Blood Supply And Lymphatic Drainage Of Upper Limb Question And Answers
Question 1. Outline the arterial supply of upper limb.
Answer:
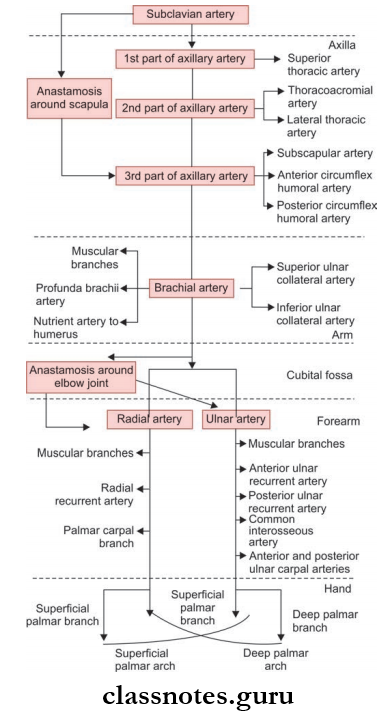
The Arterial Supply Of Upper Limb
- From the arch of the aorta, the brachiocephalic trunk originates.
- The subclavian artery is the main branch of this trunk.
- The subclavian artery continues as the axillary artery.
- The axillary artery enters and gives blood supply to the upper limb.
Read And Learn More: Anatomy Question And Answers
Question 2. Explain in detail about the axillary artery under the headings—beginning, course, relations, branches, and termination.
Answer:
Axillary Artery
Axillary Artery is the continuation of the subclavian artery and gives blood supply to the upper limb.
Axillary Artery Beginning
- At the outer border of the first rib as a continuation of the subclavian artery.
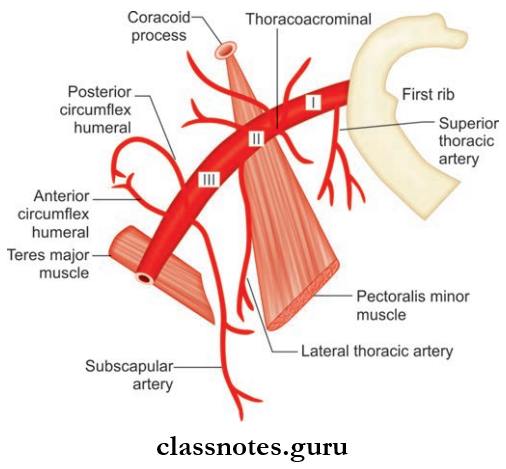
Axillary Artery Course
- It runs from the apex to the base of the axilla along the lateral wall closer to the anterior wall than the posterior wall.
- During its course, it is crossed by the pectoralis minor muscle which divides it into three parts:
- The first part is superior or proximal to the muscle.
- The second part, posterior or deep to the muscle
- Third part is inferior or distal to the muscle.
Axillary Artery Relations
- First Part
- Axillary artery and cords of brachial plexus are enclosed in an axillary sheath
- Lateral and posterior cords are lateral to the axillary artery
- Medial cord lies posterior to axillary artery
- Second Part
- Cords are arranged according to their name
- Lateral cord lies lateral to artery
- Medial cord lies medial to artery
- Posterior cord lies posterior to artery
- Third Part
- Superolaterally musculocutaneous nerve and inferolaterally median nerve lies
- The ulnar nerve lies medial to axillary artery
- Posterosuperiorly axillary nerve and posteroinferiorly radial nerve lies
Read And Learn More: Anatomy Question And Answers
Axillary Artery Branches Of
- First Part
- Superior thoracic artery
- Supplies the muscles and medial wall of axilla
- Second Part
- Thracoacromial artery
- Gives of 4 branches right angle to each other, supplying pectoral muscles and sternoclavicular joint
- Lateral thoracic artery
- It supplies pectoralis major, pectoralis minor, and serratus anterior muscles
- In females, it supplies breasts also
- Third Part
- Subscapular artery
- It is the largest branch of the axillary artery.
