- Higher filler contents exhibit lower water sorption
- Material with higher modulus is more rigid
- Natural light should be used for the selection of shades of composites
- Dentin gingival margin is more prone to marginal microleakage
- Composite should be protected from light to prevent premature polymerization
- Acid-etched enamel surface has a frosted appearance
Minimal Intervention Dentistry Question And Answers
Minimal Intervention Dentistry Short Essays
Question 1. Minimum Intervention dentistry.
Answer:
Minimum Intervention Dentistry:
- Minimum Intervention Dentistry is defined as a philosophy of professional care which deals with the first occurrence, earliest detection, and earliest cure of the disease on micro levels, followed by minimally invasive treatment to repair irreversible dosage caused by that disease
Dental Materials Used:
- GIC
- Resin-based composites
- Dentin bonding agents
- Combination of composites and GIC
Treatment Options:
- ART
- Sandwich technique
- Chemomechanical caries removal
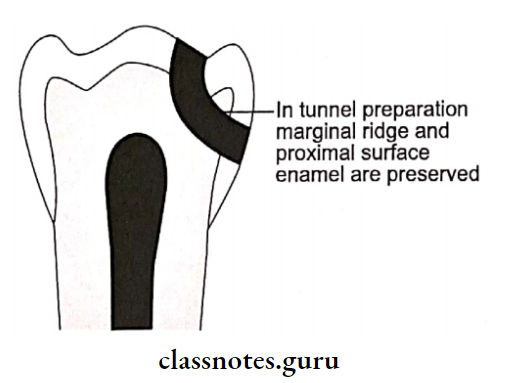
- Tunnel preparation
Read And Learn More: Operative Dentistry Short And Long Essay Question And Answers
- Pit and fissure sealant
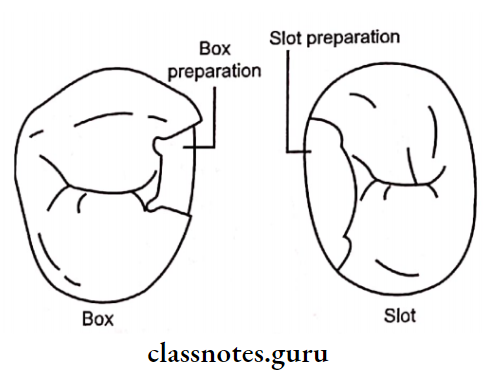
- Box and slot preparation
- Tooth preparation using laser
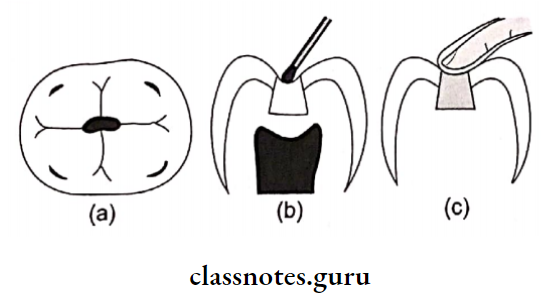
- (A) Carious lesion in posterior tooth
- (B) Excavation of caries using hand instruments
- (C) Restoration of the tooth using glass ionomer cement
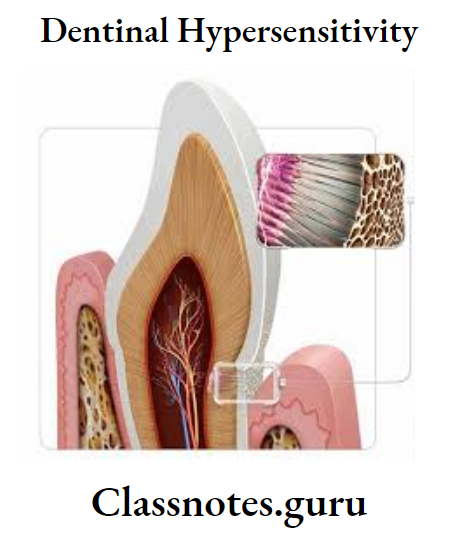
Dentinal Hypersensitivity Question And Answers
Dentinal Hypersensitivity Long Essays
Question 1. Management of dentin hypersensitivity
Answer:
Management Of Dentin Hypersensitivity:
1. Home Care With Gentrifies
- Strontium chloride
- Potassium nitrate
- Fluoride
2. In-Office Treatment
- Varnishes
- Corticosteroids
- Treatment of dentinal tubules
- Burnishing of dentin
- Silver nitrate
- Zinc Chloride
- Iontophoresis
- Fluoride compounds
- Potassium oxalate
- Dentin bonding agents
- Restorative resins
- Laser
3. Patient Education
- Dietary counseling
- Tooth brushing technique
- Plaque control
Dentinal Hypersensitivity Short Essays
Question 1. Theories of Hypersensitivity.
