
Composite Restoration Important Notes
1. Composite Restoration Disadvantages
- Gap formation due to polymerization shrinkage, microleakage
- Recurrent caries
- Time-consuming
- Technique sensitive
- Exhibit greater occlusal wear
2. Composite Restoration Indications
- Class 1, 2, 3, 4, 5, and 6 restorations
- Sealants and preventive resin restorations
- Foundations or core build-ups
- Luting agent
- Temporary restoration
- Esthetic procedures
- Partial veneers
- Tooth contour modification
- Full veneer
- Diastema closures
- Periodontal splinting
3. Composite Restoration Contraindications
- When isolation is not possible
- If all the occlusal forces will be on restorations
- Restorations that extend on the root surface
- Heavy occlusal stresses
4. Curing Lights Used For Composites
- Halogen bulb combined with filter
- Blue light emitting device
- Laser curing
5. Causes Of failures Of Composites
- Incomplete caries removal
- Incomplete etching
- Defective application of bonding agent
Read And Learn More: Operative Dentistry Short And Long Essay Question And Answers
- Contamination of composite
- Improper polymerization
- Incomplete finishing and polishing
Composite Restoration Long Essays
Question 1. Define composite. Classify and write its com¬position. Describe the management of media angular fracture of upper central right incisor not involving the pulp of a patient aged 14 years.
Or
Mention indications and contraindications of composite resin. Describe the procedure of restoring a fractured incisal angle in the maxillary incisor tooth.
Or
Classify composite resins. Discuss the composi¬tion and methods to reduce the polymerization shrinkage
Answer:
Definition Of Composite:
- Composite is a compound composed of at least two different materials with properties which are superior or intermediate to those of an individual component.
Composite Classification:
1. According To The Particle Size:
- Traditional composite – 8-12 pm
- Small-sized composite – 1-5 pm
- Microfilled composite – 0.4-0.9pm
- Hybrid composite – 0.6-1 pm
2. According To Filler Particles:
- Megafilled
- Macrofilled
- Midfilled
- Minifilled
- Microfilled
- Nanofilled
3. According To The Polymerization Method:
- Self-curing
- Ultraviolet light curing
- Visible light curing
- Dual curing
Composite Composition:
- Organic Resins – BisGMA/UDMA
- Fillers – Zinc, Silicates, Aluminium, Zirconium
- Coupling Agent – Organic silane
- Coloring Agents – Titanium oxide
- Initiator – Camphor quinone
- Inhibitor – Butylated hydroxyl toluene
Composite Indications
- Restoration of Class 1, 2, 3, 4, 5, 6
- Discolored tooth
- Midline diastema cases
- Veneers and laminates
- Bonding of orthodontic appliances
- Restoration of the non-carious lesions
- Core foundation
- As indirect restoration
- For periodontal splinting
Composite Contraindication:
- Difficult to isolate the area
- Patient with high caries index and poor oral hygiene
- Extensive caries, sub-gingivally
- Lesions over the distal surface of the canine

Methods To Reduce Polymerization Shrinkage
1. By The Addition Of Fillers
- Hybrid composites shrink- 0.6-1.4%
- Microfilled composites shrink – 2-3%
2. Incremental Placement Of Composites
- Shrinkage is allowed after the placement of increment before the next increment placement
- This controls polymerization shrinkage
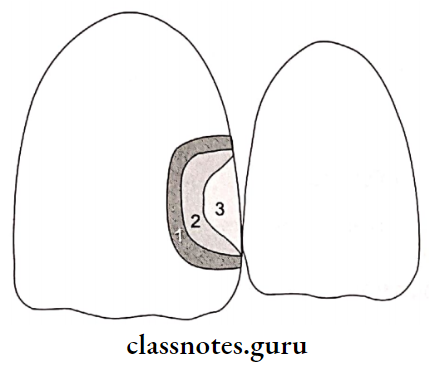
Restoration Of Fractured Central Incisor:
Anesthetized and isolated the tooth
↓
Selection of proper composites
↓
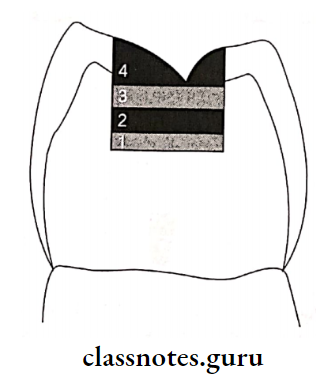
Shade selection – Done in natural daylight Dentin shade selected from
cervical 3rd Enamel shade selected from incisal 3rd
↓
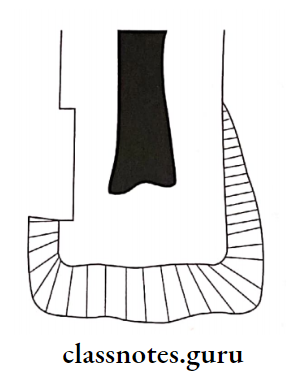
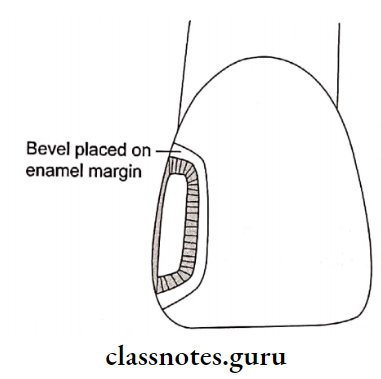
Tooth preparation
1. Enamel margins at 90°
2. Butt joint on root surfaces
3. Enamel bevel
4. Roughening of tooth surfaces
↓
Bonding – Etching, priming and bonding with bonding
agents
↓
Composite placement – In increments along with curing
↓
Carving
1. Attain proximal contour
2. Remove excess material
↓
1. Finishing with diamond points
2. Polishing with rubber points, abrasive discs
Question 2. Enumerate various uses of composite. Describe the restoration of class 2 cavity preparation.