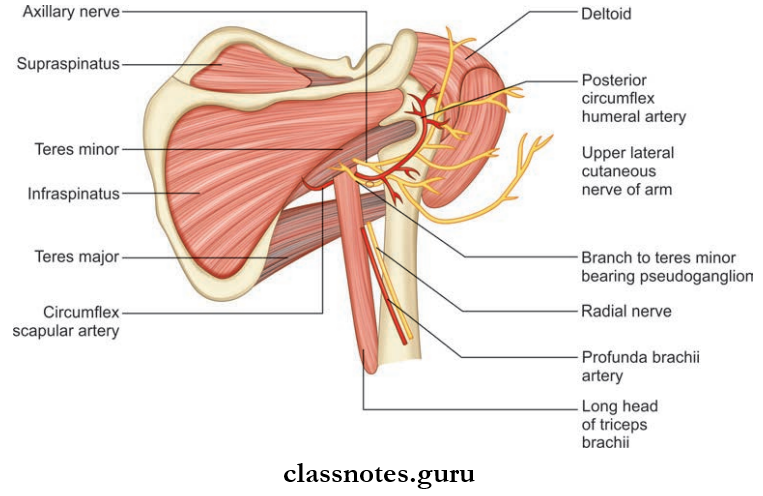
- It gives of circumflex scapular artery which passes through upper triangular intermuscular space to reach the infraspinatus fossa.
- Anterior circumflex humeral artery
- It passes in front of the surgical neck of the humerus and anastomoses with the Posterior circumflex humeral artery.
- It gives of an ascending branch to give blood supply to the head of the humerus and shoulder joint.
Question 3. Write a note on anastomosis around scapula.
Answer:
Anastomosis Around Scapula
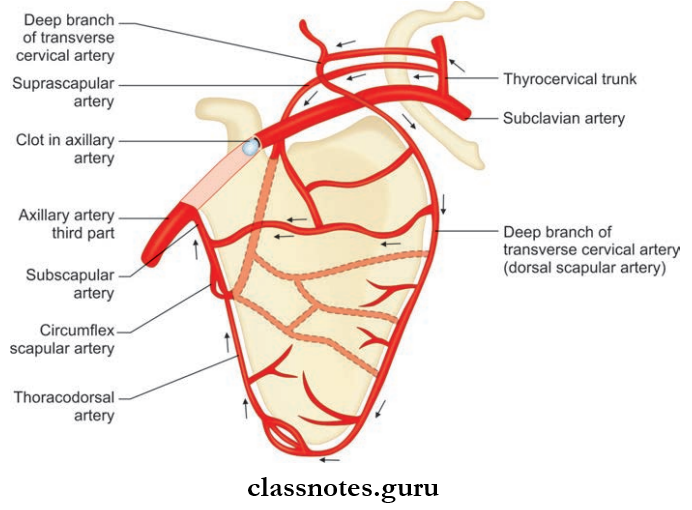
- Anastomosis around scapula is formed between the branches of the first part of subclavian artery and third part of the axillary artery
- It basically occurs at two sites:
- Around the body of scapula
- The arterial branches contributing to this are:
- Suprascapular artery (branch of thyrocervical trunk from the subclavian artery)
- Deep branch of the transverse cervical artery (branch of thyrocervical trunk form the subclavian artery)
- Circumflex scapular artery (branch of the third part of an axillary artery).
- Over the acromion process
- The arterial branches contributing to this are:
- Acromial branch of the suprascapular artery (branch of the subclavian artery)
- Acromial branch of the thoracoacromial artery (branch of an axillary artery)
- Acromial branch of the posterior circumflex humeral artery (branch of an axillary artery).
Anastomosis Around Scapula Clinical Anatomy
If anywhere between the first part of the subclavian and the third part of the axillary artery is blocked, anastomosis around the scapula opens, and collateral circulation comes into action to ensure adequate blood supply to the upper limb.
Question 4. Explain in detail about the brachial artery under the headings—beginning, course, relations, branches, and termination.
Answer:
The Brachial Artery Is The Main Artery Of The Arm.
Brachial Artery Beginning
- It is the continuation of the axillary artery from the lower border of the teres major muscle.
