Anchorage Important Notes
- Advantages of Extraoral anchorage
- Greater forces can be applied
- Permits movement of teeth in one arch without movement of teeth in another arch
- Sites for extra oral anchorage
- Occipital region
- Cervical region
- Parietal region
- Face
- Reinforced anchorage
- More than one type of resistance unit is utilized
- Ex: orthopaedic appliances, anterior inclined plane, transpalatal arch
- Reciprocal anchorage
- Resistance is offered by two units with equal and opposite forced
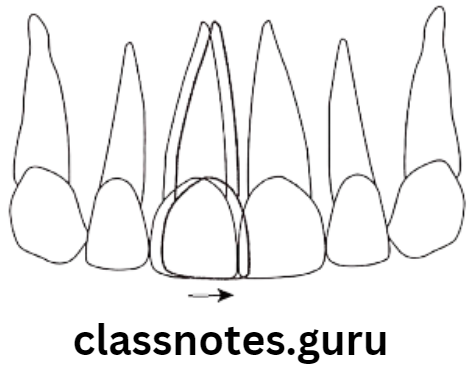
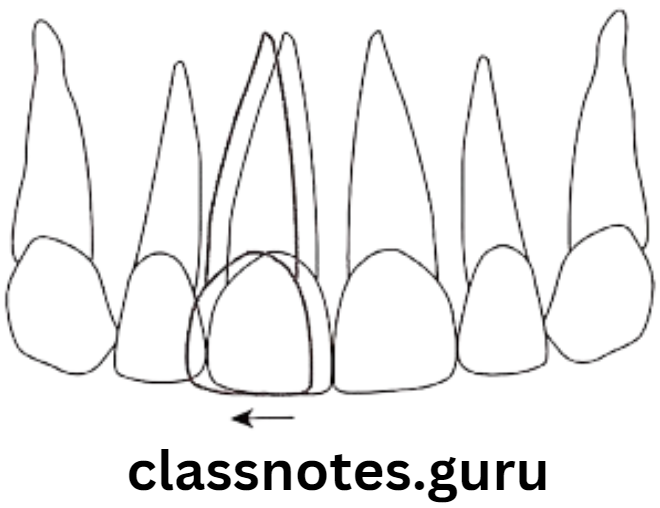
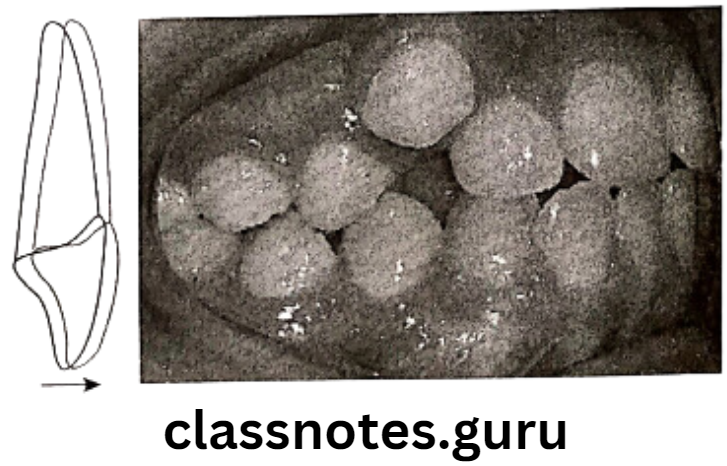
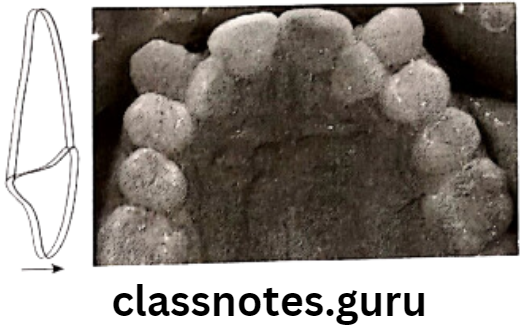
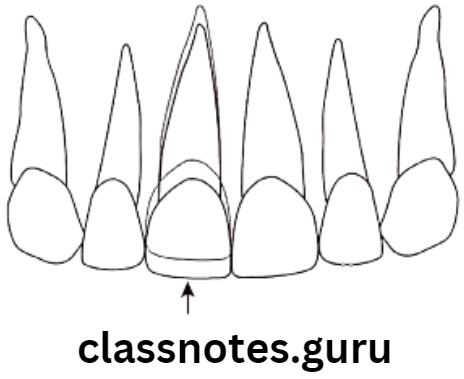
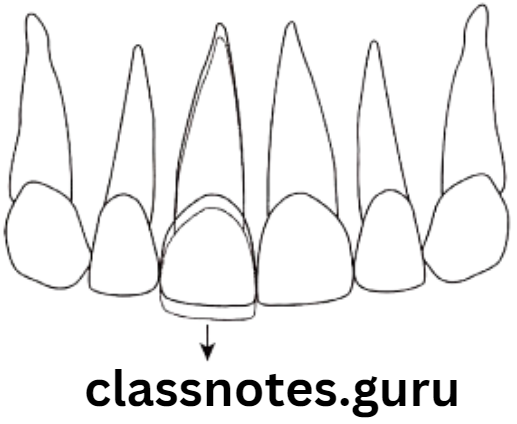
- Example closure of midline diastema, split expansion appliance and correction of crossbite
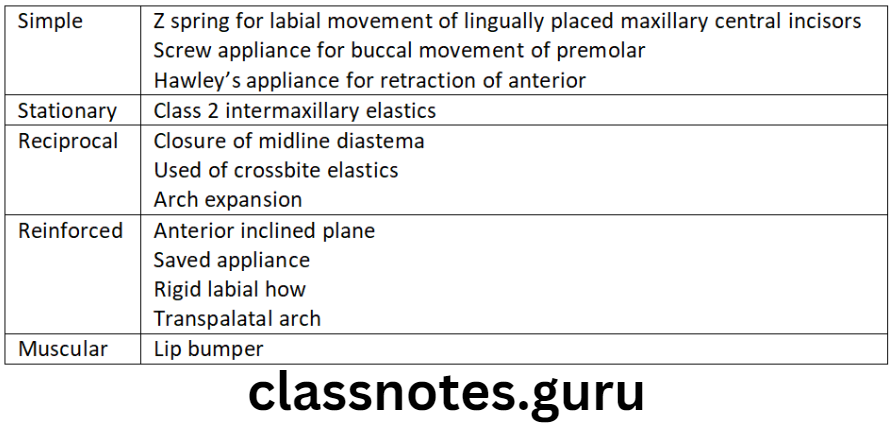
- Types of anchorage with examples
Anchorage Long Essays
Question 1. Define and classify anchorage. Explain in detail about intra-oral anchorage and factors effecting anchorage.