Answer:
Theories Of Hypersensitivity:
1. Neural Theory
- States that hypersensitivity occurs due to the activation of nerve ending lying within the dentinal tubules
- Rejected because
- Dentinal nerves do not extend beyond the inner dentin
- A newly erupted tooth does not poses such nerve endings yet it is sensitive
- Application of local anesthesia to exposed dentin does not eliminate dentin sensitivity
2. Odontoblastic Transduction Theory
- Assume that the odontoblast extend to the periphery
- Stimuli excite the odontoblastic process, this comes into close apposition to nerve endings and transmits excitation to it,
- Rejected because
- Absence of synaptic relationship between odontoblast and pulpal nerves
- There is no neurotransmitter vesicles in the odontoblastic process
- The membrane potential of odontoblast is too low to permit transduction
- The odontoblastic process is restricted to the inner third of dentinal tubules
3. Hydrodynamic Theory
- Proposes that a stimulus causes displacement of the fluid that exists in the dentinal tubules
- This activates the nerve endings present in the dentin or pulp
Read And Learn More: Operative Dentistry Short And Long Essay Question And Answers
- Accepted because
- When dentin is exposed, fluid can be seen
- Profuse branching of tubules at DEJ is present to induce sensitivity
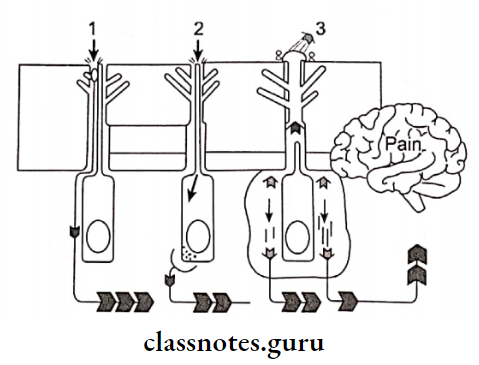
- Neural Theory: Stimulus applied to dentin causes direct excitation of the nerve fibers
- Odontoblastic Transduction Theory: Stimulus is transmitted along the odontoblast and passes to the sensory nerve, endings through synapse
- Hydrodynamic Theory: Stimulus causes displacement of fluid present in dentinal tubules which further excite nerve fibers
Dentinal Hypersensitivity Viva Voce
- The hydrodynamic theory is an accepted theory of dentinal hypersensitivity.
Non Carious Lesions And Management Question And Answers
Non-Carious Lesion Long Essays
Question 1. Define class 5 cavity. Enumerate various materials used for restoring it. Add a note on abstraction.
Answer:
Class 5 Cavity: Caries on the gingival third of facial and lingual or palatal surfaces of all teeth
Class 5 Cavity Materials Used For Its Restoration:
- GIC
- Composite
- Silver Amalgam
Class 5 Cavity Abfraction:
- Wedge-type defects usually occur in cervical areas of the tooth due to excessive occlusal stresses or parafunctional habits
Class 5 Cavity Etiology: Occlusal loading on the tooth
Class 5 Cavity Features:
- Single tooth involvement
- Sharply defined wedge-shaped defect
- Involvement of facial surfaces
- Initially, minor irregular crack on the enamel
- Later, the notch extending into dentin
Read And Learn More: Operative Dentistry Short And Long Essay Question And Answers
Management Of Abrasion, Erosion, And Abfraction:
1. Preventive:
- Correct occlusal disharmony
- Use of appliances to prevent bruxism
- Correct ill-fitting metal clasps/dentures
2. Restorative:
- Materials used
- Composite resins
- Glass Ionomer cement
- Silver amalgam
3. Endodontic Treatment
4. Periodontic Treatment
Non-Carious Lesion Short Essays
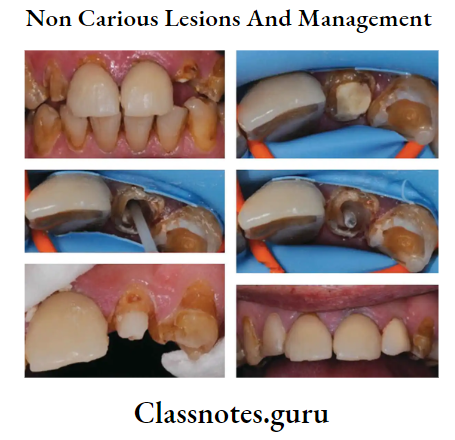
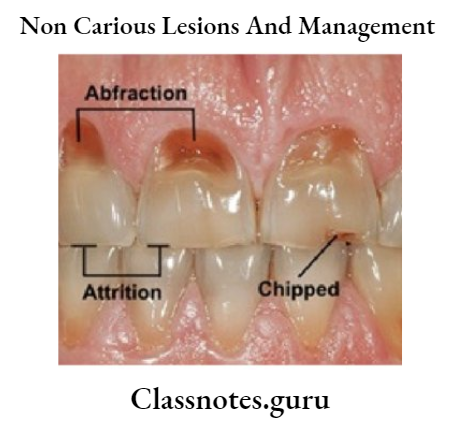
Question 1. Non-carious lesions and their management.