Brachial Artery Course
- It runs downwards and laterally in front of the arm to cross the elbow joint.
- After crossing, at the level of the neck of radius, it divides into radial and ulnar arteries in the cubital fossa.
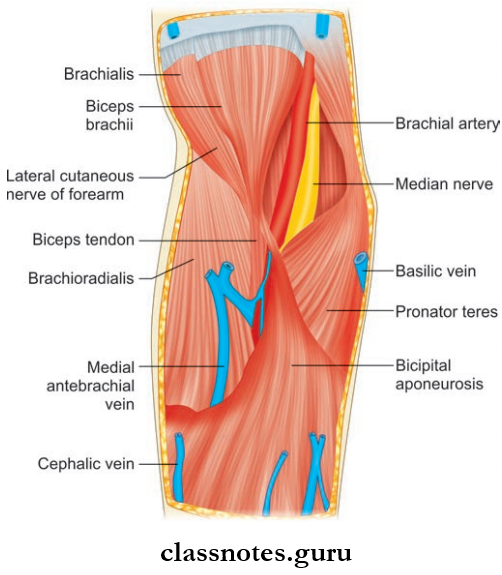
Brachial Artery Relations
- It is superficial throughout its course and is accompanied by venae comitantes.
- Anteriorly
- The median nerve crosses from lateral to the medial side in the middle of the arm
- Bicipital aponeurosis and medial cubital vein cover the artery in the elbow joint
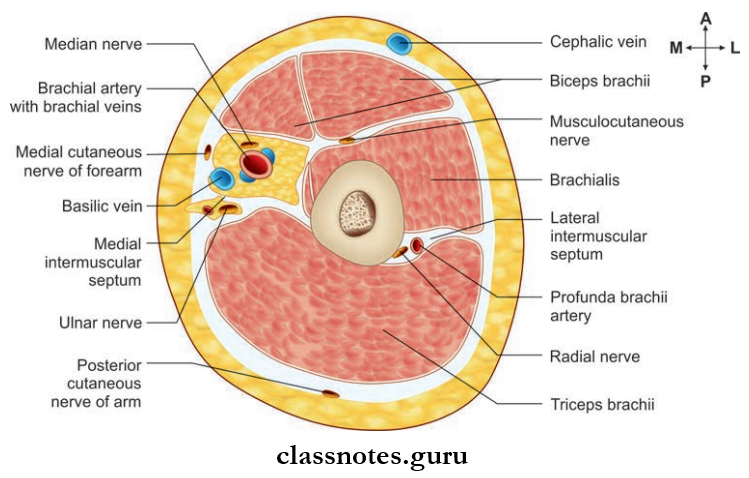
- Posteriorly
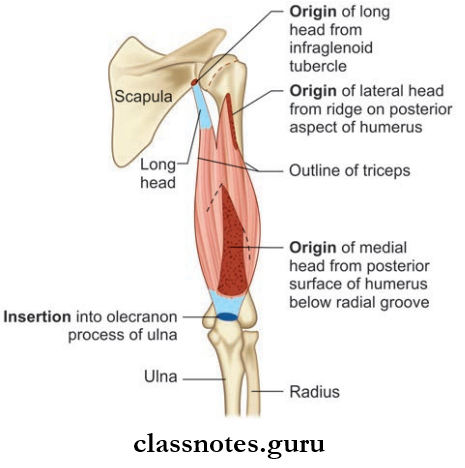
- Triceps brachii
- Radial nerve and profunda brachii artery
- Medially
- Upper part related to ulnar nerve and basilica vein
- Lower part related to the median nerve
- Laterally
- The upper part related to coracobrachialis, biceps brachii, and median nerve
- Tendon of biceps brachii in the elbow
- In the elbow, the structures from the medial to lateral side are:
- Median nerve
- Brachial artery
- Biceps brachii tendon
- Radial nerve (deeper)