Answer.
Anchorage:
Definition – By Graber:
It is the nature and degree of resistance to displacement offered by an anatomic unit for the purpose of effecting tooth movement
Classification – By Moyer:
According to force application:
- Simple anchorage
- Stationary anchorage
- Reciprocal anchorage
According to jaws involved:
- Intramaxillary
- Intermaxillary
Read And Learn More: Orthodontics Short And Long Essay Question And Answers
According to site of anchorage:
- Intraoral
- Extraoral
- Muscular
According to no.of anchorage units:
- Simple
- Compound
- Multiple
Intraoral Anchorage: Anchorage in which all the resistance units are situated within the oral cavity.
Both teeth to be moved, and the teeth acting as anchorage, are situated in oral cavity
Sources Of Anchorage
- Teeth:
- Remaining teeth, other that the teeth to be moved act as anchorage units
- It depends on its
- Root form
- Root length
- Root no and size
- Ankylosis
- Tooth inclination
- Alveolar bone:
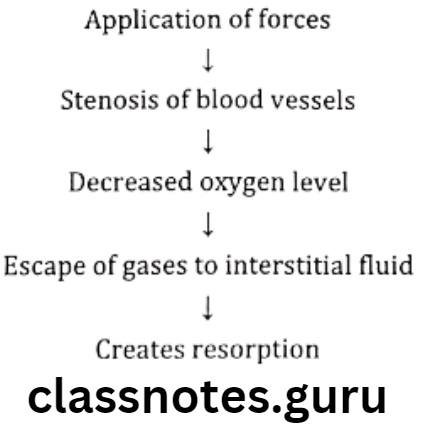
