Fixed Appliances Important Notes
- Components of fixed appliances

Fixed Appliances Long Essay
Question 1. Classify orthodontic appliances and discuss in detail the various components of fixed appliances. Add a note on its advantages and disadvantages.
Answer.
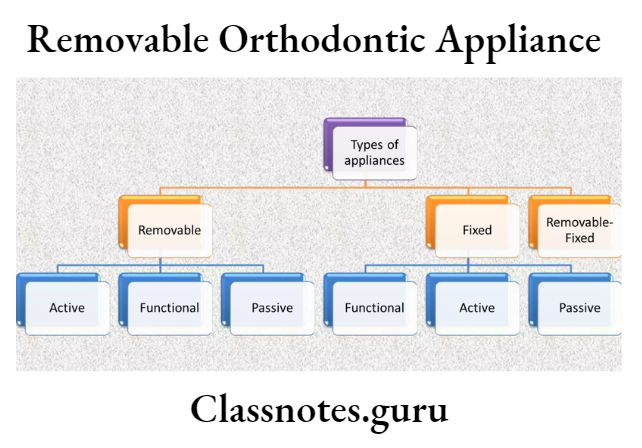
Classification Of Orthodontic Appliances:
- Mechanical appliances
- Removable appliances
- Fixed appliances
- Myofunctional appliances
- Removable appliances
- Fixed appliances
Components Of Fixed Appliances
Active components:
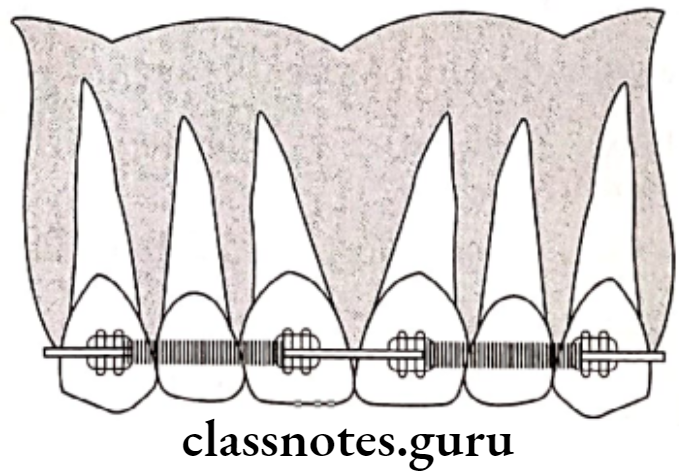
- Archwires
- Bring about tooth movement
Ideal requirement: - High spring back
- Low stiffness
- High formability
- High resilience
- Bio-compatible
- Resist to tarnish and corrosion