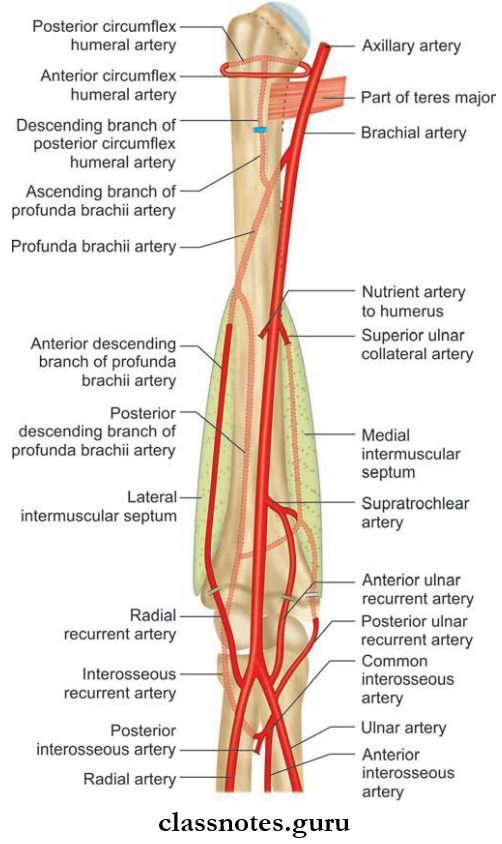
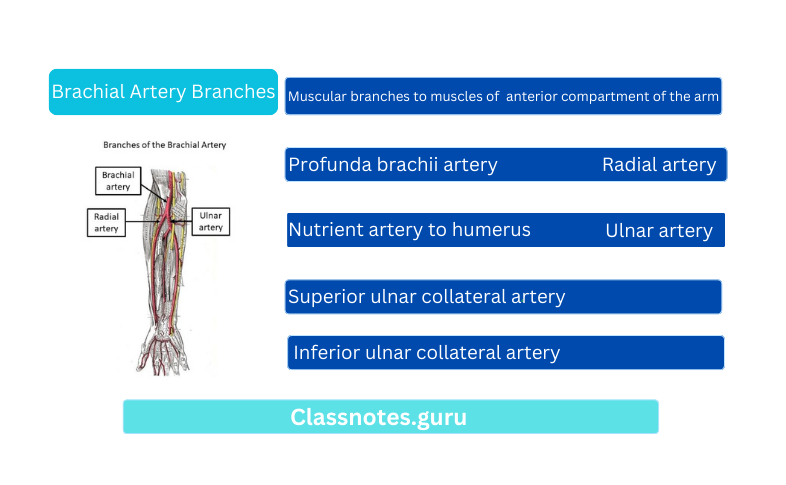
Brachial Artery Branches
- Muscular branches to muscles of anterior compartment of the arm
- Profunda brachii artery
- Nutrient artery to humerus
- Superior ulnar collateral artery
- Inferior ulnar collateral artery
- Radial artery
- Ulnar artery
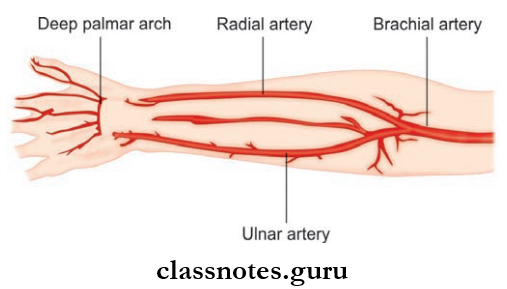
Brachial Artery Termination
- The brachial artery divides into radial and ulnar arteries in the cubital fossa at the level of neck of radius.
Brachial Artery Clinical Anatomy
- Brachial artery pulsations can be felt in the cubital fossa medial to the tendon of the biceps brachii. The pulsations are used in measuring blood pressure in auscultatory method.
- Injury to the brachial artery is one of the major complications in the supracondylar fracture of the humerus.
Question 5. Write a short note on anastomosis around the elbow joint.
Answer:
Anastomosis Around The Elbow Joint
- Anastomosis around elbow joint connects brachial artery with the upper end of radial and ulnar arteries.
- This anastomosis nourishes the ligaments and bones of the elbow joint.