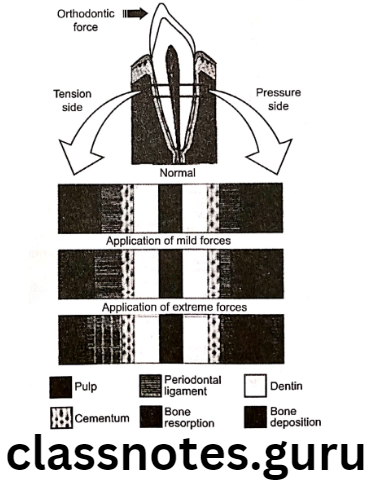
- On application of extreme forces bone permits tooth movement
- Basal bone:
- i.e. hard palate and lingual surface of mandible
- Used to augment intramaxillary or intermaxillary anchorage
- Musculature:
- Use of hypertonic labial musculature through lip bumper
Factors Effecting Anchorage
- No of teeth being moved
- Greater the number
- Greater need of anchorage
- Type of teeth being moved
- Slender anterior teeth – less anchorage
- Multirooted teeth – more anchorage needed
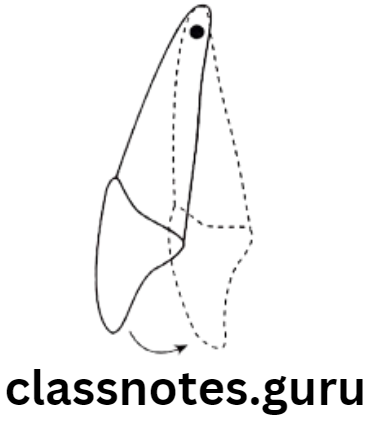
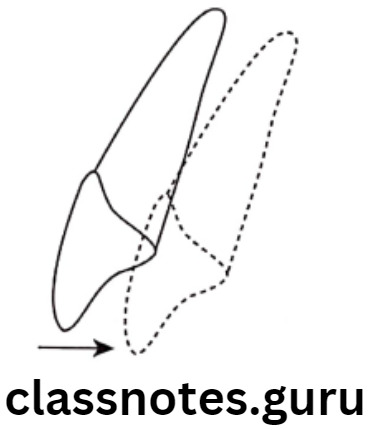
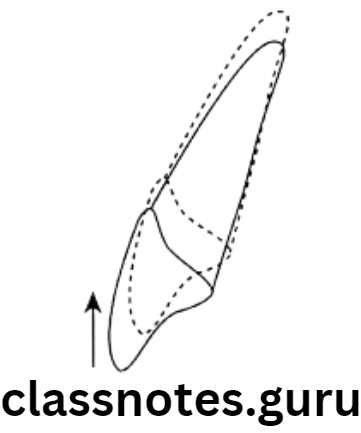
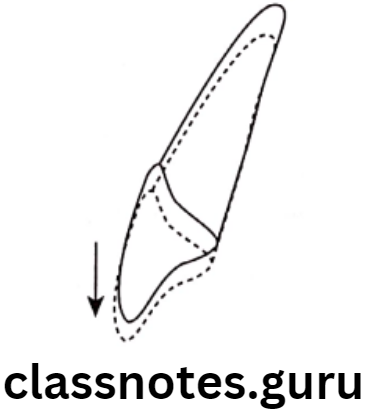
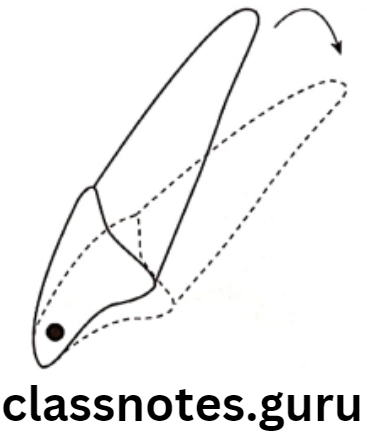
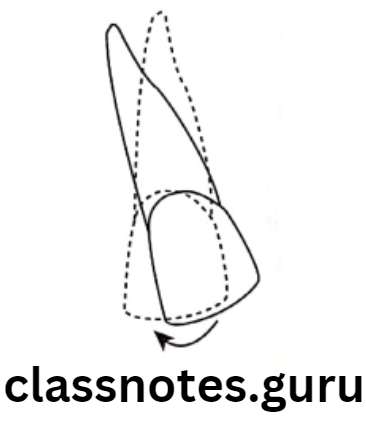
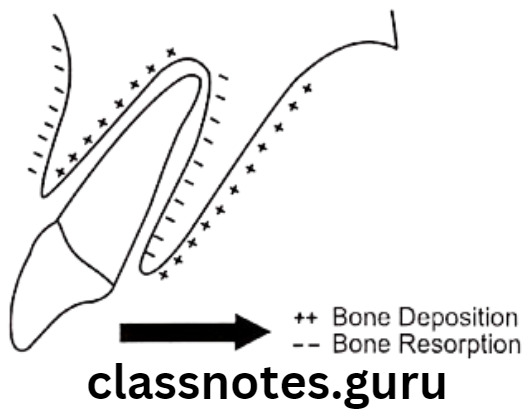
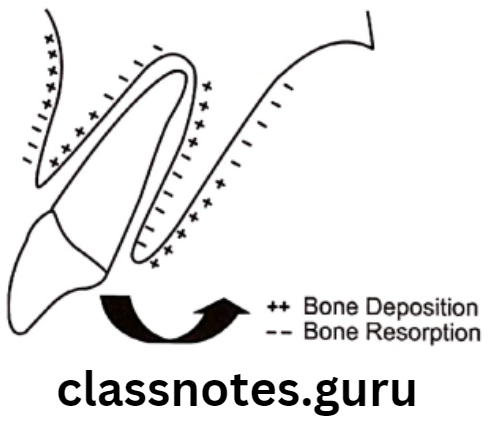
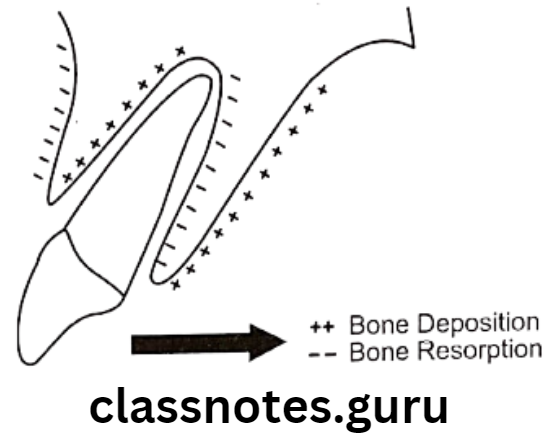
- Type of tooth movement
- Tipping movement – less anchorage
- Bodily movement – more anchorage
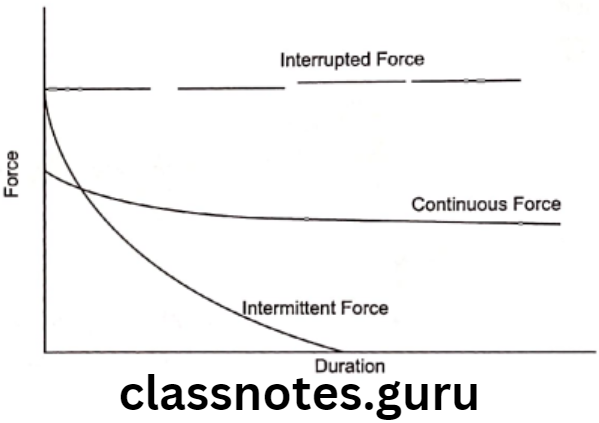
- Duration of tooth movement
