Myofunctional Appliances Important Notes
- Definition of myofunctional applications
- Myofunctional appliances are defined as loose fitting or passive appliances which harness natural forces of the oro-facial musculature that are transmitted to the teeth and alveolar bone through the medium of appliance
- Visual treatment objective [VTO]
- Helps in realizing the therapeutic goals
- Helps to motivate the patient to cooperate by making the patient realize the esthetic improvement
- Types of bionator
- Standard appliance
- Class 3 appliance
- Open bite appliance
- Classification of myofunctional appliances
- According to Tom Graber
- Group A – Teeth supported Ex. Catlan’s appliance
- Group B – Teeth/tissue supported
Example. Activation - Group C – Vestibular positioned Ex. Lip bumper
- Removable – Activator
- Semifixed – Bass appliance
- Fixed – Herbst
- Classical – Activator
- Hybrid – Bass
- Teeth borne passive – Activator
- Tooth borne active – Elastic open activator
- Tissue-borne passive-oral screen
- Tissue borne active – FR
- Functional orthopaedic magnetic appliance
- According to Tom Graber
- Frankel regulator
Myofunctional Appliances Long Essays
Question 1. Classify myofunctional appliances. Name components of FR – 2 and describe its mode of action.
Answer.
Classification Of Myofunctional Appliances:
- According to Tom Graber
- Group A – Teeth supported Ex. Catlan’s appliance
- Group B – Teeth/tissue supported
Example. Activation - Group C – Vestibular positioned Ex. Lip bumper
- Removable – Activator
- Semifixed – Bass appliance
- Fixed – Herbst
- Classical – Activator
- Hybrid – Bass
- Teeth borne passive – Activator
- Tooth borne active – Elastic open activator
- Tissue-borne passive-oral screen
- Tissue borne active – FR
- Functional orthopaedic magnetic appliance
Read And Learn More: Orthodontics Short And Long Essay Question And Answers
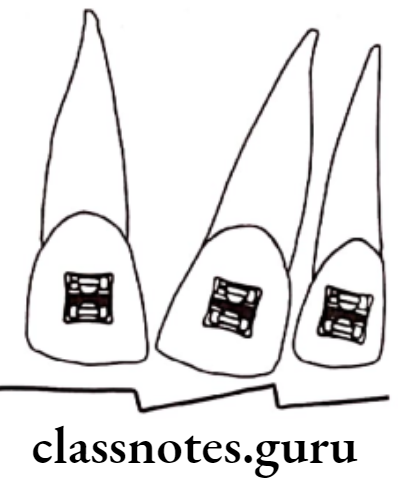
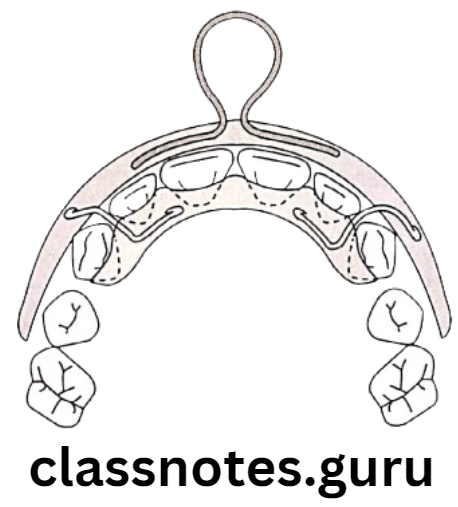
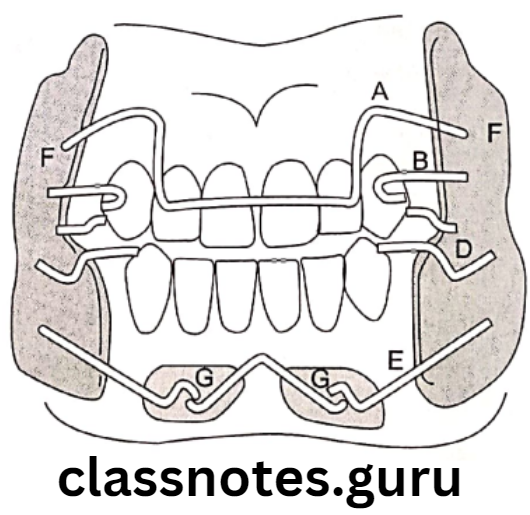