- It exits:
- In front of medial epicondyle
- In front of lateral epicondyle
- Behind medial epicondyle
- Behind lateral epicondyle
- Above the olecranon fossa.
Anastomosis Around Elbow Joint Clinical Anatomy
- This anastomosis becomes more significant when a block or injury occurs anywhere between the brachial artery and radial and ulnar arteries.
Question 6. Explain about radial artery under the headings—beginning, course, relations, branches, and termination.
Answer:
Radial Artery
Radial Artery Beginning
- In the cubital fossa brachial artery divides into radial and ulnar arteries.
- Radial artery is the smaller terminal branch of the brachial artery.
Radial Artery Course
- It is more superfiial compared to ulnar artery.
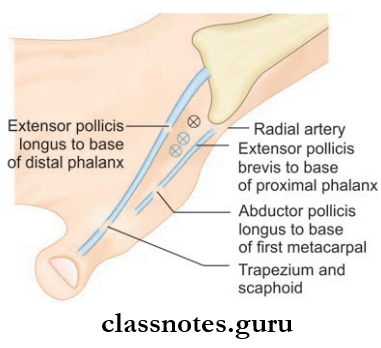
- It runs downwards along the convexity of the lateral side of the forearm and turns posteriorly to reach the anatomical snuf box in the arm.
- From the anatomical snuff box, radial artery enters the palm where it continues as deep palmar arch.
Radial Artery Relations: It is accompanied by two venae comitantes.
- Anteriorly
- Brachioradialis in the upper part
- Skin, superficial and deep fascia in the lower part
- Posteriorly
- The muscles attached to the anterior surface of the radius
- Medially
- Pronator teres in the upper 1/3rd
- Tendon of flexor carpi radialis in the lower 2/3rd
- Laterally
- Brachioradialis
- Radial nerve
Radial Artery Branches
- Muscular branches
- Radial recurrent artery
- Palmar carpal branch
- Superficial palmar branch: Joins with the terminal branch of the ulnar artery to continues as superficial palmar arch.
Radial Artery Termination It continues as deep palmar arch in the palm.
Radial Artery Clinical Anatomy
- The radial pulse is routinely palpated in the general examination of patients.
- It is felt at the ventral aspect, just above the wrist against the radius bone where the radial artery is covered by only skin and superficial fascia.
Question 7. Explain about ulnar artery under the headings—beginning, course, relations, branches, and termination.
Answer:
Ulnar Artery Beginning
- In the cubital fossa brachial artery divides into radial and ulnar arteries.
- Ulnar artery is the larger terminal branch of the brachial artery.
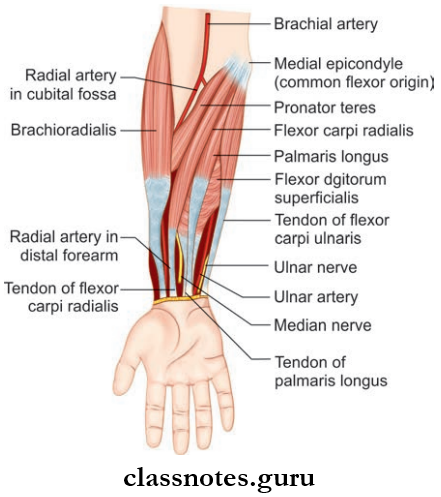
Ulnar Artery Course
- In the upper 1/3rd of the forearm, ulnar artery runs obliquely downwards to reach the anterolateral aspect.
- In the lower 2/3rd of the forearm, the ulnar artery runs vertically downwards.
- It enters the palm superfiial to flxor retinaculum.
Ulnar Artery Relations: Ulnar artery is accompanied by two venae comitantes.
- Anteriorly
- Muscles arising from the common flexor origin and median nerve in the upper half
- Skin and superficial fascia in the lower half
- Posteriorly
- Brachioradialis
- Flexor digitorum profundus
- Medially
- Ulnar nerve
- Flexor carpi ulnaris
- Laterally
- Flexor digitorum superfiialis
Ulnar Artery Branches
- Muscular branches
- Anterior and posterior ulnar recurrent arteries
- Common interosseous artery
- Anterior and posterior ulnar
- Superfiial palmar branch:
- Continues as a superficial palmar arch to anastomose with superficial palmar branch of radial artery
- Deep palmar branch:
- Anastomoses with the direct continuation of the radial artery to form deep palmar arch.