Answer:
Non-Carious Lesions And Their Management:
- Erosion: Erosion is the loss of tooth substance caused by a chemical process that does not involve known bacterial action.
- Abrasion: Abrasion is the loss of tooth substance through some abnormal mechanical process other than tooth contact
- Abfraction: Wedge-type defects usually occur in cervical areas of the tooth due to excessive occlusal stresses or parafunctional habits
Etiology: Occlusal loading on the tooth
Question 2. Erosion.
Answer:
Erosion:
Erosion Definition – Erosion is the loss of tooth substance caused by a chemical process that does not involve known bacterial action.
Erosion Causes:
1. Intrinsic:
- Eating disorder
- Gastrointestinal disorder
- Chronic alcoholism
- Pregnancy morning sickness
2. Extrinsic:
- Dietary origin
- Occupational
- Drug-induced – Aspirin
Erosion Features:
- Broad saucer-shaped depression
- Surface – smooth, hard, and polished
- Sensitive tooth
- Site – Gingival third of the labial surface of anterior
Question 3. Abrasion.
Answer:
Abrasion Definition:
- Abrasion is the loss of tooth substance through some abnormal mechanical process other than tooth contact
Abrasion Causes:
- Faulty oral hygiene practice
- Abnormal oral habits
Abrasion Features:
- Saucer shaped indentation
- Smooth, shiny surface
- Teeth affected – canines and premolars
- Unilateral
- Sharply defined margins and internal angles
Non-Carious Lesion Viva Voce
- Abrasion is seen as a sharp 5-shaped notch in a gingival portion of the facial aspect of the tooth
- Abfraction seen as sharp notch or wedge-shaped lesions
Dental Veneer Question And Answers
Veneers Important Notes
1. Indications
- To mask discoloration due to fluorosis, aging
- To correct enamel hypoplasia and hypo calcification
- To close diastema
- To correct malocclusion
- To improve aesthetics
- To correct progressive wear or fracture of anterior teeth
2. Contraindications
- Presence of inadequate enamel
- Poor quality of enamel
- Presence of habits like bruxism
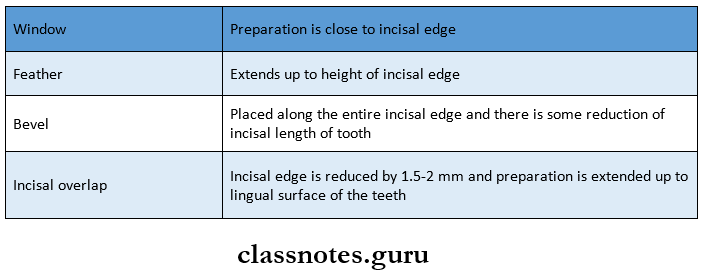
3. Incisal Preparation
- Incisal Preparation Types
Veneers Short Essays
Question 1. Veneers.