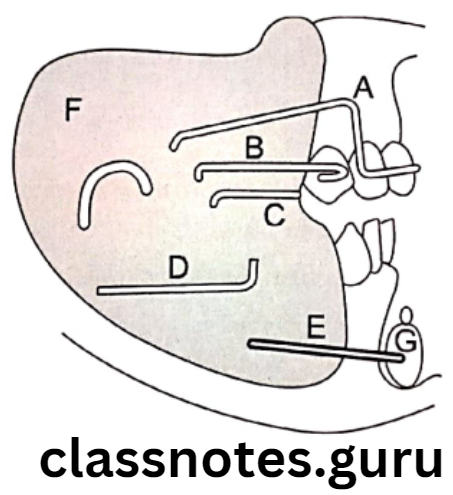
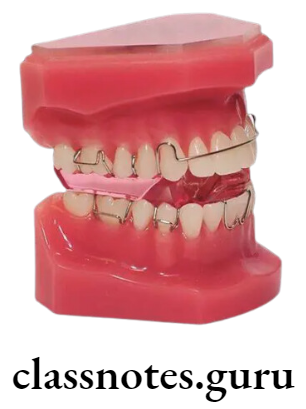
Frankel Appliance
- It is myofunctional appliance developed by Professor Rolf Frankel of Germany
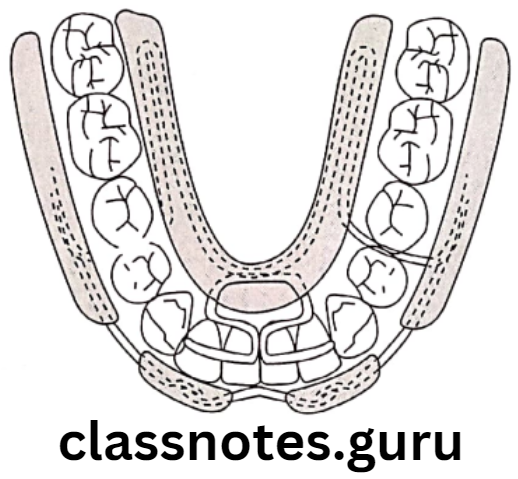
Components Of Myofunctional Appliances:
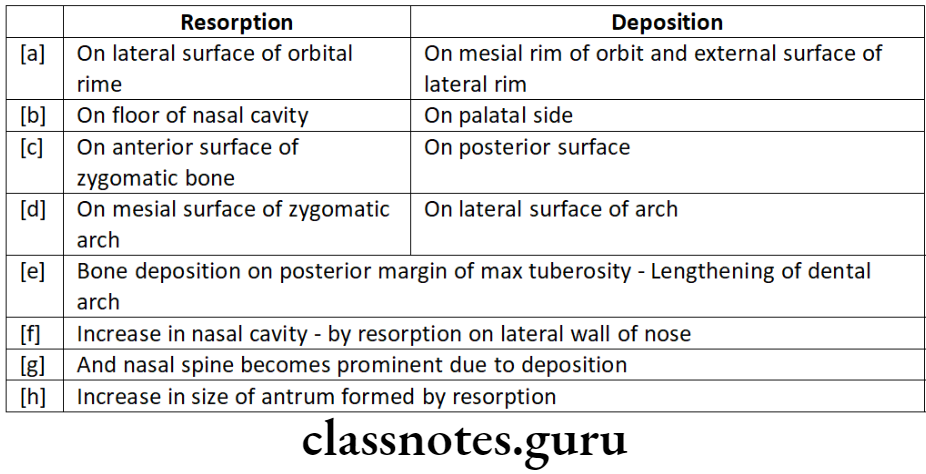
Acrylic component:
- Buccal shields
- Extends deep into the vestibule
- Helps in unrestricted dentoalveolar development
- Also causes periosteal bone deposition
- Lips pads
- Helps in the elimination of abnormal perioral muscle activity
- Eliminates lower lip trap
- Causes periosteal pull resulting in bone growth
- Lower lingual pad
- Stimulates protractor muscles of the mandible by activating proprioceptors
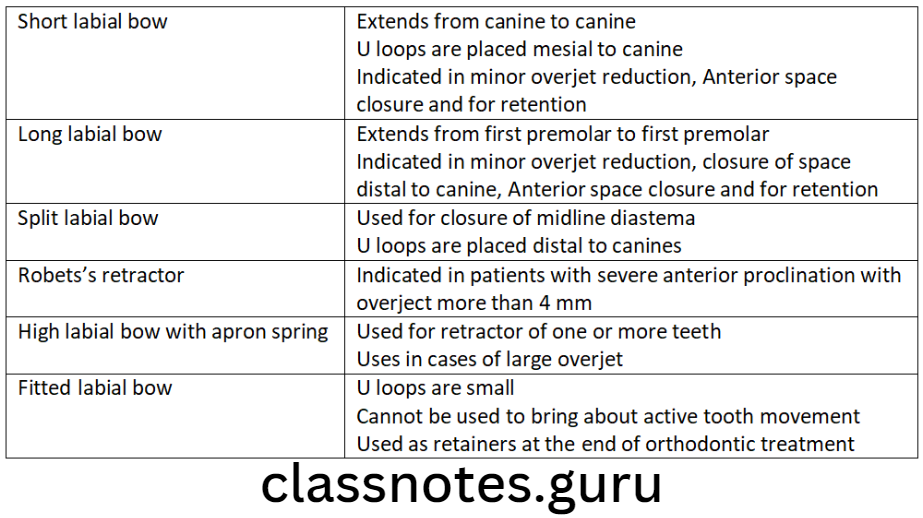
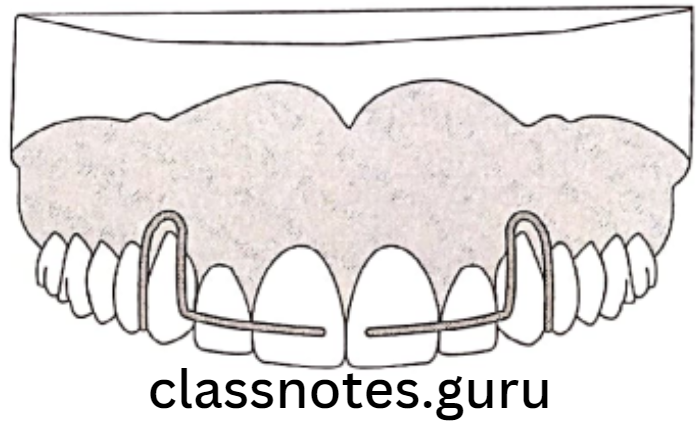
Wire component:
- Labial bow
- Adapted on labial surfaces of the lower anteriors
- Canine extensions
- Eliminates restrictive muscle function
- Helps in transverse development in the canine region
- Palatal bow
- Prevents supra eruption of first permanent molars
- Upper lingual wire
- Runs between the upper canines and first deciduous molars
- Lower lingual springs
- Prevents supra eruption of the lower incisors
- Screens the tongue pressure from lower incisors
- For proclaiming the lower incisors actively
- Causes bite opening by the relative intrusion
Lingual Cross Over Wire:
- Runs between mandibular first and second premolar
Mode Of Action Of Frankel Appliance:
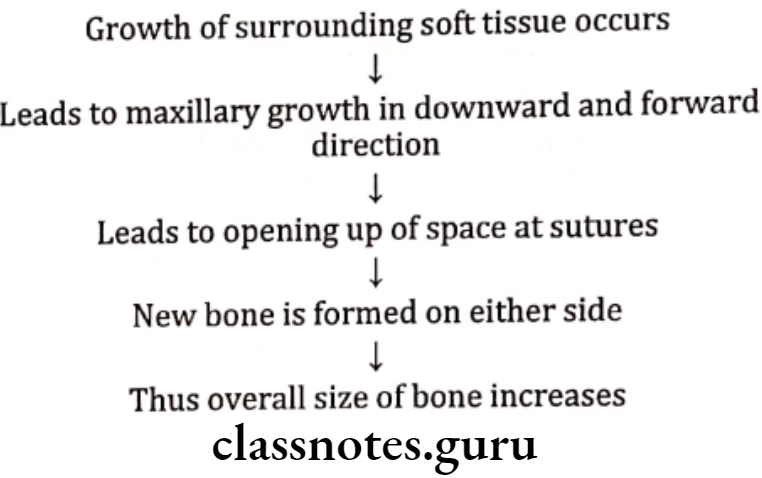
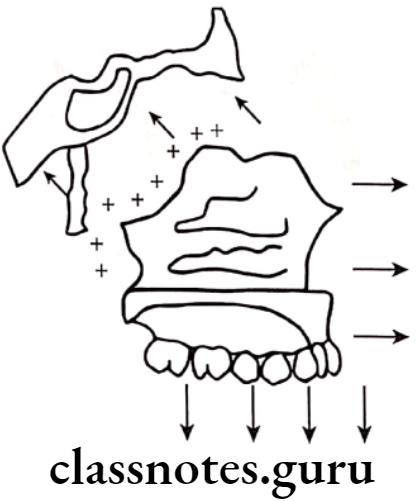
Increase in transverse and Sagittal intra-oral space:
- Buccal shields and lip pads:
- Eliminates abnormal muscular forces
- Favours forces from tongue
- Exerts outward pull on connective tissue and muscles
- This transmits force on the bone
- Results in bone formation
- Leads to lateral movement of dental alveolar region
- Increase in vertical space:
- Frankel appliance does not contact posterior teeth
- Thus, they are free to erupt