Question 8. Write a note on the superficial palmar arch.
Answer:
Superficial Palmar Arch
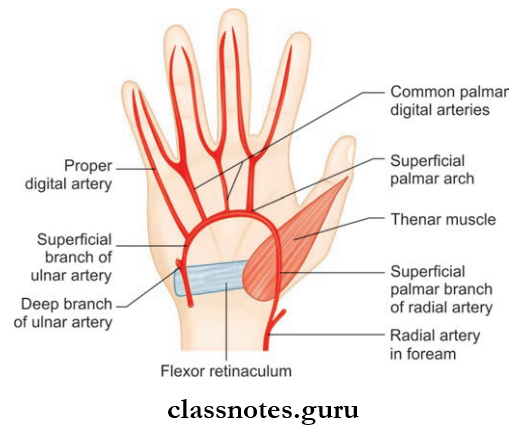
- It is formed by the anastomosis of ulnar artery with radial artery in the hand.
- It is an arterial arch and the convexity is directed toward the fingers.
Superficial Palmar Arch Formation
- It is formed by the direct continuation of the ulnar artery (superficial palmar branch) beyond the flexor retinaculum.
- The superficial palmar branch arches in the palm and finally anastomose with the superficial palmar branch of the radial artery on the lateral side and completes the arch.
Superfiial Palmar Arch Relations
- Superficial
- Deep
- Flexor tendons of flxor digitorum superfiialis and flxor digitorum profundus
- Lumbricals
- Digital branch of ulnar and median nerves.
Superficial Palmar Arch Branches
- Four digital arteries
- Cutaneous branches to the palm.
Question 9. Write a note on the deep palmar arch.
Answer:
Deep Palmar Arch
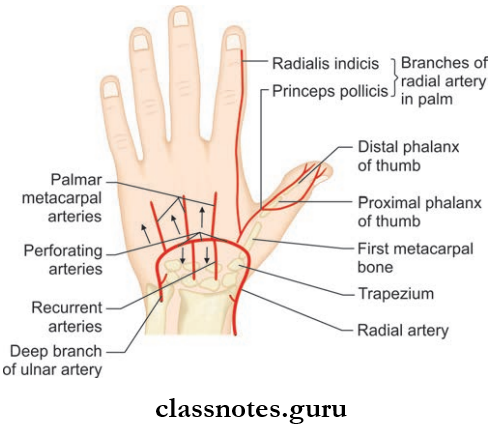
- It is the direct continuation of the radial artery
- The convexity is towards fingers
- The arch is completed by the anastomosis with deep palmar branch of the ulnar artery.
Deep Palmar Arch Relations
- Superficial
- Long flexor tendons of fingers
- Lumbricals
- Deep
- Metacarpals
- Interosseous muscles
Question 10. Give an outline of venous drainage of upper limb.
Answer:
Venous Drainage Of Upper Limb
- Venous drainage of upper limb is divided into two groups:
- Superficial
- Deep
- The superficial group of veins are located in the superficial fascia
- Deep groups of veins are located deep to the muscles and accompany arteries known as venae comitantes.
Question 11. What are the main superficial veins of the upper limb? Describe about each of them mentioning their formation, tributaries, course, and termination.
Answer:
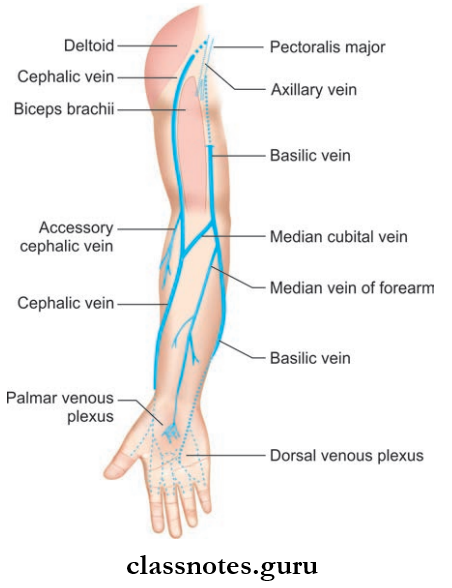
Main Superficial Veins Of The Upper Limb
- They lies in the superficial fascia.