Or
Composite as a posterior restorative material.
Answer:
Various Uses Of Composite:
Composite Indications:
- Small, incipient lesions
- Possible to control moisture
- As core foundation
- Patient with low caries index
Composite Contra-Indications:
- Difficult to control moisture
- Extensive lesion
- High occlusal stresses
- Presence of parafunctional habits
- Patients with high caries index and poor oral hygiene
Composite Disadvantages:
- Polymerization shrinkage
- Technique sensitive
- Time-consuming
- Expensive compared to amalgam
Composite Restoration
1. Tooth Preparation
- Use small round bur, initially
- Extend preparation using fissure bur
- Maintain minimal depth
- Faciolingual dimension l/4th of intercuspal dis¬tance
- No need of retentive features
- Converging occlusal walls
- Rounded line angles
- Bevelling of enamel margin
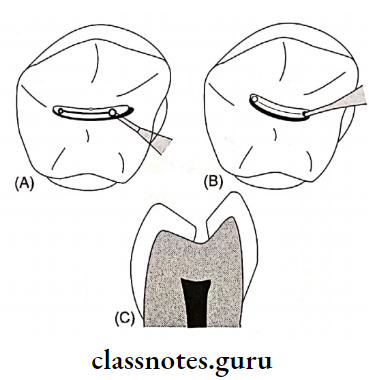
- (A) Preparation of outline usinground bur
- (B) Excavation of caries, keeping the pulpal floor shallow
- (C) Completed class I tooth preparation
2. Matrix placement in Class 2
3. Etching the preparation with 37% phosphoric acid
4. Application of primer and adhesive
5. Pulp Protection
- Use of calcium hydroxide as base
- GIC as liner
6. Composite Placement
- In increments and subsequently curing it
7. Finishing And Polishing
Composite Restoration Short Essays
Question 1. Methods of curing composites.
Answer:
Methods Of Curing Composites:
1. Tungsten Quartz Halogen Curing Unit
- It is conventional
- Uses visible light in the range of 410-500 nm
- Limited lifetime of 100 hours
- Starts curing cycle at a low power density
- Time-consuming
- Plasma arc curing unit
- Use of high-frequency electrical field
- This field ionizes xenon gas into a mixture of ions, electrons, and molecules
- Results in the release of energy in the form of plasma
- Uses 450-500 nm wavelength
- Expensive
2. Light-Emitting Diode Unit
- Have long life i.e. approximately 10,000 hours
- A wavelength of 400-500nm is used
- Suitable for composite with camphor-quinone photoinitiator
3. Argon Laser Curing Unit
- Uses a wavelength of 470 nm
- Monochromatic in nature
- Produces intensity of 200-300 mW
- May cause pulpal damage
- Has a higher degree of polymerization
Question 2. Visible Cured Composite.
Answer:
Visible Cured Composite:
Wavelength – 460-470 nm
Visible Cured Composite Mechanism:
On activation, photoinitiator combines with amine accel-
orator
↓
Release of free radicles
↓
Polymerization
Visible Cured Composite Advantage: Improved color stability
Visible Cured Composite Photoinitiator Used: Camphoroquinone
Composite Restoration Short Answers
Question 1. Packable composite.