- Prolonged duration – undue strain
- Skeletal pattern:
- Vertical grower – More anchorage loss
- Horizontal grower – Less anchorage loss
- Occlusal interlock
- Good buccal occlusion – Resist tooth movement.
Question 2. Define Anchorage. Discuss different types of anchorage with illustrations.
Answer.
Definition – By Moyer:
It is the nature and degree of resistance to displacement offered by anatomic unit to effect tooth movement
Classification – By Moyer:
According to force application:
- Simple anchorage
- Stationary anchorage
- Reciprocal anchorage
According to jaws involved:
- Intramaxillary
- Intermaxillary
According to site of anchorage:
- Intraoral
- Extraoral
- Muscular
According to no.of anchorage units:
- Simple
- Compound
- Multiple
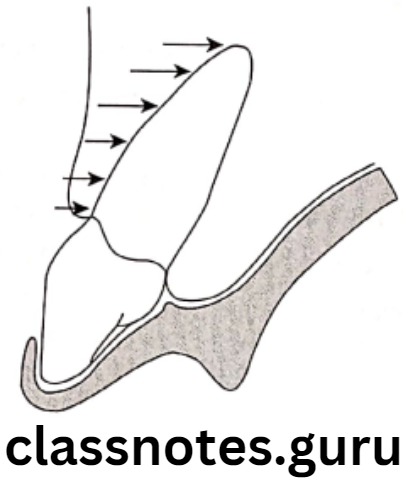
Simple anchorage:
- It is dental anchorage in which manner and application of force is such that it tends to change the axial inclination of tooth/teeth that form the anchorage unit in the plane of space in which the force is being applied.
