
Neoplasia Important Notes
1. Exfoliative cytology or Pap smear
- It involves the study of cells that spontaneously shed off from epithelial surfaces into body cavities or body fluids
- It is based on the principle that malignant cells are incohesive and loose
- Thus they shed off into the lumen
- The cells are obtained by scraping, brushing or washing mucosal surfaces
2. Metastasis
- It is used to distinguish benign and malignant tumours
- Malignant tumours can metastasize
- Carcinomas metastasize through lymphatics while sarcomas through blood vessels
3. Oncogenic viruses
- These are viruses which induce carcinogenesis
- They may contain either DNA or RNA
Examples:
Neoplasia Long Essays
Question 1. Define neoplasia. Give the difference between benign and malignant tumours. Add a note on the paraneoplastic syndrome.
Answer:
Neoplasia Definition:
Neoplasia is defined as a mass of tissue formed as a result of the abnormal, excessive, uncoordinated, autonomous and purposeless proliferation of cells even after cessation of stimulus for growth which causes it.
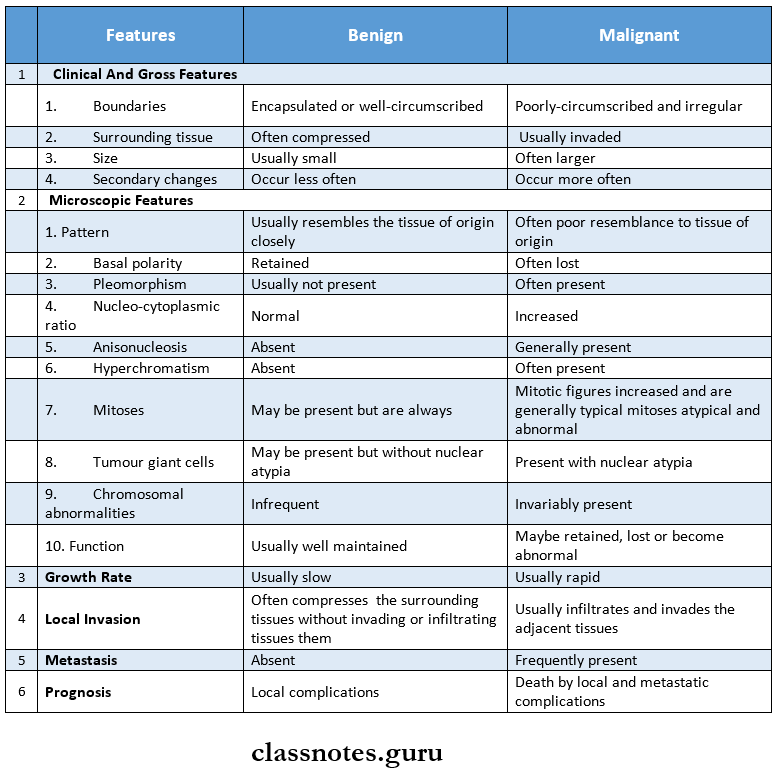
Differences between benign and malignant tumours:
Paraneoplastic Syndrome:
Para neoplastic syndromes are a group of conditions developing in patients with advanced cancer which are neither explained by direct and distant spread of the turn-over nor by the usual hormone elaboration by the tissue of origin of the tumour.
- They occur in 10% -15% of patients with cancer.
- Various clinical syndromes included in INS are.
- Endocrine syndrome.
- Hypercalcemia
- Cushing’s syndrome
- Polycythemia
- Flypoglycacmia.
- Endocrine syndrome.
Read And Learn More: Pathology Question And Answers
- Neuromyopathic syndromes
- Haematologic and vascular syndrome
- Gastrointestinal syndrome
- Renal syndrome
- Cutaneous syndromes
- Amyloidosis.
Question 2. Define neoplasia. Classify tumours. Discuss the mode of spread of malignant tumours.