Answer:
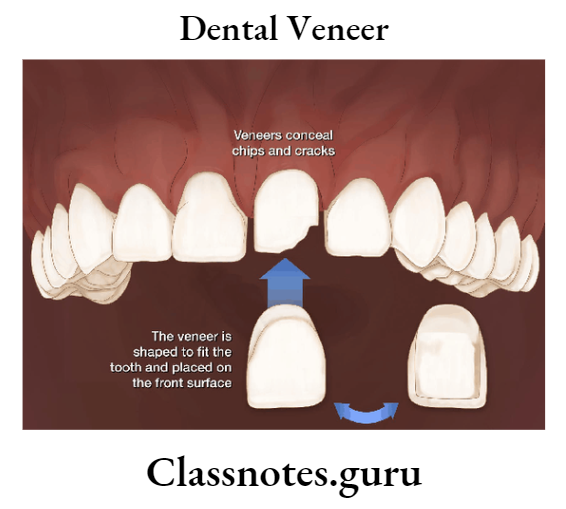
Veneers:
- Described as a layer of tooth-colored material applied on the tooth surface for aesthetic purpose
Veneers Indications:
- Defective surface
- Discolored facial surface
- Discolored restoration
Read And Learn More: Operative Dentistry Short And Long Essay Question And Answers
Veneers Types:
1. Based On The Method Of Fabrication:
- Direct technique
- Indirect technique
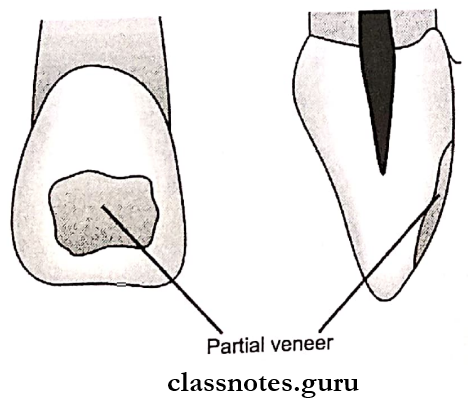
2. Based On The Extent Of Coverage:
- Partial veneer
- Full veneer
Veneers Procedure:
- Cleaning of teeth
- Shade selection
- Isolation
- Tooth preparation
- Acid etching
- Application of bonding agent
- Placement of composite
Veneers Short Answers
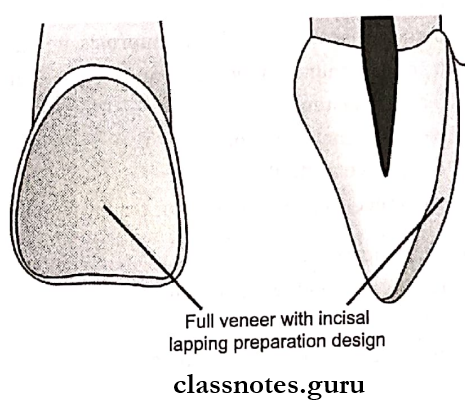
Question 1. Incisal Lapping for Veneers.
Answer:
Incisal Lapping For Veneers:
Incisal Lapping For Veneers Indications:
- Crown lengthening
- Severe incisal defect
Incisal Lapping For Veneers Advantages:
- No need for temporary restoration
- Improved esthetics
Question 2. Direct Veneer.
Answer:
Direct Veneer:
Direct Veneer Indications:
- Localized discoloration
Direct Veneer Advantages:
- Single appointment
- Economical
Direct Veneer Disadvantages:
- More chair time
- More labor
Veneers Viva Voce
- Veneer placement is time-consuming
- Indirect veneers are attached to enamel by acid etching and bonding with resin.
Dental Bonding Question And Answers
Bonding Important Notes
1. Bonding Systems
- Enamel bonding system
- Dentin bonding system
- Amalgam bonding system
2. Enamel Bonding System
- Consist of unfilled liquid acrylic BIS-GMA resin monomer mixture placed onto acid etched enamel
- Steps:
- Acid etching by 37% phosphoric acid
- Results in the formation of resin tags
- A concentration greater than 50% results in the formation of monocalcium phosphate monohydrate that prevents further dissolution
- Below 30% results in the formation of dicalcium phosphate dehydrate that cannot be easily removed
- The length of application of the etchant is 15 seconds