Manner:
- Removable appliance used to move the teeth
- Here the combined root surface area of anchorage units must be double that of teeth to be moved
Stationary anchorage:
- It is defined as dental anchorage in which the manner and application of force tends to displace the anchorage unit bodily in the plane of space in which the force is being applied.
- Resistance to bodily movement is greater than that of tipping movement
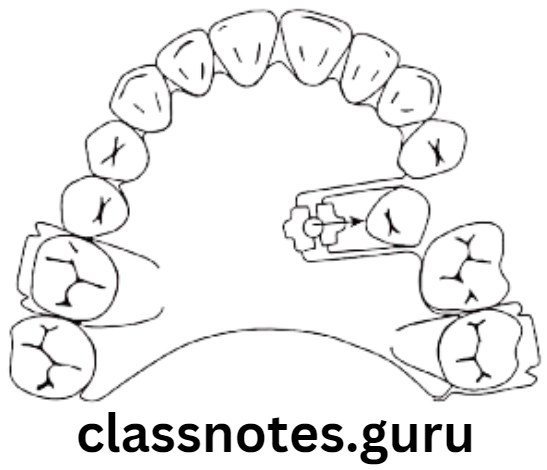
Reciprocal anchorage:
- It is resistance offered by two malposed units when the dissipation of equal and opposite forces tends to move each unit towards more normal occlusion
- Example Closure of mid line diastema, cross bite elastics, arch expansion
Intraoral anchorage:
- Anchorage in which all the resistance units are situated within the oral cavity
- Both teeth to be moved, and the teeth acting as anchorage, are situated in oral cavity
Sources Of Intraoral Anchorage:
Teeth:
- Remaining teeth, other that the teeth to be moved act as anchorage units
Alveolar bone:
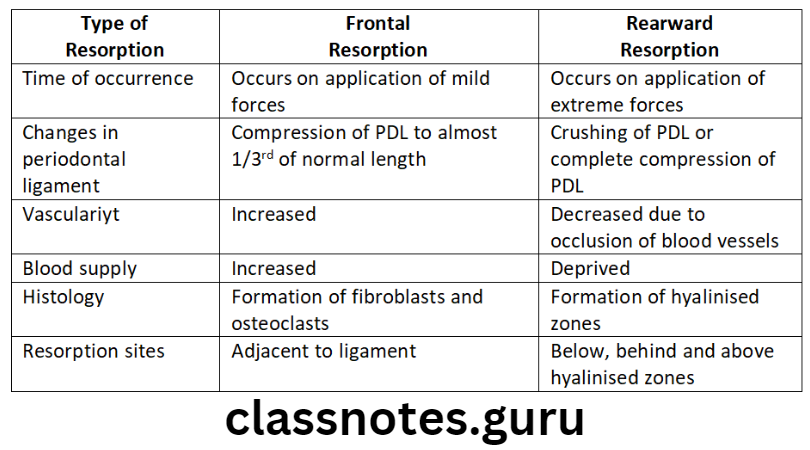
- On application of extreme forces bone permits tooth movement by its resorption
Basal bone:
- i.e. hard palate and lingual surface of mandible
- Used to augment intramaxillary or intermaxillary anchorage
Musculature:
- Use of hypertonic labial musculature through lip bumper
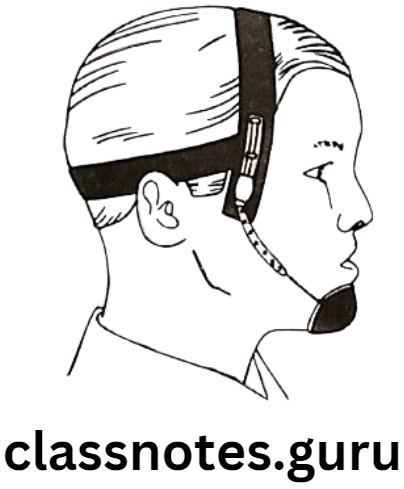
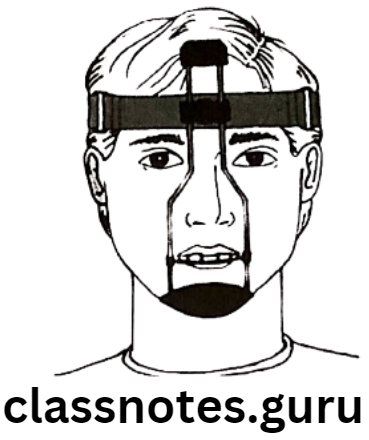
Extraoral anchorage:
- Resistance units are located outside oral cavity
- Example Occiput, back of neck, cranium and face
- Head gear, face mask
Muscular anchorage:
- Perioral musculature acts as resistance units