Answer:
Packable Composite:
- The basis is Polymer Rigid Inorganic Matrix Material (PRIMM)
- Components – Resin and ceramic inorganic fillers in-corporates in a silanated network of ceramic fibers
- Filler content – 48-65% by volume
- Particle size – 0.7-20 pm
Packable Composite Indications:
- Stress bearing areas
- Class 2 restoration
Packable Composite Advantages:
- Increased wear resistance
- Better reproduction of occlusal anatomy
- The deeper depth of cure
- High flexural modulus
- Decreased polymerization shrinkage
Question 2. Failure in Composite Restoration.
Answer:
Failure In Composite Restoration:
Causes:
- Incomplete caries removal
- Incomplete etching
- Defective application of bonding agent
- Contamination of composite
- Improper polymerization
- Incomplete finishing and polishing
Failures Seen:
- Discoloration
- Marginal fracture
- Secondary caries
- Restoration fracture
- Post-operative sensitivity
- Plaque accumulation
Question 3. Fillers in Composites.
Answer:
Commonly Used Fillers:
- Silica, aluminium, zinc, barium, zirconium
- Boron silicate
Fillers Effects:
- Reduces thermal expansion
- Reduces polymerization shrinkage
- Reduces water sorption
- Increases abrasion resistance
- Increases strength
- Improves handling properties
- Increases translucency
Question 4. Microfilled Composite.
Answer:
Microfilled Composite:
- Particle size – 0.04 – 0.1 micrometer
- Filler content-35-50% by weight
Microfilled Composite Properties:
- Low modulus of elasticity
- Excellent translucency
- Low fracture toughness
- Marginal breakdown
Microfilled Composite Indication:
- Anterior teeth restoration
- Cervical abfraction lesions
Question 5. Hybrid Composite.
Answer:
Hybrid Composite:
- Made up of polymer groups reinforced by an inorganic phase
- Particle size – < 2 nm
- Filler content- 75-80% by volume
Generations Particle size (pm)
Nanofill – 0.04-0.1
Nanohybrid – 1-3
Microhybrid – 0.4-0.8
Hybrid Composite Indications:
- Posterior restoration
- Class 3, 4, and 5 restoration
- Direct veneer
- Discoloration of teeth
Question 6. Light Cured Composite.
Answer:
Light Cured Composite:
- Polymerization is towards the light source
- Material is placed in increments
Light Cured Composite Advantages:
- Adequate working time
- Good color stability
- Aesthetically good
- Less polymerization shrinkage
- More abrasion resistance
Light Cured Composite Activator Used:
- Ultraviolet – 0.1% Benzoin methyl ether
- Visible light-Camphoroquinone
Question 7. Coupling agents.
Answer:
Coupling agents Coupling Agents:
- The coupling agent bonds the filler particles to the resin matrix
- The most commonly used coupling agent are organosilanes
- In the presence of water, the methoxy group of it forms an ionic bond with the filler particle
- On the other end, methacrylate group forms a covalent bond with resin when it is polymerized
Coupling agents Functions:
- Transfers stress to filler particles
- Improves physical and mechanical properties
- Inhibits leaching by preventing water from penetrating along the filler resin interface
Question 8. Nanocomposite restoration.
Answer:
Nanocomposite Restoration:
- Nanocomposites contain filler particles that are extremely small [0.005-0.01 micrometer]
- They may be clustered or aggregated into large units that can be blended with nanoparticles to produce nanohybrids
Nanocomposite Restoration Advantages:
- Good physical properties
- Improved esthetics
- Small particle size
- Highly polishable
Question 9. Resin matrix in restorative resin
Answer:
Resin Matrix In Restorative Resin:
- Matrix of composite resin consists of BisGMA, urethane methacrylate, or TEGDMA
- Bis-GMA is a difunctional monomer produced as the reaction product of bisphenol*A and glycidyl methacrylate
Resin Matrix In Restorative Resin Functions
- Reduces polymerization shrinkage
- Increases strength and rigidity
- Increases viscosity
Composite Restoration Viva Voce
- The color matching for composites when done in a dry state would make the tooth appear lighter than the adjacent teeth
- BIS-GMA and UDMA are extremely viscous
- Conventional composites have a higher amount of ini¬tial wear at occlusal contacts
- Microfill composites are used for restoring class 5 cervical lesions
- Flowable composites should never be placed in areas of occlusal stress
- Higher filler contents exhibit lower water sorption
- Material with higher modulus is more rigid
- Natural light should be used for the selection of shades of composites
- Dentin gingival margin is more prone to marginal microleakage
- Composite should be protected from light to prevent premature polymerization
- Acid-etched enamel surface has a frosted appearance