- This leads to an increase in vertical intra-oral space
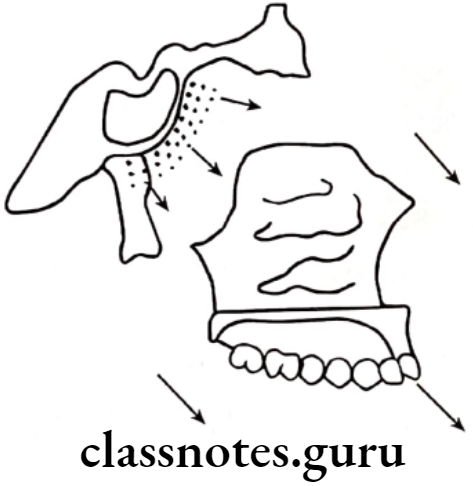
- Mandibular protraction:
- By lingual pads
- These apply pressure on the lingual alveolar process
- Causes activation of protractor muscles
- Position the mandible mesially
- Muscle function adaptation:
- Overcomes abnormal muscular forces
- Rehabilitates muscles
- Causes muscle pull
- This leads to bone formation
- Massages soft tissues
- Improves blood circulation
- Improves muscle tone
- Prevent hyperactivity of mentalis
- Eliminates lip trap
- Establishes lip seal

Question 2. Define and classify myofunctional appliances. Discuss indications and mode of action of the activator.
Answer.
Definition:
- Myofunctional appliances are defined as loose fitting or passive appliances which harness natural forces of the oro-facial musculature that are transmitted to the teeth and alveolar bone through the medium of appliance
Classification Of Myofunctional Appliances:
- According to Tom Graber
- Group A – Teeth supported Ex. Catlan’s appliance
- Group B – Teeth/tissue supported
Example. Activation - Group C – Vestibular positioned Ex. Lip bumper
- Removable – Activator
- Semifixed – Bass appliance
- Fixed – Herbst
- Classical – Activator
- Hybrid – Bass
- Teeth borne passive – Activator
- Tooth borne active – Elastic open activator
- Tissue-borne passive-oral screen
- Tissue borne active – FR
- Functional orthopaedic magnetic appliance
Activator Of Myofunctional Appliances:
- Activator is myofunctional appliance described by Andresen and Haupl
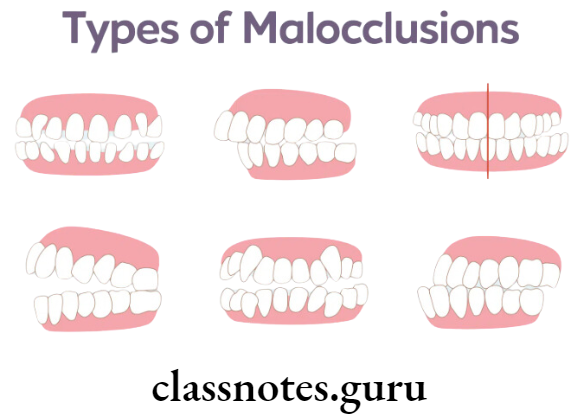
Indications Of Myofunctional Appliances:
- Class 1 open bite
- Class 1 deep bite
- Class 2 div. 1
- Class 2 DDiv 2
- Class 3
- Preliminary treatment
- Post-treatment retention
- Decreased facial height
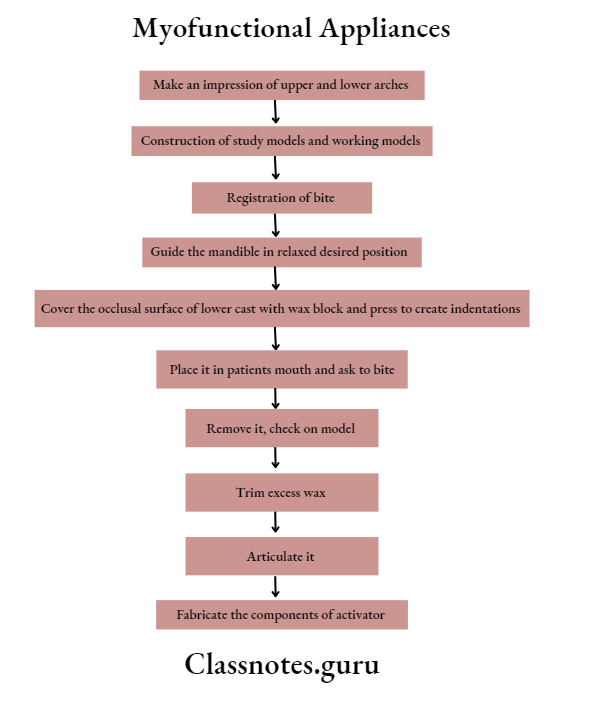
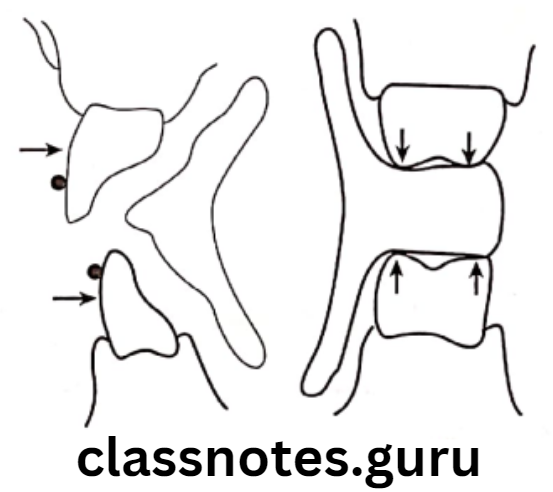
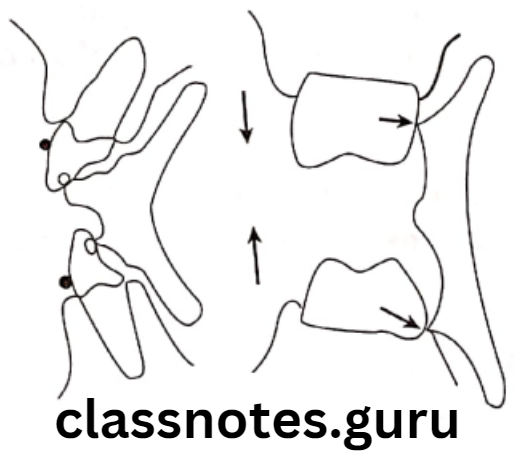
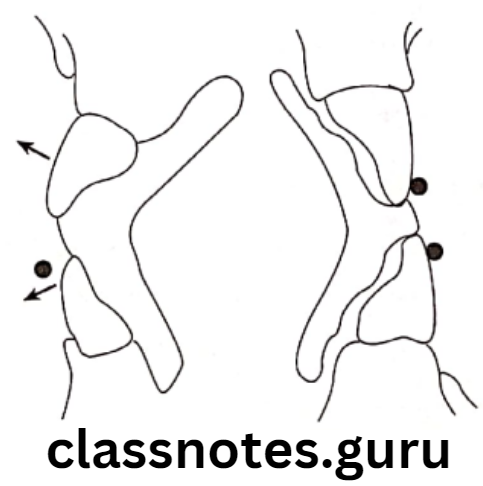
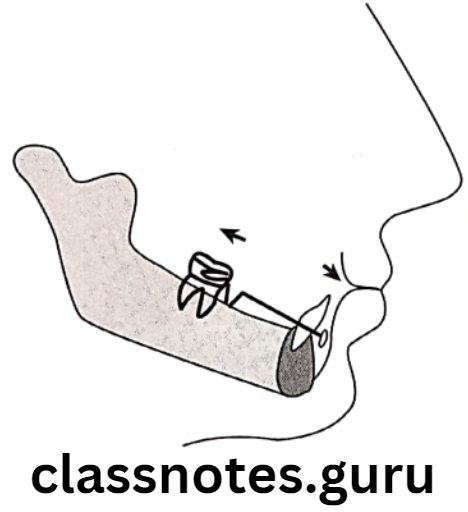