- Can be soldered/welded
- Least friction creating
Classification:- Based on material
- Gold and Gold alloys
- Stainless steel
- Nickel titanium
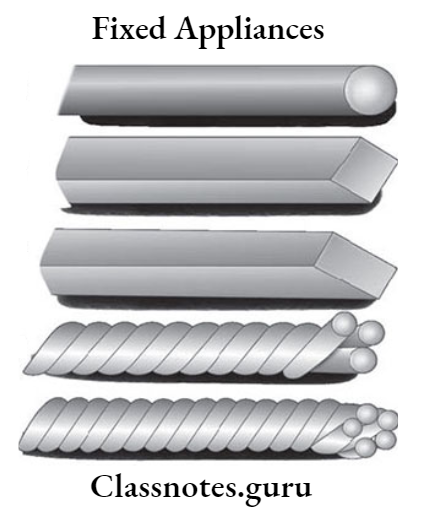
- Based on Cross section
- Round
- Rectangular
- Square
- Multistranded
- Based on material
- Bring about tooth movement
Read And Learn More: Orthodontics Short And Long Essay Question And Answers
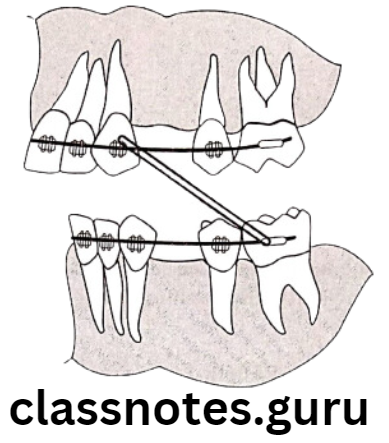
Elastics:
- Simple elactic – Resemble rubber band
- Made of latex rubber
- Available – various diameters and colors
Use:- Closure of space
- Correcting of open bites
- Correction of cross bites
- Correction of inter arch relationship
- Elastic chain
- Material – Polyurethane
- Use – Closure of Space between teeth