Answer:
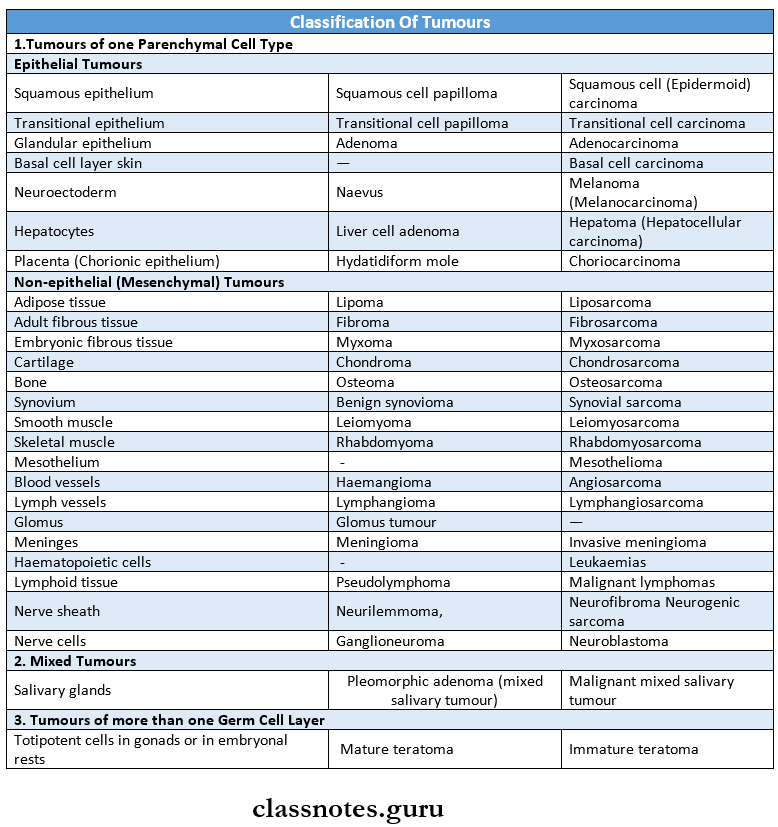
Classification of Tumours:
Spread of Tumours: It is by 2 ways.
1. Local invasion/direct spread:
- Benign tumours:
- Form encapsulated/circumscribed masses
- These that expand and push aside the surrounding normal tissues without actually invading, in- filtrating/metastasising.
- Malignant tumours: They also enlarge by expansion.
- These tumours invade via the route of least resistance
- Often cancers extend through tissue spaces, via lymphatics, blood vessels, and perineural spaces and may penetrate bone.
- More commonly, tumours invade thin-walled capillaries and veins than thick-walled arteries.
2. Metastasis/Distant spread:
- Metastasis is defined as the spread of tumours by inva¬sion in such a way that discontinuous secondary tumour mass/masses are formed at the site of lodgement.
- Benign tumours do not metastasise while all malignant tumours with a few exceptions like gliomas of the CNS and basal cell carcinoma of skin can me¬tastasis.
Routes of Metasis:
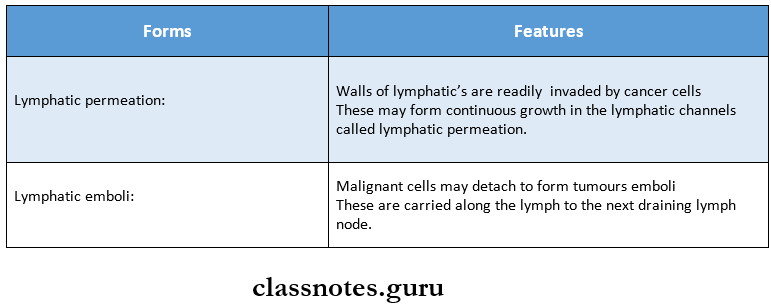
1. Lymphatic spread: In general, carcinomas metastasize by lymphatic route
Involvement of lymph nodes by malignant cells may be of two forms.
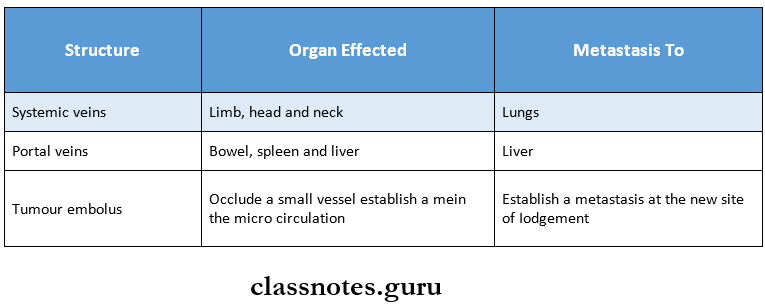
2. Haemategenous spread:
- Sarcomas spread through hematogenous spread
- The common site for blood-borne metastasis are
- Lung,
- Breast,
- Thyroid,
- kidney,
- Liberate and
- Ovary.