Mode of Action Of Myofunctional Appliances:
- Prevents dentoalveolar growth of maxilla
- Moves it distally
- Move mandible forward
- Stretches elevator muscles
- Adaptation of condyle
Question 3. Classify myofunctional appliances. Describe indications, construction and trimming of the activator.
Answer.
Classification Of Myofunctional Appliances:
- According to Tom Graber
- Group A – Teeth supported Ex. Catlan’s appliance
- Group B – Teeth/tissue supported
Example. Activation - Group C – Vestibular positioned Ex. Lip bumper
- Removable – Activator
- Semifixed – Bass appliance
- Fixed – Herbst
- Classical – Activator
- Hybrid – Bass
- Teeth borne passive – Activator
- Tooth borne active – Elastic open activator
- Tissue-borne passive-oral screen
- Tissue borne active – FR
- Functional orthopaedic magnetic appliance
Activator Of Myofunctional Appliances:
- Activator is myofunctional appliance described by Andresen and Haupl
Indications Of Myofunctional Appliances:
- Class 1 open bite
- Class 1 deep bite
- Class 2 div. 1
- Class 2 Div 2
- Class 3
- Preliminary treatment
- Post-treatment retention
- Decreased facial height
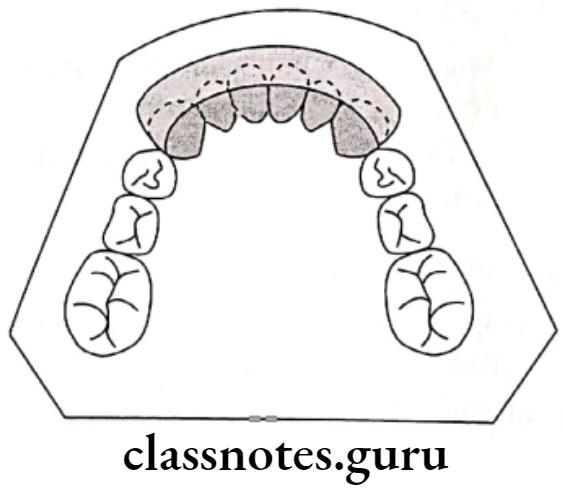
Construction Of Myofunctional Appliances:
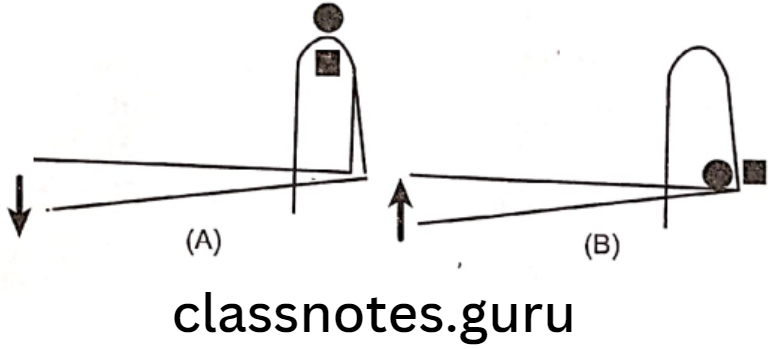
Trimming:
For Vertical control:
- Intrusion:
- Acrylic – Over incisal edge/cusp tips
- Labial bow – Below the height of the contour initially
- Extrusion:
- Acrylic – Lingual surface
- Labial bow – Above the height of contour gingivally
For Sagittal control: - Protrusion
- Acrylic – lingual surface
- Labial bow – Passive, away from teeth
Retrusion:
- Acrylic – Away from the lingual surface
- Labial bow – Active
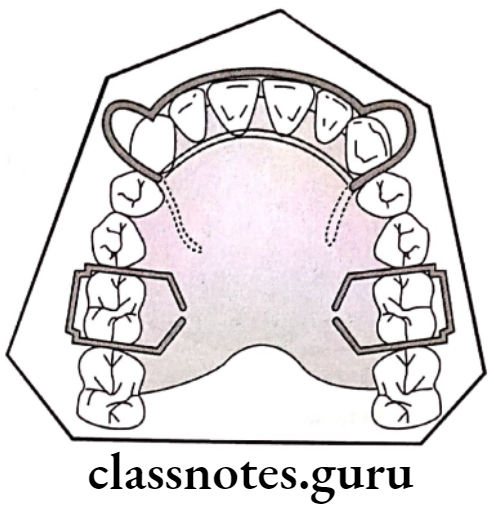
Movement of posterior teeth in the sagittal plane:
- In class 2 – Acrylic over the mesial lingual surface of maxillary molars
- Distolingual surface of mandibular molars
Movement of teeth in the transverse plane:
Myofunctional Appliances Short Essays
Question 1. Jasper jumper.