- Increased in fluoride-treated teeth and primary teeth
- Etched enamel is rinsed with water for 20 seconds
- Next enamel bonding agent is applied to the etched surface
- Acid etching by 37% phosphoric acid
3. Dentin Bonding System
- Consist of unfilled liquid acrylic BIS-GMA resin monomer mixture placed onto acid-conditioned dentin surface
- Dentin bonding is difficult because
- Dentin tissue contains plenty of fluids
- Presence of a smear layer
- Chemical effects on the pulp
- Steps:
- Step 1 – Etching/ conditioning
- Conditioners are agents that aid in the removal or modification of the smear layer
- Step 2- Application of primer
- Primers are hydrophilic monomers which are applied over the etched surfaces for easy flow of bonding agents
- Step 3 – Application of bonding agent
- Dentin bonding agents are unfilled resins that help in the formation and stabilization of hybrid layer
- Step 1 – Etching/ conditioning
4. Amalgam Bonding Systems
- Amalgam Bonding Systems is used to bond
- Amalgam to tooth
- Amalgam to amalgam
- Amalgam to other metal substrates
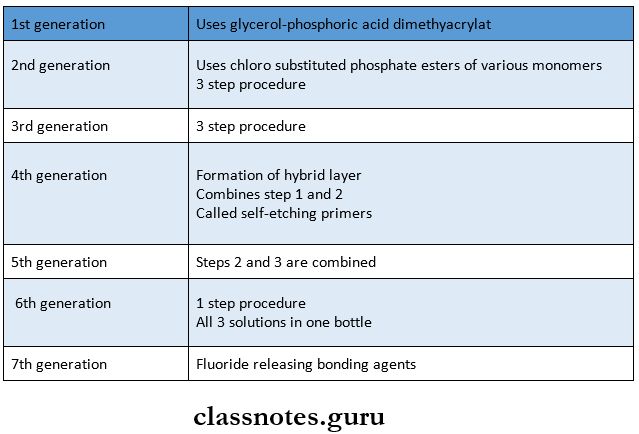
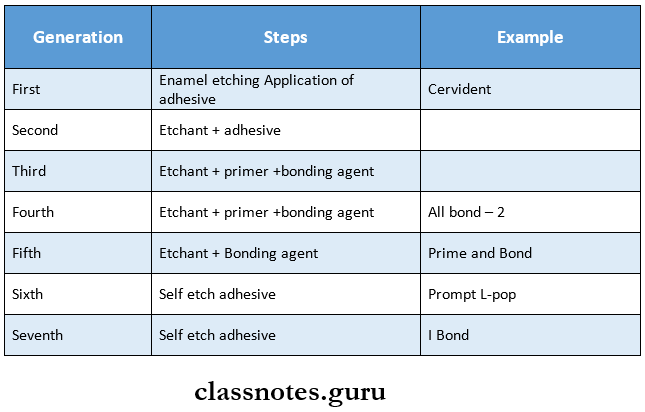
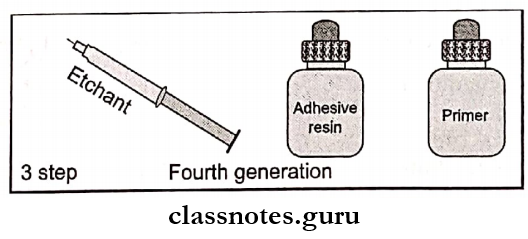
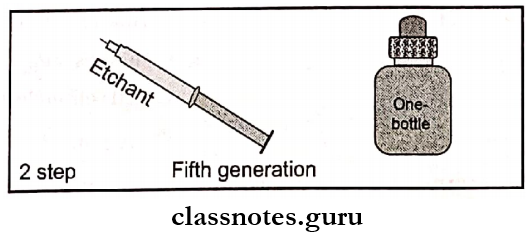
5. Dentin Bonding Agents – Generations
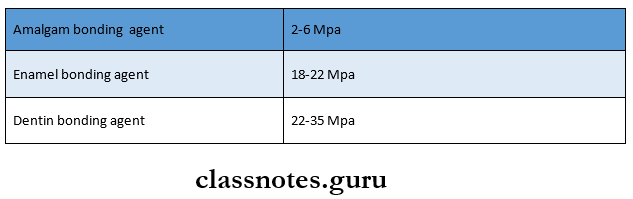
6. Bond Strength Of Various Bonding Systems
Read And Learn More: Operative Dentistry Short And Long Essay Question And Answers
Bonding Short Essays
Question 1. Acid etching.
Answer:
Acid Eetching:
- Acid etching is the process of increasing the surface reactivity by demineralizing the superficial calcium layer and thus creating enamel tags.
- These tags help in micro-mechanical bonding between the tooth and restorative resin.
Acid etching Mechanism:
- Cleanses debris
- Increases enamel surface area
- Produces micropores for mechanical interlocking
- Exposes more reactive surface layer
Factors Affecting It:
- Form of acid-gel
- The concentration of acid – 37% phosphoric acid
- Time – 15-20 sec.