Example Use of lip bumper
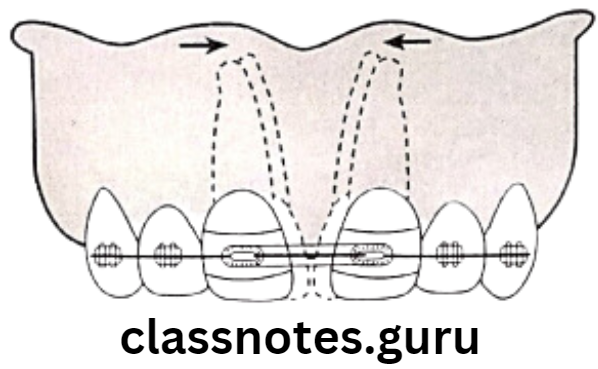
Intramaxillary anchorage: Teeth to be moved and the resistance units, both are situated in same jaw
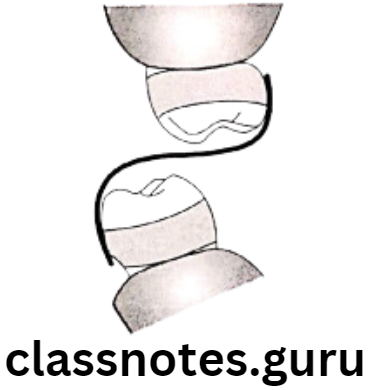
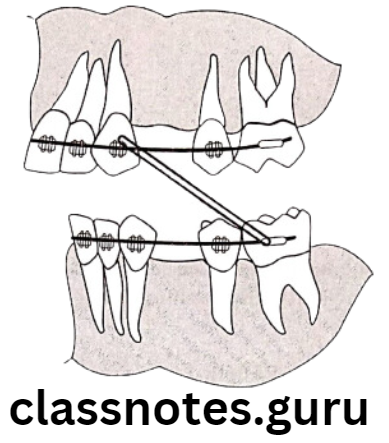
Intermaxillary anchorage [Baker’s anchorage]: Anchorage units are located in one jaw while teeth to be moved are located in other jaw Ex. Class 2 elastic traction between lower molars and upper anteriors
Simple/Primary Anchorage: Single tooth with greater alveolar support it used to move tooth with lesser alveolar support.
Compound Anchorage: More than one teeth with greater alveolar support is used to move tooth with lesser alveolar support.
Reinforced/Multiple Anchorage: Anchorage in which more than one type of resistance unit is termed reinforced anchorage. Ex: Extraoral anchorage, upper anterior inclined plance, transpalatal arch.

Question 3. Define anchorage. Classify it and discuss in detail the methods to reinforce anchorage.
Answer.
Definition – By Graber:
- It is the nature and degree of resistance to displacement offered by an anatomic unit for the purpose of effecting tooth movement
Classification – By Moyer:
According to force application:
- Simple anchorage
- Stationary anchorage
- Reciprocal anchorage
According to jaws involved:
- Intramaxillary
- Intermaxillary
According to site of anchorage:
- Intraoral
- Extraoral
- Muscular
According to no.of anchorage units:
- Simple
- Compound
- Multiple
Methods of Reinforcing Anchorage:
Extraoral forces:
- Forces generated from Cranium, back of neck and face are used
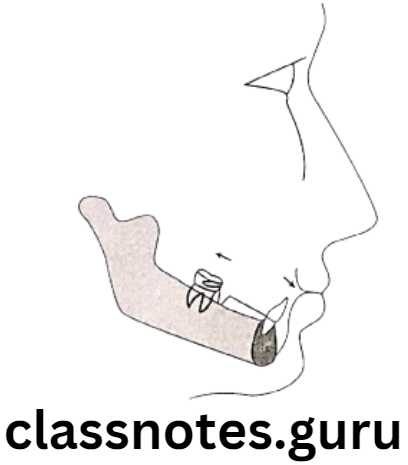
Upper Anterior Inclined Plane:
Effects: Forward gliding of mandible during jaw closure
- Stretching of retractor muscles
- Application of distal force on maxillary teeth
Modification Saved appliances with additional upper incisal capping
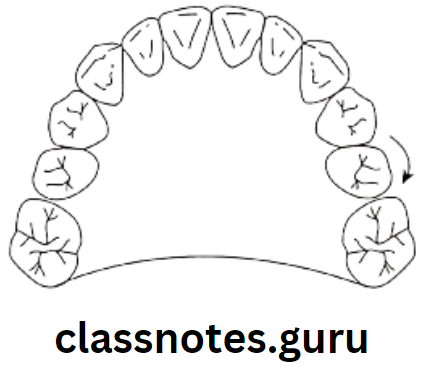
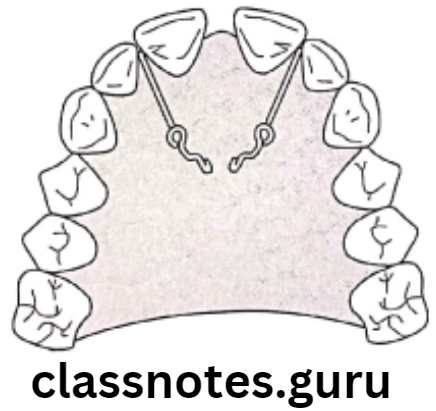
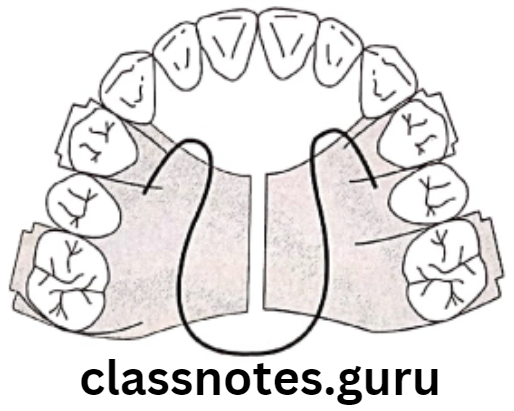
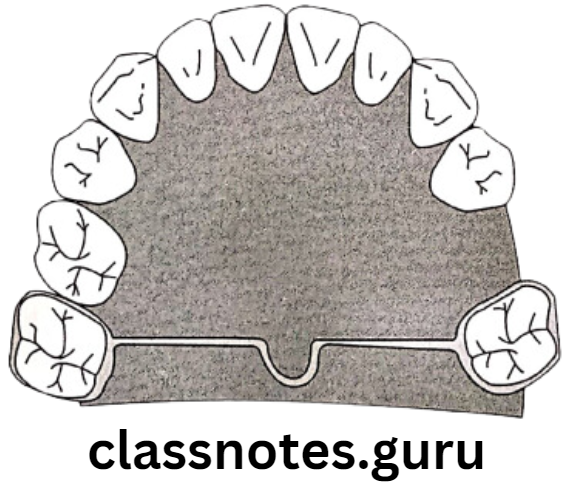
Use of Transpalatal Arch and Lingual Arches:
- Transpalatal Arch: Fixed mechano therapy
- Transverse palate connecting 1st permanent molars of either side
- Lingual Arch:
- Connects contra lateral lower molars through lingual aspects
- Prevents medial movement of lower molar
Anchorage Short Essays
Question 1. Extra Oral Anchorage.
Answer.
Extraoral anchorage:
- Resistance units are located outside oral cavity
- Example Occiput, back of neck, cranium and face
- Head gear, face mask
Question 2. Baker’s Anchorage/Inter-maxillary anchorage.
Answer.
Baker’s Anchorage
Anchorage units are located in one jaw while teeth to be moved are located in other jaw Ex. Class 2 elastic traction between lower molars and upper anteriors
Examples Of Baker’s Anchorage:
- Baker’s anchorage is a form of intermaxillary anchorage used to adjust the jaw relationship and teeth by using elastics from maxilla and mandible
- Class 2 elastics worn from mandibular molars to maxillary anteriors used to retract the maxillary anteriors
- Class 3 elastics worn from maxillary molars to mandibular anteriors used to retract the mandibular anteriors
Question 3. Reinforced Anchorage.
Answer.
Reinforced Anchorage
- Anchorage in which more than one type of resistance unit termed reinforced anchorage.