Answer.
Jasper jumper is a flexible, fixed tooth-borne appliance introduced by Jasper in 1980
Jasper jumper Indications:
- Class 2 malocclusion with maxillary excess and mandibular deficiency
Effects Of Jasper jumper
- Skeletal effects:
- Holds and displaces maxilla distally with a small shift of point A distally
- Clockwise rotation of the mandible
- Forwarded movement of condyles
- Dental changes:
- Posterior tipping and intrusion of upper molars and palatal tipping of maxillary incisors
- Anterior translation and tipping of mandibular teeth and intrusion of mandibular incisors
Jasper jumper Advantages:
- It produces continuous forces
- Allows a greater degree of mandibular freedom
- It is easier to maintain better oral hygiene
Question 2. Name components of FR2 and describe the uses of buccal shields.
Answer.
Components Of FR2:
Acrylic component:
- Buccal shields
- Lip pads
- Lower lingual pad
Wire component:
- Labial bow
- Canine extensions
- Palatal bow
- Upper lingual wire
- Lower lingual springs
- Lingual cross-over wire
- Support wire for lip pads
Use of Buccal Shields:
- Prevents abnormal muscular forces
- Creates forces on tissue
- This leads to bone formation
- Rehabilitates muscles
- As it stands away from posterior teeth, it allows their eruption
Question 3. Mode of action of functional appliance.
Answer.
Force Application:
Force Elimination by
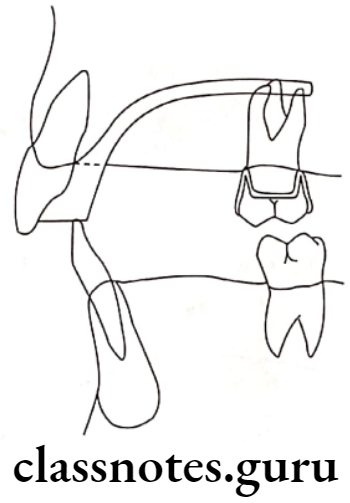
- Bite planes – Effects:
- Disocclude the posterior teeth
- Differential eruption of posteriors
- Intrusion of incisors
- Downward and backward mandibular rotation
- Reduces mandibular prognatism
- Shields/Screens – Effects:
- Prevents muscular forces on dentoalveolar structures
- Allows unrestricted growth of the jaw
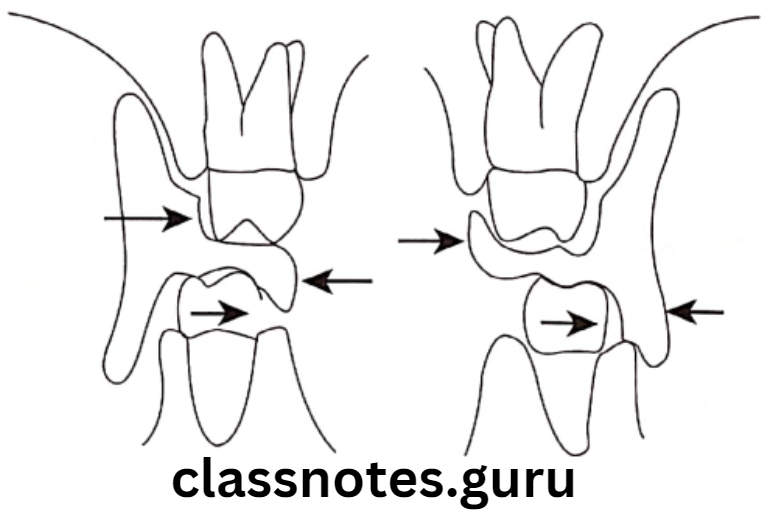
- Construction bite – Effects:
- Displaces mandible from its rest position
- Stretches muscles
- Displaces mandible in sagittal and transverse plane
Question 4. Case Selection for Functional Appliances.
Answer.
Factors Considered:
Age – Growing patient:
- Between 10 years of age and pubertal growth phase
Social considerations:
- Patients living far from the clinic
- Hostelites
Dental considerations:
- Uncrowded cases
- Local irregularities
Skeletal considerations:
- Moderate to severe skeletal class 2 malocclusions
- Low angle cases
- High-angle cases with deep bites
- Class 2 Division 2
- Mild class 3 malocclusions
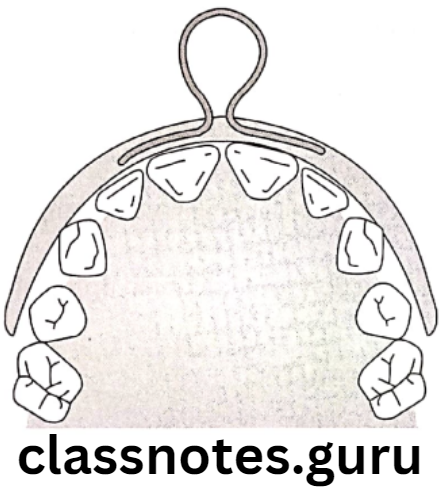
Question 5. Oral Screen.
Answer.