- Chemical nature of enamel
- Type of dentition
Acid etching Technique:
- Oral prophylaxis
- Isolate the tooth
- Application of etchant for 15 seconds
- Rinse thoroughly for 5-10 seconds
- Dry it which results in a frosty, white appearance
- Apply enamel bonding agents
Question 2. Dentin Bonding agents.
Answer:
Bonding Agents:
- Denting bonding agents have both hydrophilic and hydrophobic ends
- The hydrophilic end displaces dentinal fluid while the hydro-phobic end bonds to the composite resin
Bonding Short Answers
Question 1. Hybridization.
Answer:
Hybridization:
- Given by Nakabayachi
- Hybridization is a process of the formation of resin
- Important in micromechanical bonding
- Conditioning the dentinal surface exposes the collagen fibrin network with microporosities
- These spaces are filled with low-viscosity monomers when the primer is applied.
Question 2. Hybrid Layer.
Answer:
Hybrid Layer:
- The layer formed by the demineralization of dentin infiltration of monomer and subsequent polymerization is called a hybrid layer
Zones:
1. Top Layer – Loosely arranged collagen fibrils
- Interfibrillar spaces filled with resin
2. Middle Layer – Replacement of hydroxyapatite crystals by resin monomer
3. Bottom Layer-Unaffected dentin
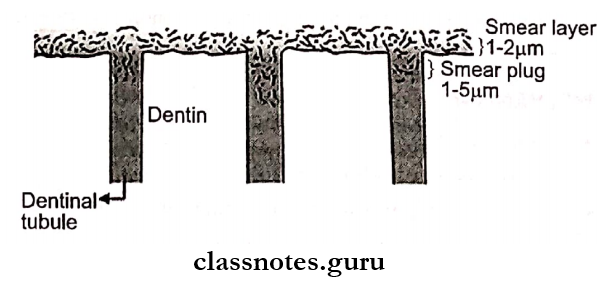
Question 3. Smear Layer.
Answer:
Smear Layer:
Definition:
- Smear Layer is defined as any debris calcific in nature, produced by reduction or instrumentation of enamel, dentin, or cementum.
- Depth – 1-5 pm
Components:
- Inorganic:
- Tooth Structure
- Nonspecific inorganic contaminants
- Organic:
- Coagulated proteins
- Necrotic pulp tissues
- Saliva, blood cells
- Micro-organism
- Role:
- The physical barrier for bacteria
- Diffusion of molecules
- Resistance to fluid movement
Question 4. Types and Definition of Adhesion.
Answer:
Definition Of Adhesion:
- Adhesion refers to the forces between atoms of two unlike substances when placed in intimate contact with each other
Adhesion Types:
- Micromechanical – By formation of resin tags
- Adsorption – Chemical bonding
- Diffusion – Precipitation of substances
- Combinations
Question 5. Objectives of Acid Etching.
(or)
Effects of acid etching on Enamel
Answer:
Objectives Of Acid Etching:
- Creates microporosity in the enamel
- Increases surface area of enamel
- Results in the selective dissolution of enamel
- Formation of resin tag through the penetration of resins
- Forms a mechanical bond to the enamel
- Allows the wetting of tooth surface with resin
Question 6. Self-Etching Primers.
Answer:
Self-Etching Primers:
- These are sixth-generation dentinal adhesives
- Etchant and primes are in the same bottle while the adhesive resin is in other
- Easy to manipulate
- Good bond strength to dentin
- Example. Prompt L-Pop
Bonding Viva Voce
- After etching, the surface area increases up to 2000 times that of the original untreated surface
- Maleic acid, citric acid, and oxalic acid are used to etch enamel and dentin
- The bonding agent enhances the wettability of composites to etched enamel
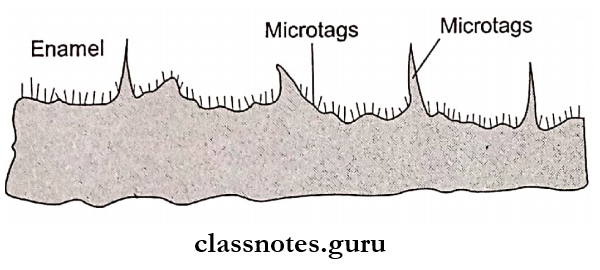
- Resin tags between enamel rod peripheries are called macro tags
- Resin tags across the end of each rod are called micro tags
- Length of micro tags – 2-5 mm
- Most composites are hydrophobic
- 2-HEMA and HEMA dissolved in acetone or alcohol are used as primers
- Cast restorations bonding system uses luting cement
- Buonocore discovered acid etching