- Elastic thread
- Material – Core of latex rubber, surrounded by silk
- Use – Closure of space, Derotation
- Elastic modules – Two rings separated by variable distance
- Use – Closure of space and derotation
- Ligating rings
- Use – To secure arch wires to brackets


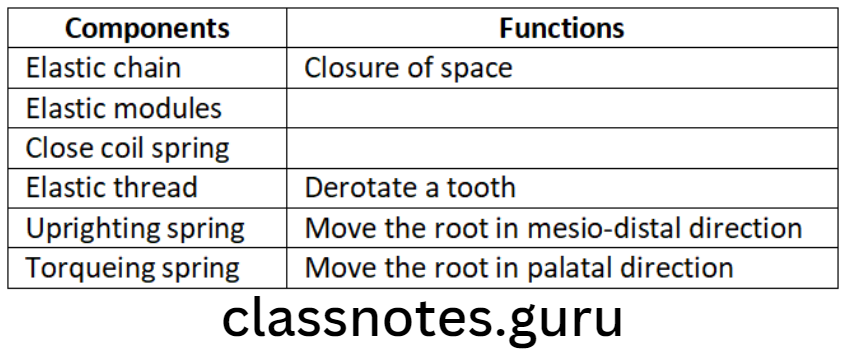
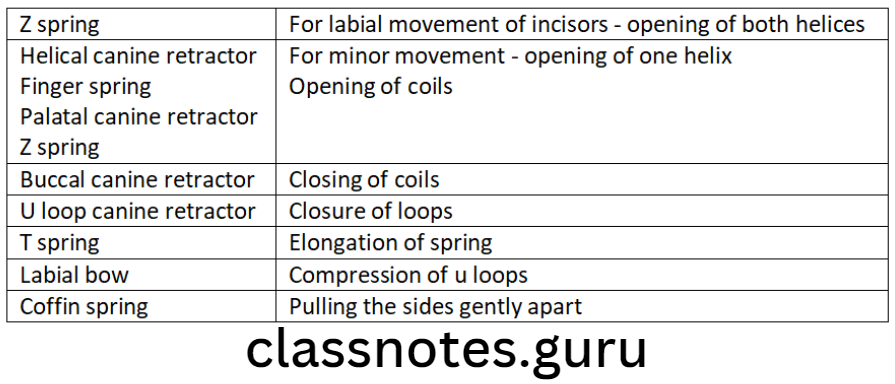
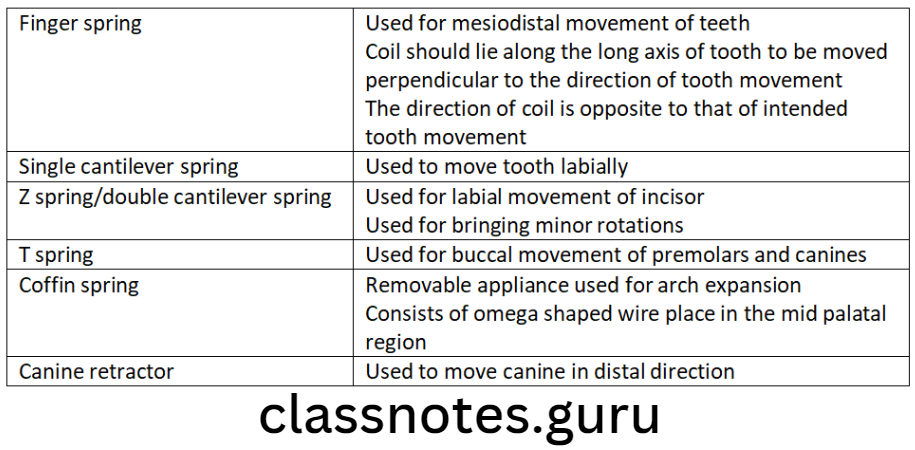
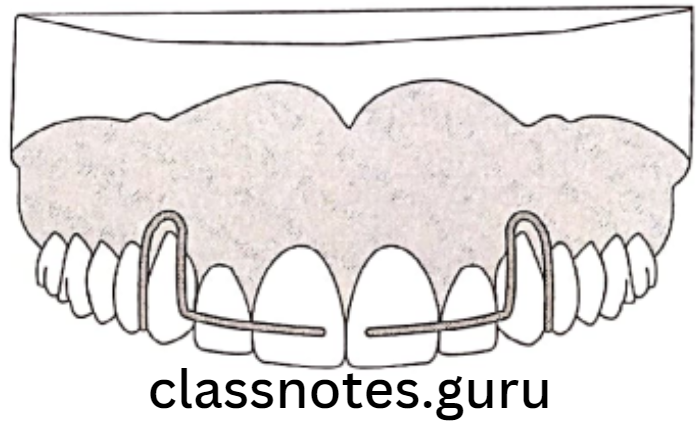
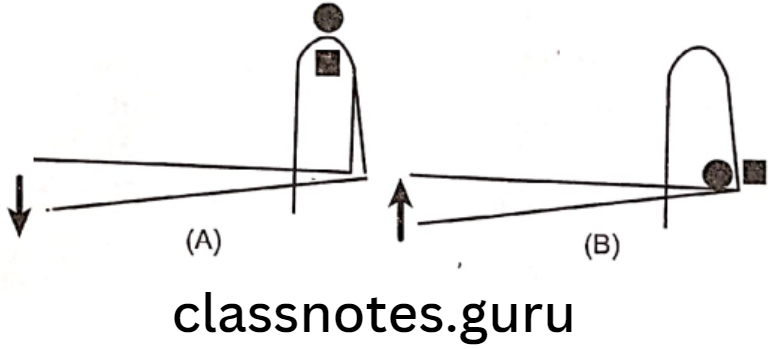
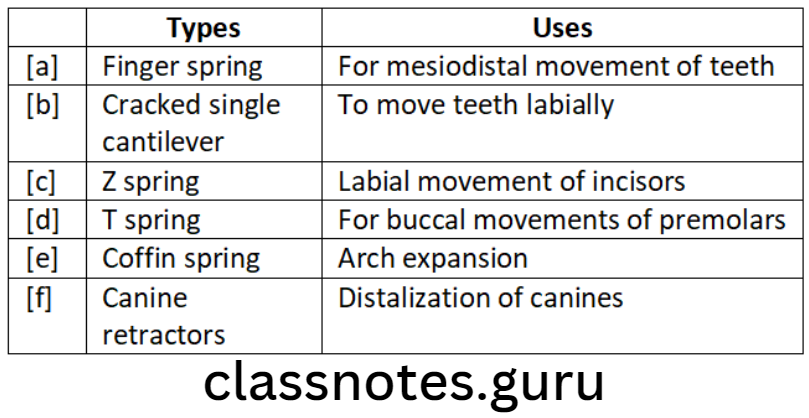
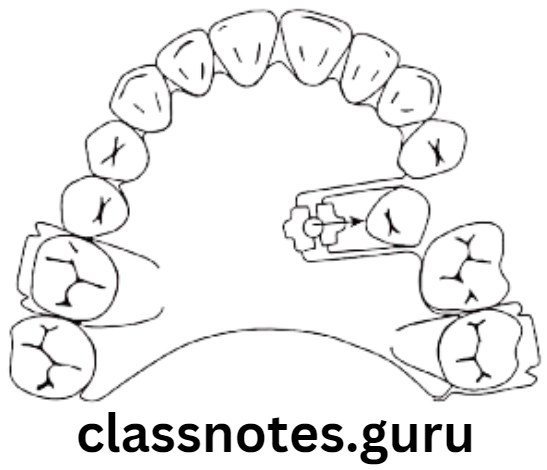
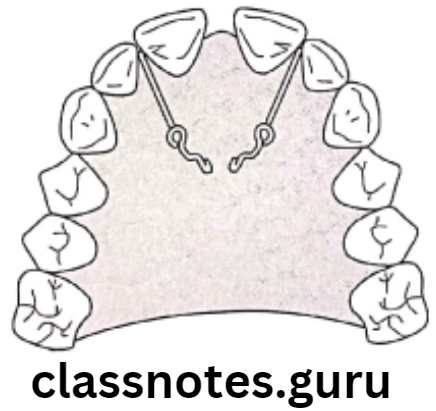
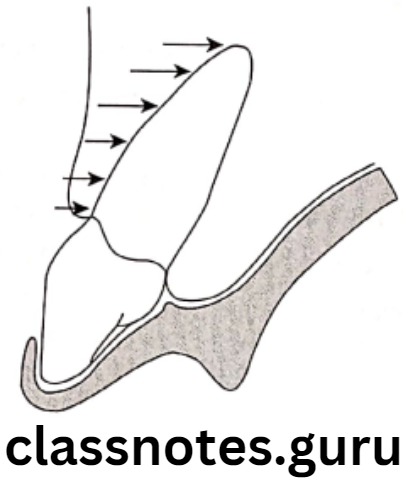
Springs:
Use: To bring about tooth movement
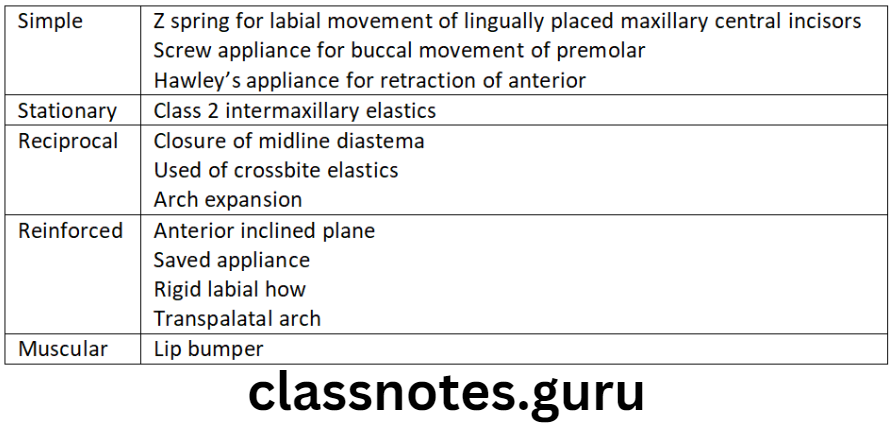
Types Of Orthodontic Appliances:
- Uprighting – to move the root mesially
- Torquing – Move root labially/palatally
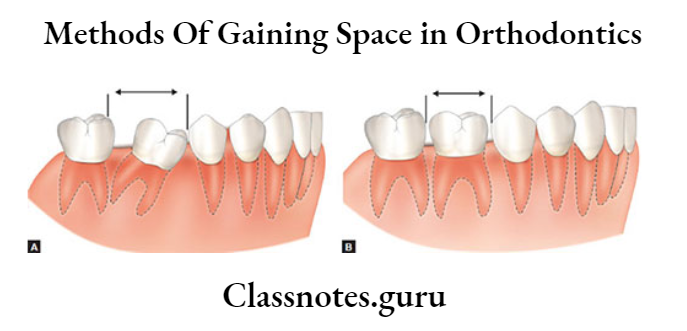
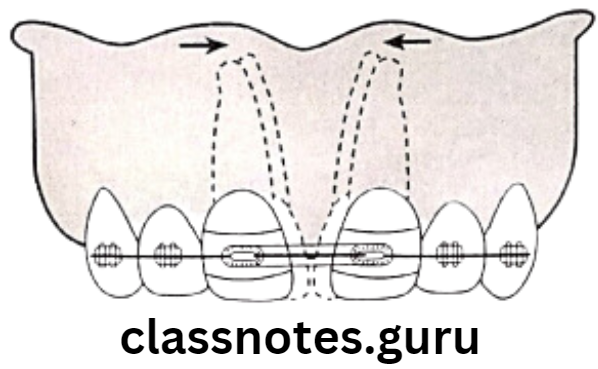
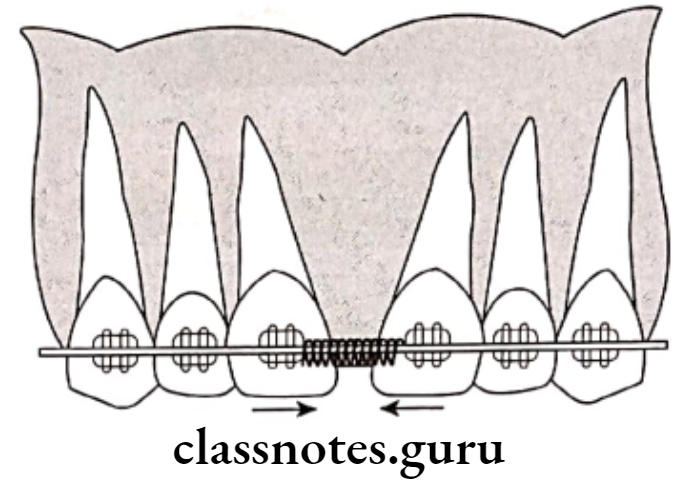
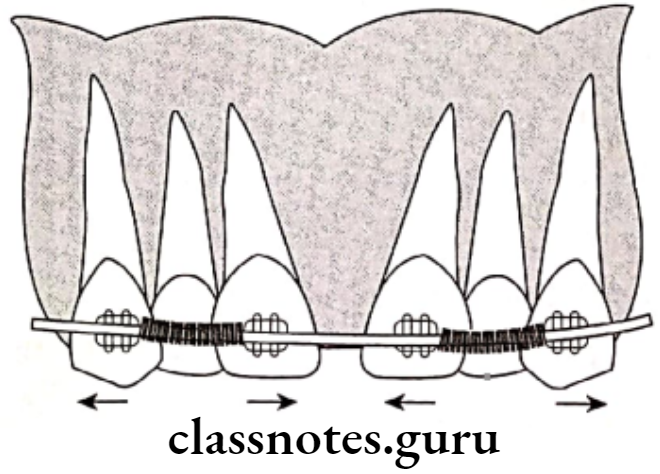
- Open coil springs – To open space between teeth
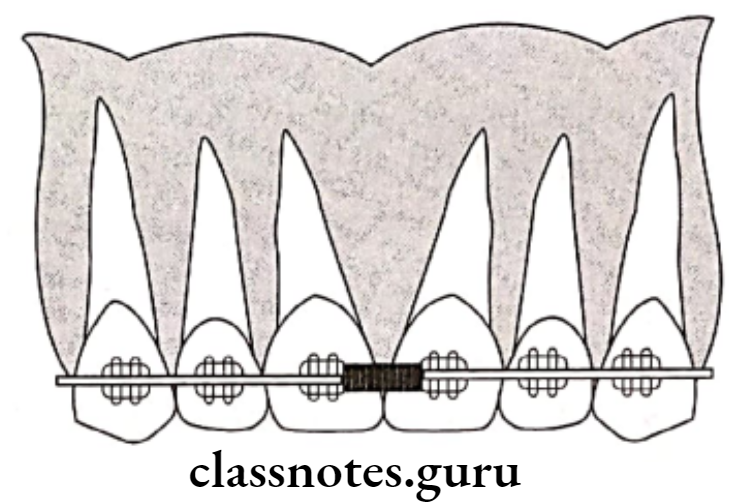
- Closed coil springs – To close space
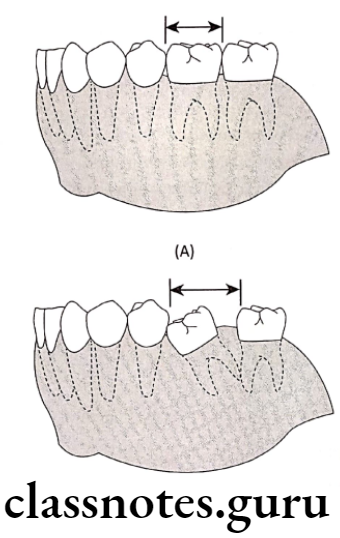
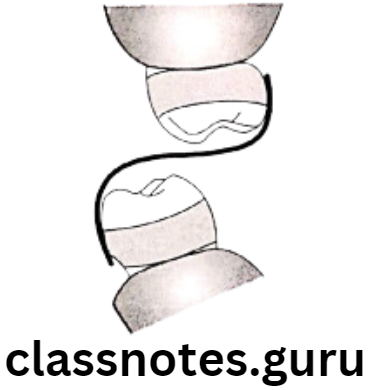
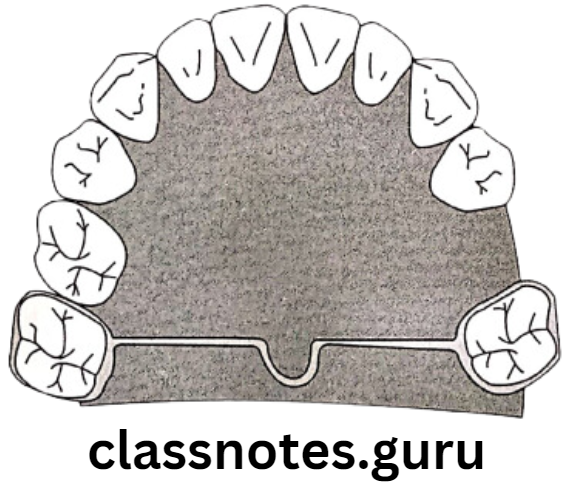
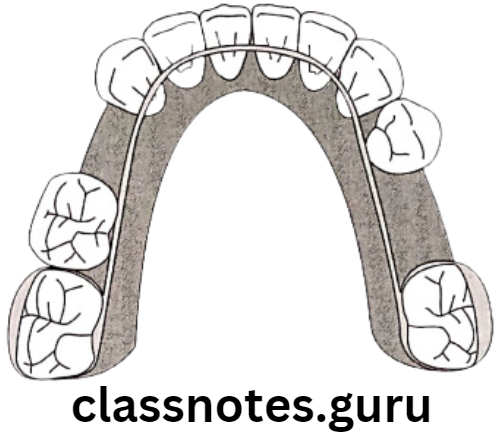
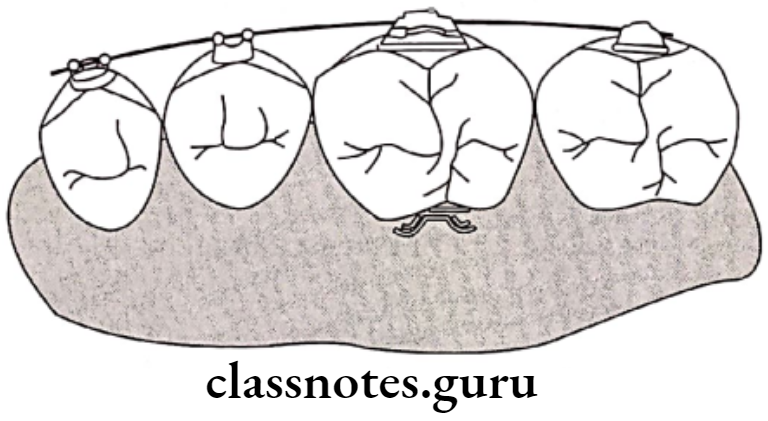
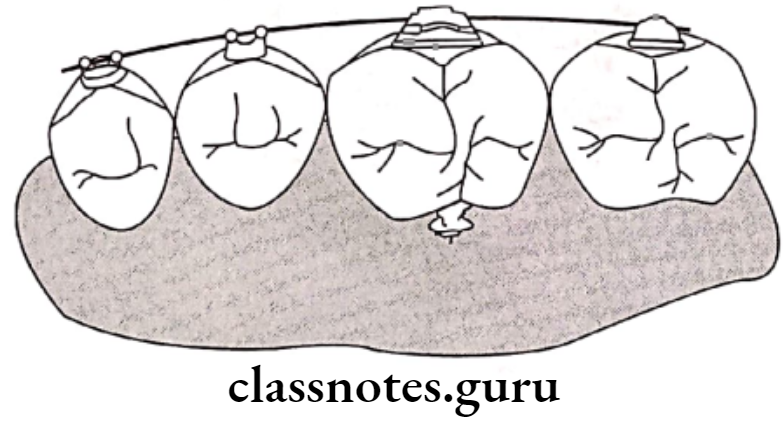
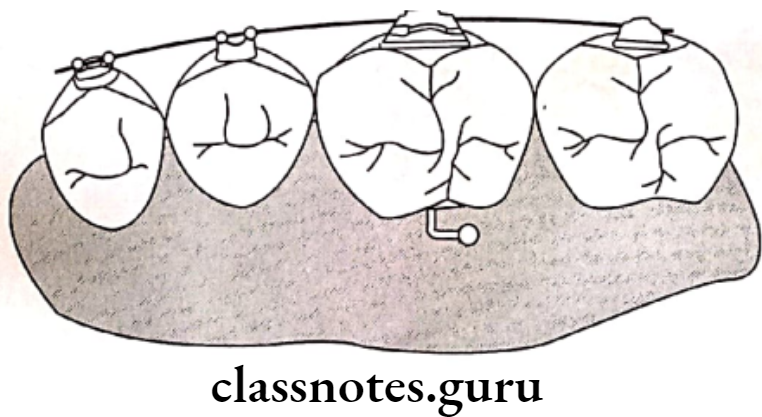
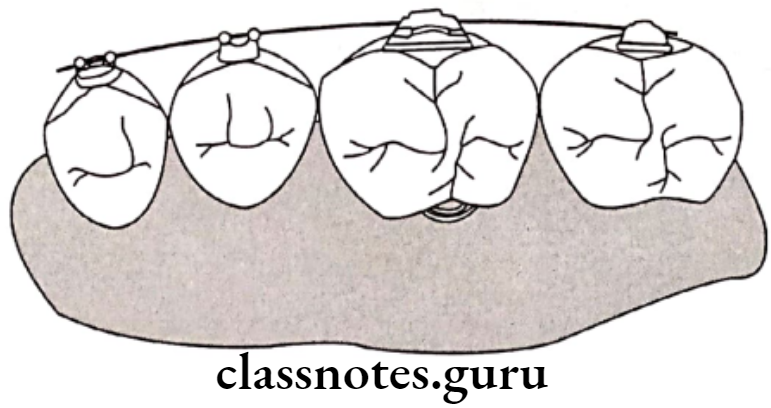
Separators:
Uses Of Separators: To break tight contact
Types Of Separators:
- Brass wire
- Ring
- Dumbbell
- Kesling
Passive Component:
- Bands:
Use – To fix various attachments to tooth
Advantage:- Reduces chair time
- Comfortable for patient
Available:
- In various sizes for different teeth
- Of stainless steel
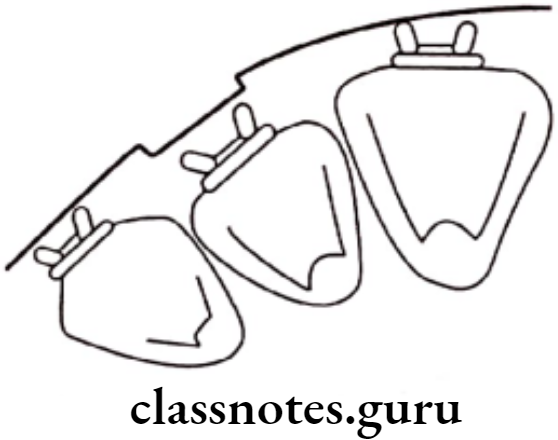
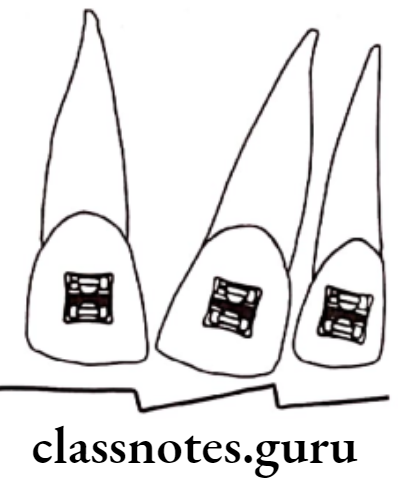
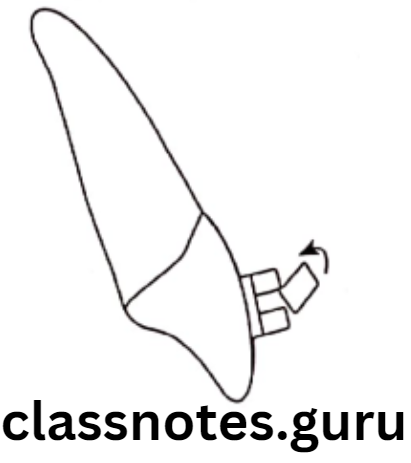
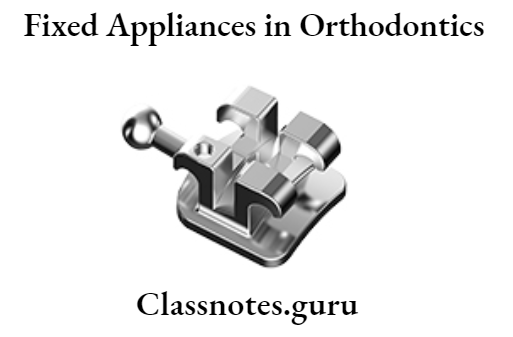
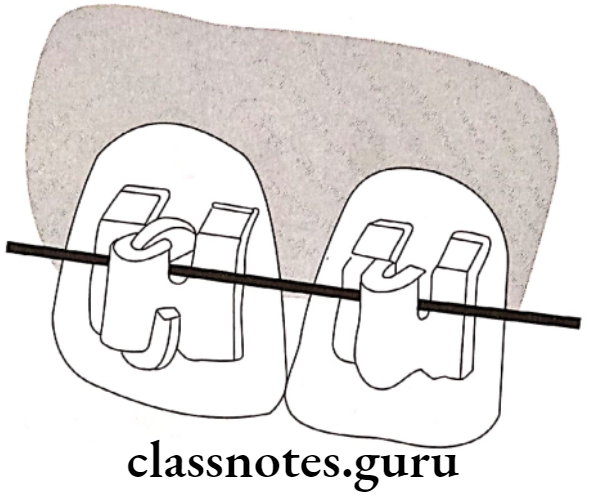
- Brackets:
- Use – To transmit force to teeth
Type:- Edge wise
- Ribbon arch
- Weladable and bondable
- Metallic
- ceramic
- Plastic
- Use – To transmit force to teeth
- Available – In various sizes
- Have one/more slots to accept arch wire