- They runs away from the pressure points, so they are absent in the palm, along the ulnar border of the forearm, and in the back of the arm. Due to this reason, they are having a spiral course, from the dorsal surface of hand to ventral surface of the arm.
- They comprise of:
- Dorsal venous arch
- Cephalic vein
- Basilic vein
- Median cubital vein.
Superficial Veins Of Upper Limb Dorsal Venous Arch
- It is a network of veins situated on the dorsum of hand.
- Tributaries
- Three dorsal metacarpal veins
- A dorsal digital vein from the medial side of little finger
- A dorsal digital vein from the radial side of the index finger
- Two dorsal digital veins of the thumb
- Veins draining palm of hand
- Dorsal venous arch drains into cephalic and basilic veins.
Superficial Veins Of Upper Limb Cephalic Vein
- It is the preaxial vein of upper limb and is homologous with the great saphenous vein of lower limb.
- Cephalic Vein Formation
- It is the continuation lateral end of the dorsal venous arch.
- Cephalic Vein Course
- It runs over the roof of the anatomical snuff box and ascends along the radial border of the forearm. It continues upwards in front of elbow joint and lateral border of biceps brachii to pierce deep fascia at the lower border of the pectoralis muscle
- From there, it runs in the cleft between the deltoid and pectoralis muscle up to the infraclavicular fossa where it pierces the clavipectoral fascia to drain into the axillary vein
- The cephalic vein is accompanied by the lateral cutaneous nerve of the forearm.
- Cephalic Vein Termination
- The cephalic vein after piercing the clavipectoral fascia, drains into the axillary vein.
Superficial Veins Of Upper Limb Basilic Vein
- It is the postaxial vein of upper limb and is homogenous with that of the short saphenous vein of lower limb.
- Basilic Vein Formation
- It is the continuation of the medial end of the dorsal venous arch.
- Basilic Vein Course
- It ascends along the back of the medial border of the forearm and winds around the border below the level of the elbow joint to reach in front of the forearm.
- From there, it ascends upwards along the medial border of biceps brachii and pierces the deep fascia at the level of the middle of the arm.
- Under the deep fascia, it joins with the brachial veins and run along the medial side of the brachial artery to continue as the axillary vein.
- Basilic Vein Termination
- It continues as the axillary vein at the level of the lower border of the teres major.
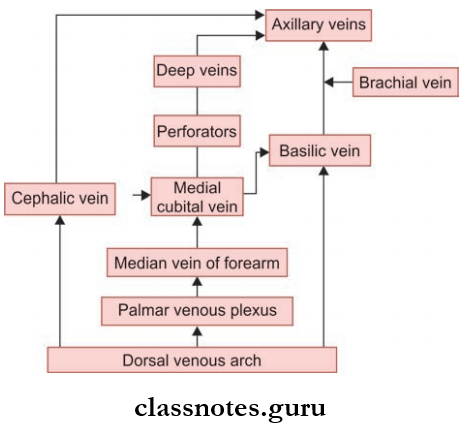
Median Cubital Vein
- It is a venous channel between the cephalic and basilic veins in the cubital fossa.
- The cephalic vein is carrying a larger quantity of impure blood compared to more efficient basilic vein.
- So medial cubital vein shunts the extra volume of blood from the cephalic to the basilic vein ensuring efficient venous drainage.
- It begins from the cephalic vein 2.5 cm below the bend of the elbow.
- It runs obliquely upwards and medially.
- It terminates in a basilic vein 2.5 cm above the bend of the elbow.
- The median vein of the forearm is one of the tributaries.
- Deep veins communicate with media cubital veins through perforators.