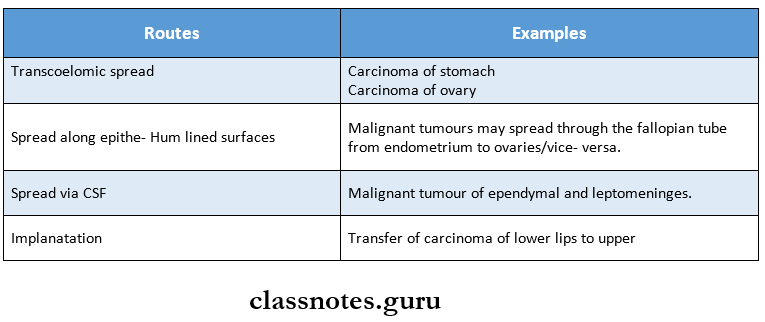
- Spread:
Various other routes:
Question 3. Define tumour. Write briefly about carcino¬gens. Describe gross and microscopic features of squamous cell carcinoma.
Answer:
- Tumour: Tumour is defined as a mass of tissue formed as a result of abnormal, excessive, uncoordinated, autonomous and purposeless proliferation of cells
- Carcinogens: The agents which can induce tumours are called carcinogens
Types of Carcinogens:
Squamous Cell Carcinoma Features:
- Age: common in older individuals
- Sites involved
- Lower lip
- Lateral tongue
- The floor of the mouth
- Soft palate
- Gingiva
- Alveolar ridge
- Buccal mucosa
- Presentation
- Initially asymptomatic lesion
- Resembles leukoplakia
- Appears as a white or red nodule or fissure over the mucosa
- The advanced lesion appears as rapidly enlarging exo-phytic growth or ulcer or tumour-like mass
- The ulcer has persistent induration around the periph¬ery with elevated and everted margins
- May predispose candidal infections
- May be a secondary infected
Squamous Cell Carcinoma Morphology:
Gross appearance:
- It appears as nodular or lucrative growth
- Shows fungating and polypoid mass without ulceration
- Margin- elevated and indurated
Cut section
It shows grey-white endophytic as well as exophytic tumours
Microscopic appearance
- It is characterised by malignant cells
- These cells show variable degrees of differentiation
- Cells invade through the basement membrane into the dermis
Arrangement
- Cells are arranged in concentric layers called epithelial pearls
- They contain keratin material in the centre of the cell masses
- Cells are separated by lymphocytes
Question 4. Discuss about injury caused by ionizing radiation.
Answer:
- Ionizing radiation like X-rays, alpha, beta and gamma rays can cause cancer
- Cancer caused by them are
- Cancer of
- Thyroid
- Skin
- Breast
- Ovary
- Uterus
- Lung
- Myeloma
- Salivary glands
- Leukaemia
- Cancer of
Ionizing radiation Mechanism:
- It causes DNA damage by one of the following mechanism
- Direct damage to cellular DNA
- Dislodges ions from water and other molecules of the cell and result in the formation of highly reactive free radicals that causes damage
Effects of Radiation:
- Chromosomal breakage
- Translocation
- Point mutation
Factors effecting it
- Type of radiation
- Dose
- Dose rate
- Frequency
- Host factors
- Age
- Individual susceptibility
- Immune competence
- Hormonal influences
- Type of cells irradiated
Question 5. Define carcinogenesis. Discuss in detail the chemical carcinogenesis.