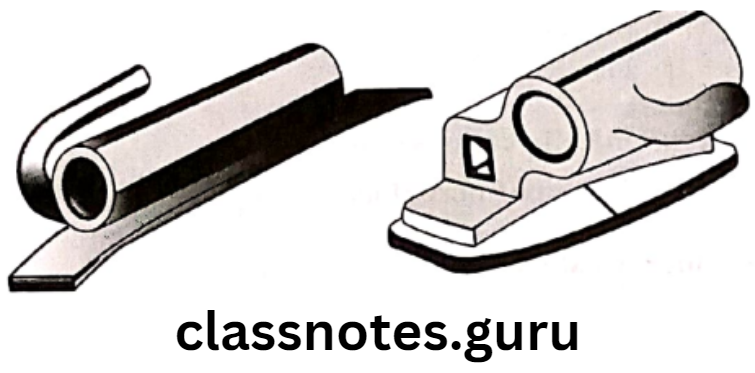
Buccal Tubes:
- Fixed on anteriors/premolar
- On molar called molar tube
- Can be welded/bonded/cemented
- Can be round/rectangular
- Additional tubes for extra-oral anchorage
- Lingual Attachments:
- Attachments fixed on lingual aspect
Example: Lingual buttons, lingual cleats, eye lets and ball end hook
- Attachments fixed on lingual aspect
- Ligature Wires:
- Use – To secure arch wire
- Size – 0.009 – 0.011 inched diameters
- Available in various colors
- Used in edge wise brackets
- Lockpins:
- use – To secure ribbon arch brackets
- Made of brass
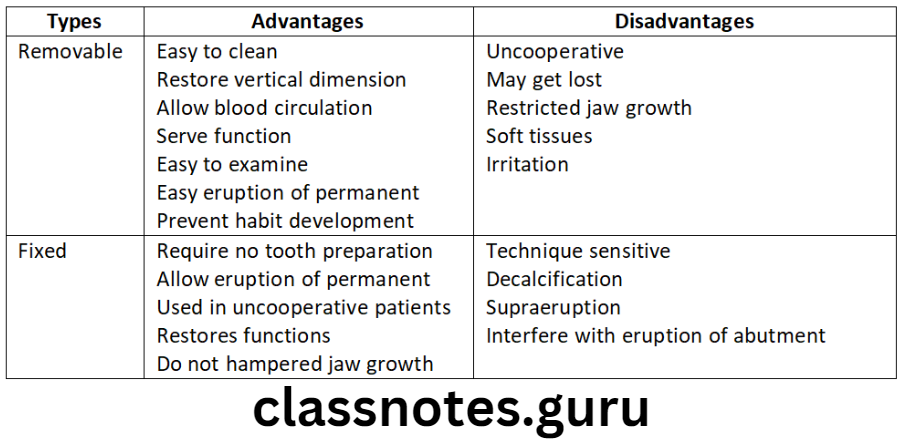
Advantages Of Fixed Appliances.
- Cooperation of patient is achieved
- Various tooth movements are possible