- Resistance units become more effective when more units are added because the reactionary force is distributed over a larger area
- Distribution of force over large area means keeping force light which minimizes trauma and pain during treatment
Examples:
Extraoral forces:
- Forces generated from Cranium, back of neck and face are used
Upper Anterior Inclined plane:
Effects: Forward gliding of mandible during jaw closure
- Stretching of retractor muscles
- Application of distal force on maxillary teeth
Modification saved appliances with additional upper incisal capping
Use of Transpalatal Arch and Lingual Arches:
- Transpalatal Arch: Fixed mechano therapy:
- Transverse palate connecting 1st permanent molars of either side
- Lingual Arch:
- Connects contra lateral lower molars through lingual aspects
- Prevents medial movement of lower molar
Question 4. Anchorage.
Answer.
Definition – By Graber:
- It is the nature and degree of resistance to displacement offered by an anatomic unit to effect tooth movement
Classification – By Moyer:
According to force application:
- Simple anchorage
- Stationary anchorage
- Reciprocal anchorage
According to jaws involved:
- Intramaxillary
- Intermaxillary
According to the site of anchorage:
- Intraoral
- Extraoral
- Muscular
According to no.of anchorage units:
- Simple
- Compound
- Multiple
Reciprocal Anchorage:
- It is the resistance offered by two malposed units when the dissipation of equal and opposite forces tends to move each unit toward more normal occlusion
- Example Closure of mid-line diastema, crossbite elastics, arch expansion
Question 5. Methods of Reinforcing Anchorage.
Answer.
Extraoral forces:
- Forces generated from the Cranium, back of the neck and face are used
Upper Anterior Inclined Plane:
Effects: Forward gliding of mandible during jaw closure
- Stretching of retractor muscles
- Application of distal force on maxillary teeth
Modification Saved appliances with additional upper incisal capping
Use of Transpalatal Arch and Lingual Arches:
- Transpalatal Arch: Fixed mechanic therapy:
- Transverse palate connecting 1st permanent molars of either side
- Lingual Arch:
- Connects contra lateral lower molars through lingual aspects
- Prevents medial movement of lower molar
Anchorage Short Questions And Answers
Question 1. Reciprocal Anchorage.
Answer.
Reciprocal Anchorage
It is the resistance offered by two malposed units when the dissipation of equal and opposite forces tends to move each unit toward more normal occlusion
Example Closure of mid-line diastema, crossbite elastics, arch expansion
Question 2. Simple Anchorage.
Answer.
Simple Anchorage
It is a dental anchorage in which the manner and application of force is such that it tends to change the axial inclination of tooth/teeth that form the anchorage unit in the plane of space in which the force is being applied.
Manner: Removable appliance used to move the teeth. Here the combined root surface area of anchorage units must be double that of teeth to be moved
Question 3. Factors affecting anchorage.
Answer.
Factors affecting anchorage
- Biological factors:
- Teeth
- Size of anchoring unit
- Axial inclination of teeth
- Use of optimum force
- Differential force system
- Persistent habits
- Mechanical factors:
- Friction
- Type of tooth movement
- Technique employed
Question 4. Anchorage loss.
Answer.
Anchorage loss
- The undersirable movement of the anchor teeth in excess of that planned treatment is known as anchorage loss
- Reasons for anchorage loss
- Excessive force
- Improper treatment planning
- Resistance between arch wires and brackets
- Methods to prevent anchorage loss are
- Use of anchorage savers like transpalatal arches, lingual arches
- Use of optimum and differential force
- Utilizing muscular forces
- Reinforcement of anchorage.
Question 5. Baker’s anchorage
Answer.
Baker’s anchorage
- Anchorage units are located in one jaw while teeth to be moved are located in other jaw Example Class 2 elastic traction between lower molars and upper anteriors
Examples Of Baker’s Anchorage:
- Baker’s anchorage is a form of intermaxillary anchorage used to adjust the jaw relationship and teeth by using elastics from maxilla to mandible
- Class 2 elastics worn from mandibular molars to maxillary anteriors used to retract the maxillary anteriors
- Class 3 elastics worn from maxillary molars to mandibular anteriors used to retract the mandibular anteriors
Anchorage Viva Voce
- Correction of single tooth cross bite is an example of reciprocal anchorage
- Lip bumper is example of muscular anchorage
- Unwanted movement of anchor teeth is called anchor loss
- Anchorage during orthodontic treatment is mainly obtained from intraoral and Extraoral sources
- Ankylosed teeth serve as excellent anchorage
- In maximum anchorage cases 1/4th extraction space can be lost by movement of anchor units