Answer:
Definition
- Carcinogenesis means the mechanism of induction of tumours
- Agents that induce tumours are called carcinogens
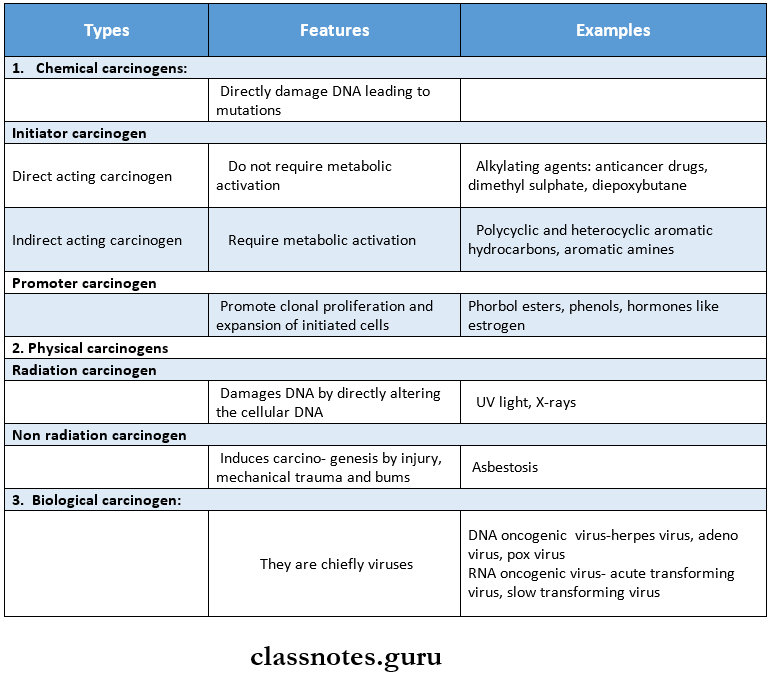
Chemical carcinogenesis:
- Chemical carcinogens have highly reactive electrophile groups that directly damage DNA leading to mutations and eventually cancer.
- Depending upon the mode of action, they are classified as:
- Initiator carcinogens.
- Promoter carcinogens
1. Initiator carcinogens: They can initiate the process of neoplastic transformation.
- Direct-acting carcinogens: They do not require metabolic activation.
- Alkylating agents: Anticancer drugs (Cyclophosphamide, busulfan, melphalan, nitrosourea),
- β-propionolactone and episodes.
- Indirect-acting agents (Procarcinogens): They require metabolic activation.
- Polycyclic and heterocyclic aromatic hydrocarbons: Benzathracenes, benzopyrene.
- Aromaticamaines, amides and azo dyesmaphthylamine ([3-naphthylamine), Ben-zidine and azo dyes like 2 – acctylaminofluorene, dimethyl amino azo benzene (butter yellow)
- Naturally occurring products: Chemical derived from plants and microbial sources i.e., aflatoxin Bl,
- Others: Nitrosamines/Nitrosamides in gastric carcinoma, insecticides, fungicides etc.
2. Promoter carcinogens:
- It promotes further clonal proliferation and expression of initiated cells
- Examples Phorbol esters, phenols, hormones like estrogen
Question 6. Define neoplasia. Classify oncogenic viruses and explain the role of viruses in carcinogenesis.
Answer:
Neoplasia Definition:
Neoplasia is defined as a mass of tissue formed as a result of abnormal, excessive, uncoordinated, autono¬mous and purposeless proliferation of cells even after cessation of stimulus for growth which causes it
Oncogenic Viruses:
- They are associated with neoplasms
- Based on nucleic acid content, oncogenic viruses are divided into 2 groups:
- DNA viruses
- RNA viruses
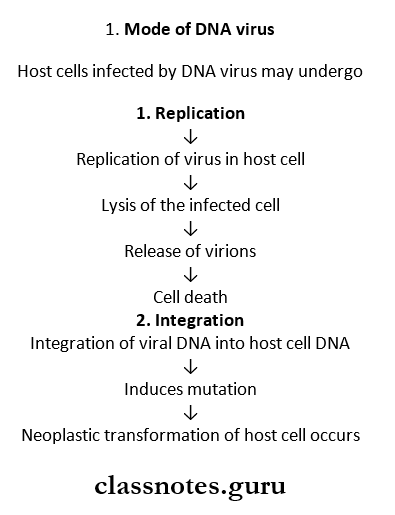
Role Of Virus In Carcinogenesis:
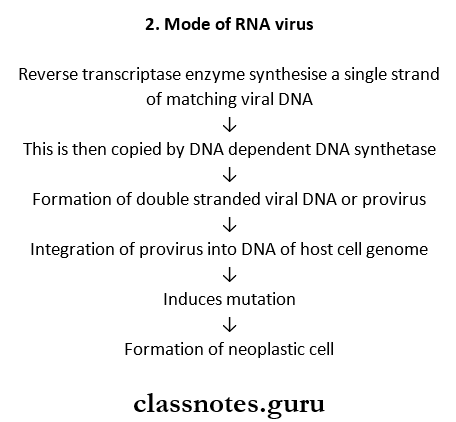
Neoplasia Short Essays
Question 1. Characteristics of malignancy
Answer:
1. Rate of growth:
- Malignant tumour cells have increased mitotic rates and slower death rates i.e., cancer cells do not follow normal control in the cell cycle and are immortal.