- Tooth movement of multiple teeth is possible simultaneously
- Good occlusion is achieved
- More precise tooth movements possible
- Can be used in complicated malocclusions
- Better anchorage is obtained
- Management of appliance possible
- Convenient for the operator as no need of timely wear of appliance
- Less time of treatment required
Disadvantages Of Fixed Appliances.
- Difficult to maintain oral hygiene
- More time consuming
- More chair time required
- Technique sensitive
- May apply misdirected forces
- Frequent visits required
- Expensive
Fixed Appliances Short Essays
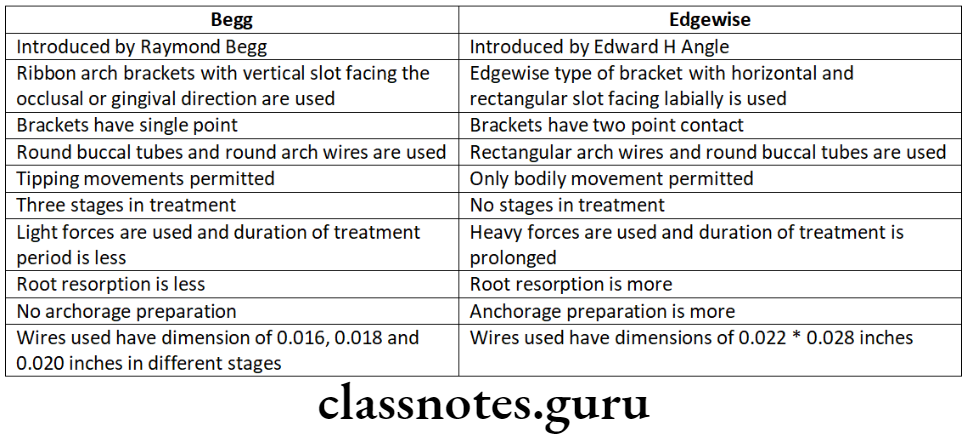
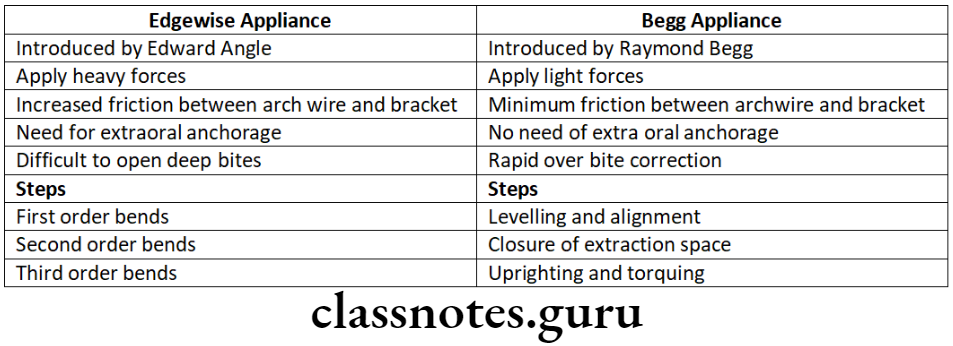
Question 1. Name 3 fixed appliace techniques. Differntiate begg and Edgewise appliances.