Question 12. List the deep veins of upper limb.
Answer:
Deep Veins Of Upper Limb They Comprise:
- Venae comitantes of radial, ulnar and brachial arteries
- Axillary vein
- They receive venous drainage from superficial veins.
Deep Veins Of Upper Limb Clinical Anatomy
- As the perforator veins fies the medial cubital vein, it is the favorite site of intravenous injections and blood withdrawals.
- Making a fit will increase the venous return as this activity squeezes the blood in the muscles of hand into the dorsal venous arch.
Question 13. Write a note on lymphatic drainage of upper limb.
Answer:
Lymphatic Drainage Of Upper Limb
Lymphatic drainage of upper limb consists of lymph vessels and nodes arranged as superficial and deep groups.
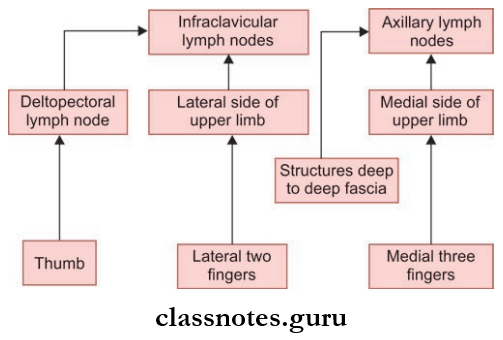
The Superficial Group Of Lymph Nodes Are:
- Infraclavicular nodes
- Deltopectoral nodes
- Superficial cubital/supratrochlear nodes.
The Deep Group of Lymph Nodes are:
- Axillary lymph node
- Deep cubital node.
Superficial Lymph Vessels
- They are located in the subcutaneous tissue.
- They are larger in number than deep lymph vessels.
- They drain lymph from the skin and subcutaneous tissues.
- Lymph vessels from the lateral side lateral of the upper limb including lateral two digits follow the cephalic vein and drain into the infraclavicular lymph node which is a superficial lymph node
- Lymph vessels from the medial side of the upper limb including the medial three digits follows the basilic vein and drain into a lateral group of axillary lymph node which is a deep lymph node.
- But some of the medial lymph vessels terminate in the supratrochlear or epitrochlear lymph nodes which are superficial lymph nodes.
- Few lymph vessels from the thumb drain into deltopectoral lymph nodes.
Deep Lymph vessels
- They are lesser in number than deep lymph vessels.
- They drain lymph from the structure deep to deep fascia including. For example, Muscles
- They follow the arteries and drains into a lateral group of axillary lymph nodes.
Deep Lymph Vessels Clinical Anatomy
- Lymphangitis is the inflmmation of lymph vessels and can occur due to injury to any part of the upper limb
- Axillary lymph nodes can become enlarged and painful followed by infections in any part of the upper limb.
Blood Supply And Lymphatic Drainage Of Upper Limb Multiple Choice Questions
Question 1. Epitrochlear lymph nodes are located along:
- Median cubital vein
- Cephalic vein above elbow
- Basilic vein above elbow
- Brachial artery
Answer: 3. Basilic vein above elbow
Question 2. Which is not a branch of deep palmar arch?
- Proximal perforation
- Recurrent
- Palmar metacarpal
- Common palmar digital
Answer: 4. Common palmar digital
Question 3. Which is not a branch of third part of the axillary artery?
- Thracoacromial artery
- Posterior circumflex humeral artery
- Subscapular artery
- Anterior circumflex humeral artery
Answer: 1. Thracoacromial artery
Question 4. Anastomosis around the scapula occurs between:
- The first part of the subclavian artery and first part of the axillary artery
- The first part of the subclavian artery and the third part of the axillary artery
- The second part of subclavian artery and first part of the axillary artery
- The second part of the subclavian artery and the third part of the axillary artery
Answer: 2. First part of the subclavian artery and the third part of axillary artery
Question 5. Anastomosis around the elbow joint exists at all these sites, except:
- Behind medial epicondyle
- Behind lateral epicondyle
- Above the olecranon fossa
- Around the neck of radius
Answer: 4. Around neck of the radius