Synonym – Vestibular Screen:
- Introduced by Newell in 1912
Principle Of Oral Screen:
- Application of muscular forces to teeth by applying forces of circumoral to teeth
- Elimination of forces to teeth and allow them to move due to forces exerted by the tongue
Oral Screen Indication:
- Interception of habits
- Treatment of mild malocclusions
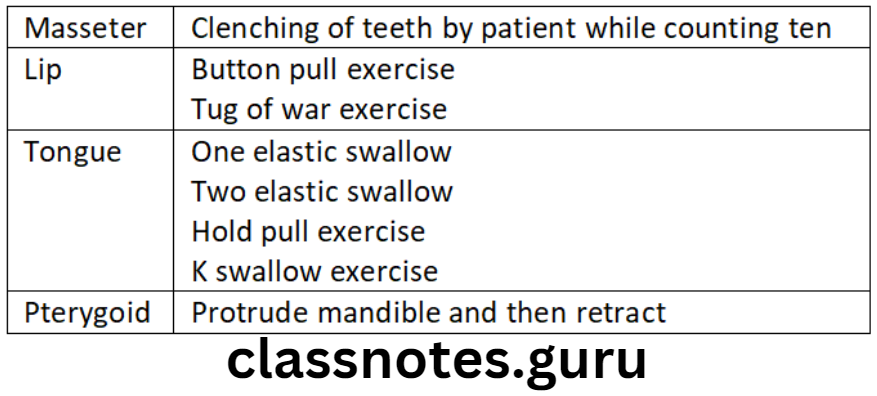
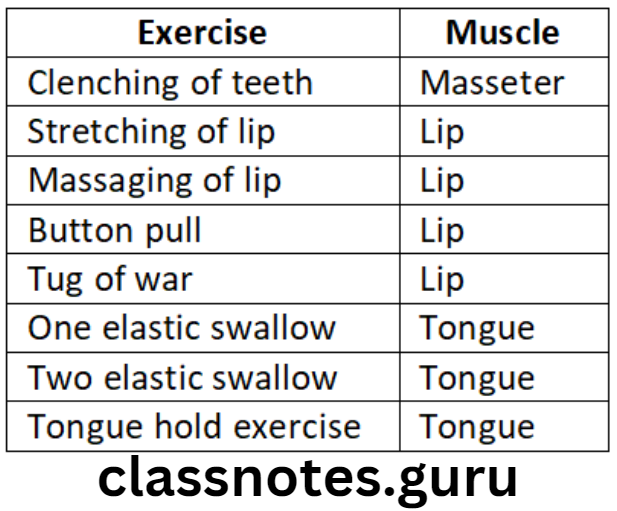
- For muscular exercises
- Correction of mild anterior proclination
Management Of Oral Screen:
- Frequency of wear – During the night 2-3 hours during day time
Question 6. Frankel 2.
Answer.
Uses of Frankel 2 – For treatment of class 2 division 1 and division 2 malocclusion.
Components Of Frankel 2:
Acrylic:
- Buccal shields
- Lip pads
- Lower lingual pad
Wire:
- Palatal bow
- labial bow
- canine extension
- Upper lingual wire
- Lingual cross-over wire
- Support wire
- Lower lingual spring
Functions Of Frankel 2:
Acrylic components:
- Eliminate the muscle as well as lip function over the dentoalveolar segment
Wire component:
- Palatal bow – Prevent supra eruption of posteriors
- Canine loops – Help in transverse development in the canine region
- Labial bow – Passive
- Lingual stabilizing bow – Prevents lingual tipping of incisors
- Lower lingual springs – Screen tongue pressure
- Procline lower incisors
- Lingual cross-over wire
- Labial support wires – Support lip pads
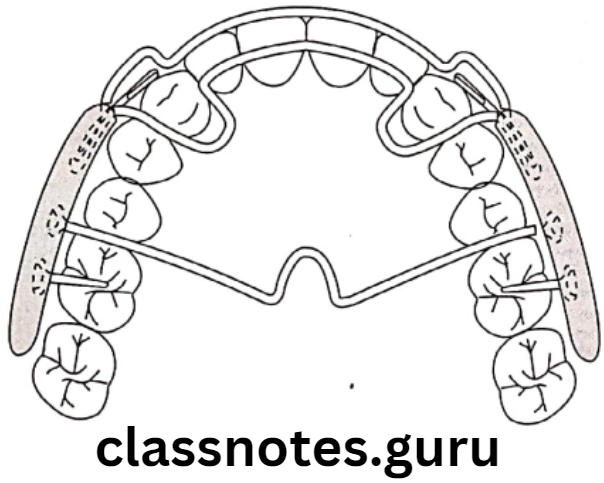
Question 7. Explain the treatment procedure in a child of 8 years with a deficient maxilla, the appliance used and the mode of action.
Answer.
An 8 years old child is a growing child
- Thus my function appliance can be used to facilitate the change
- Among them, Frankel regulator 3 can be used
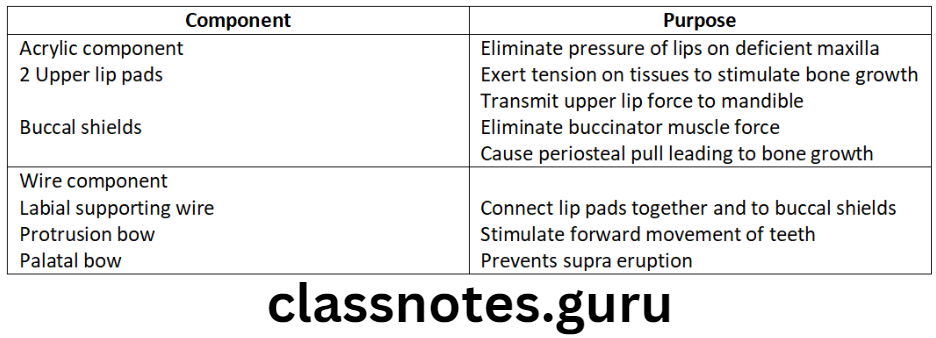

Mode of Action:
- In transverse and sagittal intraoral space
- By acrylic component
- In vertical space
- As the appliance is kept free from posterior teeth
- Muscle function adaptation
- Overcomes abnormal perioral muscle activity
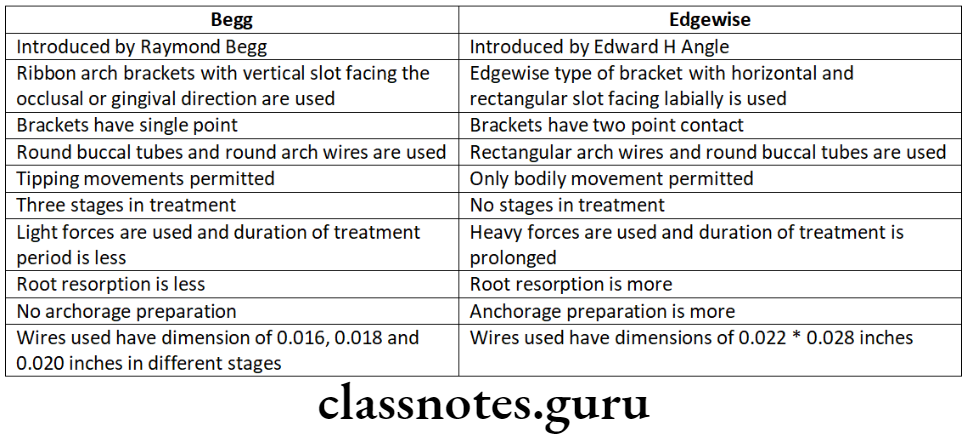
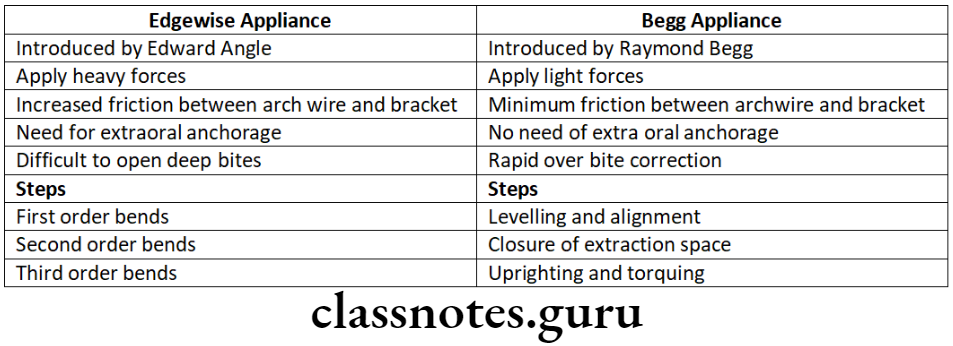
Question 8. Difference between Activator and Frankel Appliance.