Answer.
Fixed Appliance Techniques:
- Edgewise technique
- Begg appliance
- Lingual technique
Question 2. Passive Components of Fixed Appliances.
Answer.
Bands Of Fixed Appliances:
Use – To fix various attachments to tooth
- Advantage:
- Reduces chair time
- Comfortable for patient
- Available:
- In various sizes for different teeth
- Of stainless steel
Brackets Of Fixed Appliances:
Use – To transmit force to teeth
Types Of Brackets:
- Edge wise
- Ribbon arch
- Weladable and bondable
- Metallic
- ceramic
- Plastic
Available – In various sizes
- Have one/more slots to accept arch wire
Buccal Tubes:
- Fixed on anteriors/premolar
- On molar called molar tube
- Can be welded/bonded/cemented
- Can be round/rectangular
- Additional tubes for extra-oral anchorage
Lingual Attachments:
- Attachments fixed on lingual aspect
Example: Lingual buttons, lingual cleats, eye lets and ball end hook
Ligature Wires:
- Use – To secure arch wire
- Size – 0.009 – 0.011 inched diameters
- Available in various colors
- Used in edge wise brackets
Lockpins:
- use – To secure ribbon arch brackets
- Made of brass

Fixed Appliances Short Questions And Answers
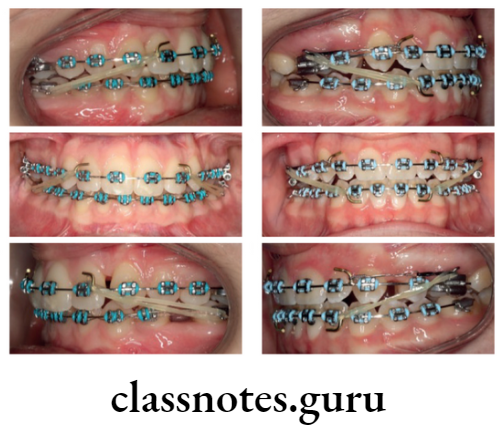
Question 1. Fixed Appliances.
Answer.
Appliances that are fixed/fitted onto the teeth by the operator and cannot be removed by the patient at will are called “Fixed appliances”
Important Advantages Of Fixed Appliances:
- Patient cooperation
- Capable of all tooth movements
- Capable of even root movements
Disadvantages Of Fixed Appliances:
- Poor oral hygiene maintenance
- Time consuming
- Technique sensation
Question 2. Elgiloy Wires.
Answer.
Chemical Name: Cobalt Chromium Nickel
Properties Of Elgiloy Wires:
- Adequate spring back
- Formability
- Biocompatible
- Arch wires – Active component of fixed appliance
Question 3. Molar Tubes.
Answer.
- Fixed on anteriors/premolar
- On molar called molar tube
- Can be welded/bonded/cemented
- Can be round/rectangular
- Additional tubes for extra-oral anchorage
Question 4. Parts of Fixed Appliances.
Answer.
- Active components:
- Archwires
- Elastics
- Springs
- Separators
- Passive components:
- Bands
- Brackets
- Buccal tubes
- Lingual attachments
- Ligature wires
- Lockpins
Question 5. Stainless Steel.
Answer.
- Austenitic stainless steel
- Use – To make orthodontic archwires
Properties Of Stainless Steel:
- Adequate strength
- Adequate spring back
- Resilience
- Formability
- Biocompatible
- Economical
Fixed Appliances Viva Voce
- Brackets are fixed on anterior teeth and premolars
- Buccal tubes are used on molars
- Elastic chains are made of polyurethane
- Zinc phosphate can be used for cementatin of bands onto the teeth
- Oral hygiene maintenance is difficult in case of fixed appliances
- Plastic brackets are made up of poly carbonate
- Titanium arch wires exhibit superior elastic properties
- Lock pins are made of brass
- Buccal tube is passive component of fixed appliance