Answer.
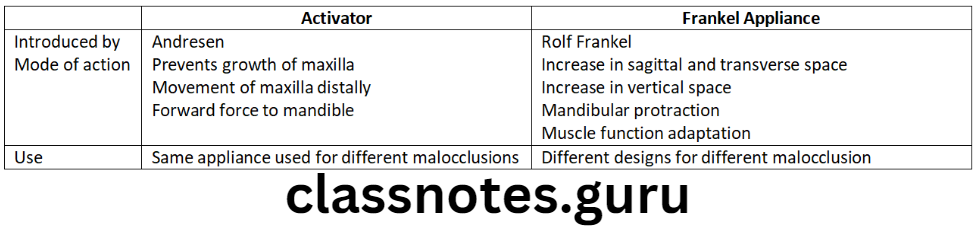
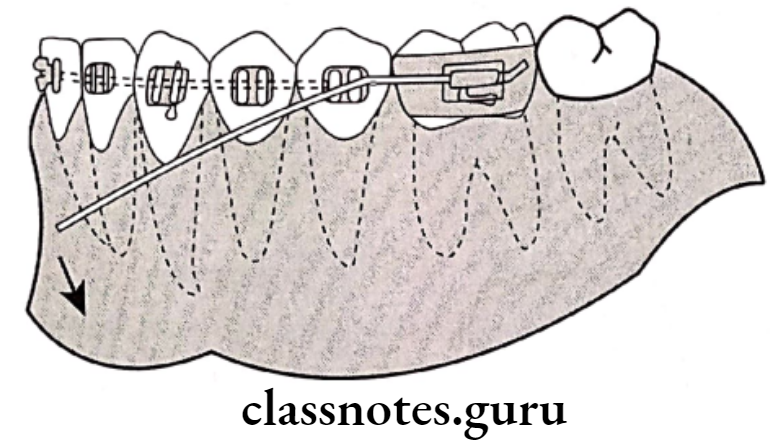
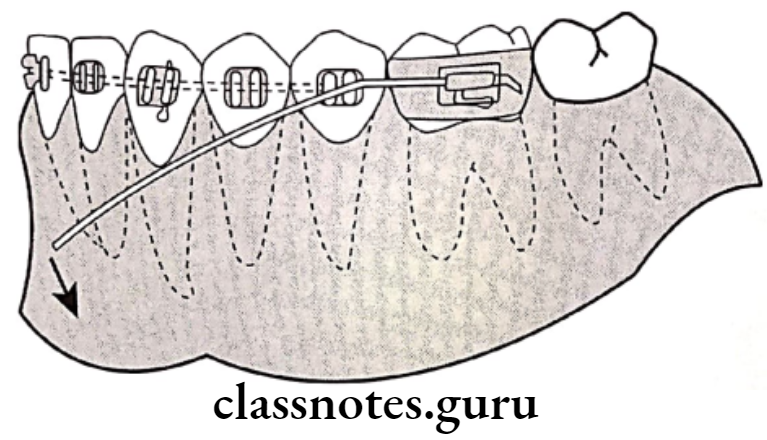
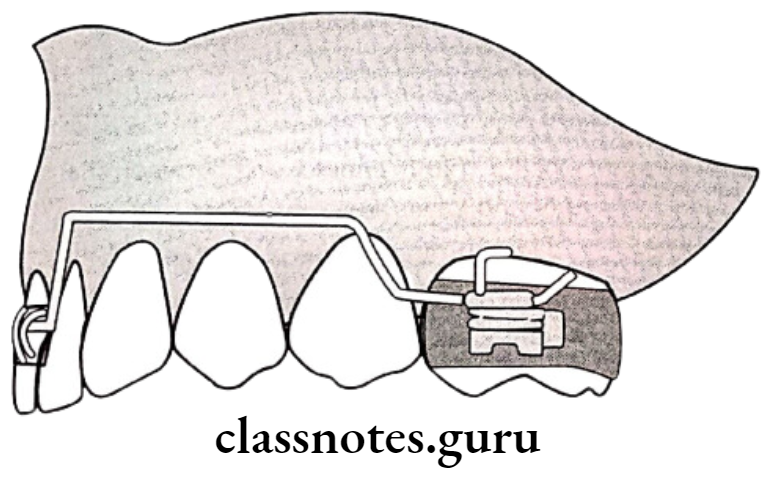
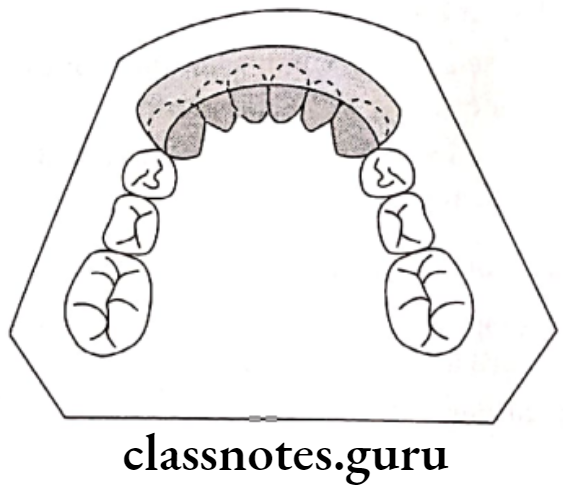
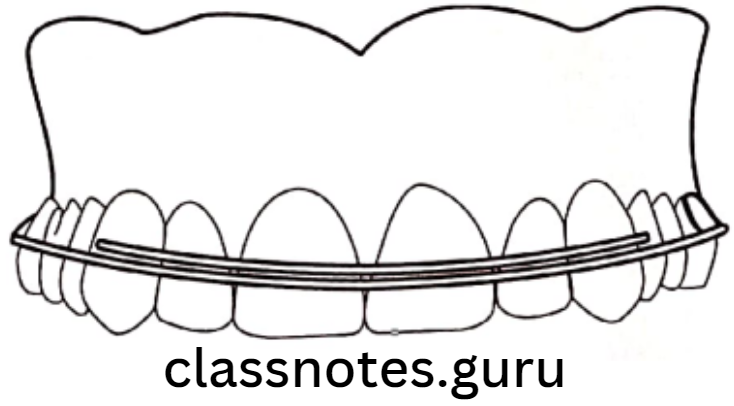
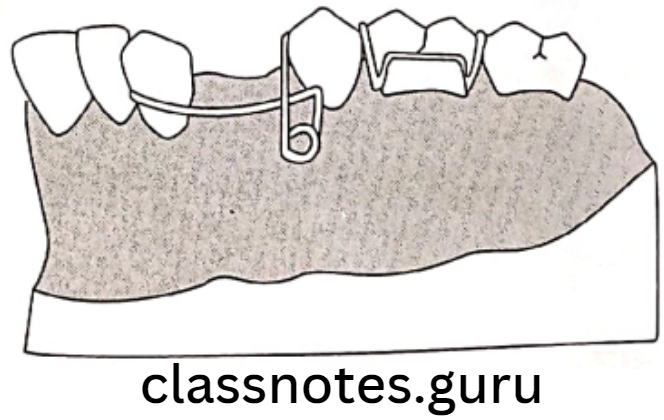
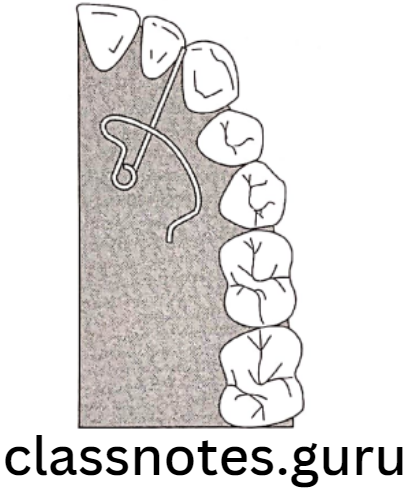
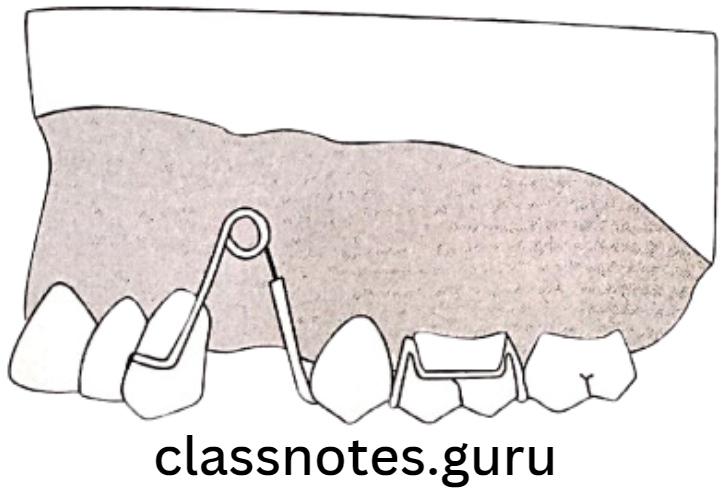
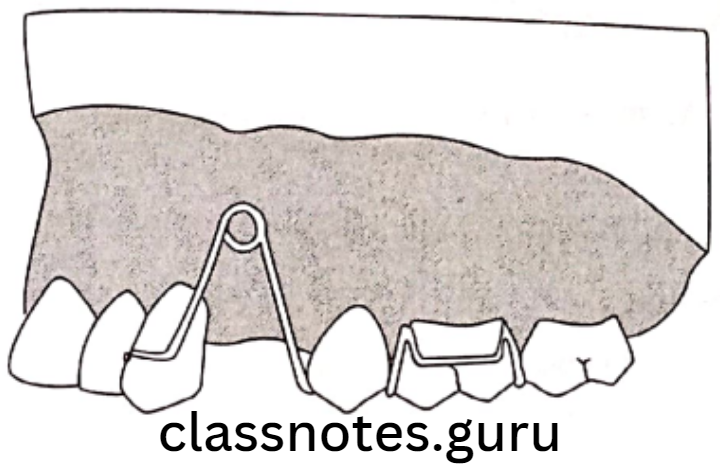
Question 9. Lip Bumper.
Answer.
Combined removable fixed appliance
Mode of Action:
- Force application/elimination
Uses Of Lip Bumper:
- Interception of lip biting habits
- Increases arch length
- Reduces crowding
- In the case of active mental activity
- For augmentation of anchorage
- For visualization of 1st molar
- Used as space regainer
Designs Of Lip Bumper:
- Stainless steel wire from one molar to the opposite molar passing away from the anterior
- Acrylic portion from canine to canine
Myofunctional Appliances Short Questions And Answers
Question 1. Herbst Appliance.
Answer.
By Emil Herbst in the early 1900’s.
Herbst Appliance Indications:
- Post-adolescent patient – treatment of Class 2
- TMJ disorders
- Interception of mouth breathing habit
Types Of Herbst Appliance:
- Banded Herbst
- Bonded Herbst
Effects Of Herbst Appliance:
- Class 1 molar correction
- Increase in mandibular growth
- Visualization of molar
- Reduction of over-jet
- Increase SNB and decrease SNA
Question 2. Twin Block.
Answer.
Design: Consist of inclined planes with intermaxillary and extraoral traction
Acrylic Components:
- Upper inclined plane – Covering lingual cusps of upper posterior till mesial ridge of upper 2nd PM [Premolar]
- Lower inclined plane – From lower anterior upto distal marginal ridge of 2nd premolar
- The angle between them – 45
Wire components:
- Modified arrow head clasp – To retain the upper plate
- Molar tube – for attachment of face bow
- Jack screw – for maxillary expansion
- Interdental ball clasp – Retain lower plate
Myofuctional Appliances Viva Voce
- Reverse binator is used for Angle’s class 3 malocclusion
- Newell developed an oral screen
- Lip bumper should be worn for 24 hours a day
- Myofunctional appliances harness natural forces from perioral structures
- Oral screening works on both force application and force elimination principle
- Twin block is the most acceptable functional appliance