- Also, the rate of growth is directly proportional to the degree of differentiation.
2. Clinical and gross features:
- Clinically, malignant tumours grow rapidly, ulcerate on the surface, invade locally into deep tissues, may spread to distant sites, produce weight loss, anorexia and anaemia.
- Grossly, irregular in shape, poorly circumscribed and extending into adjacent tissues secondary changes like haemorrhage, infarction and ulceration are seen more often.
3. Microscopic features:
- Malignant tumours have a poor resemblance to origin.
- Basal polarity is lost
- Pleomorphism is present hyperchromatism and abnormal mitotic figures are seen.
- The nucleocytoplasmic ratio is increased anisonucleo- sis is generally present
- Tumour giant cells are present with nuclear atypia.
- The function may be retained/lost/abnormal.
4. Local invasion:
- Tumours invade via routes of least resistance eventually most cancers recognize no anatomic boundaries.
- Cancers extend through tissue space, permeate lymphatics, blood vessels, and perineural spaces and may penetrate the bone by going through nutrient foramina.
5. Metastasis/Distance spread:
- Lymphatic spread – In general carcinomas metastasize by the lymphatic route.
- Hematogenous spread – Common route for sarcomas.
- Spread along body cavities and natural passages – Routes are trans coelom, epithelial lined surfaces, CSF, and implantation.
Question 3. Staging of tumours
Answer:
- Staging of cancer is determined by surgical exploration or imaging and is based on the size, local and regional lymph node spread and distant metastasis.
- Staging is a system to determine the prognosis and choice of treatment of malignant cancer.
- Important systems of staging which currently in use are as follows:
- TNM system (T-primary tumour, N-regional lymph node involvement, M-metastases]
- ATC (American Joint Committee) System.
- Both systems take into account the following criteria;
- Size of the primary tumour
- Nodal involvement
- Metastasis
TNM Staging: For each of the 3 components T, N and M, numbers are added to indicate the extent of involvement as under:
- T0 to T4: In sites to the largest and most expensive primary tumour
- N0 to N3: NO nodal involvement to widespread lymph node involvement.
- M0 to M2: NO metastasis to disseminated haematoge- nous metastasis.
AJC system: Cancers are divided into stages 0 to 4 and take into account all the 3 components i.e., size, nodal spread and distant metastasis.
Neoplasia Short Question And Answers
Question 1. Oncogenes
Answer:
- Mutant versions of proto-oncogenes that function autonomously without a requirement for normal growth-promoting signals are known as oncogenes.
- A normal gene/proto-oncogene is converted / acti¬vated to an oncogene by.
- Change in the structure of the gene
- Change in regulations of gene expression.
- Oncogenes are activated by.
- Point mutation and deletion
- Chromosomal translocation
- Gene amplification.
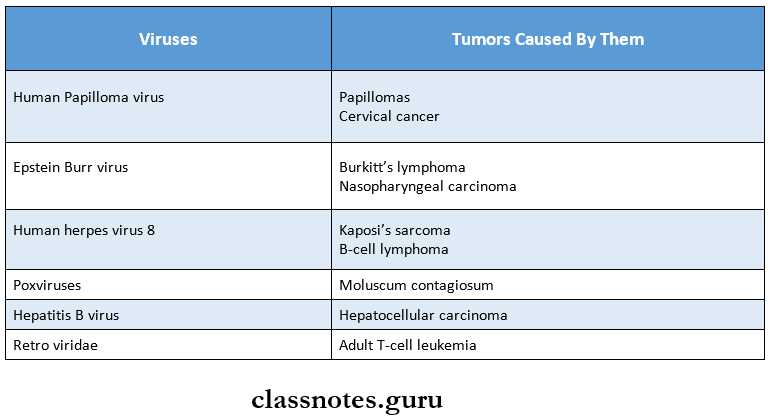
Question 2. Oncogenic viruses
(or)
Virus-related human tumours and examples.
Answer:
- Oncogenic viruses are associated with neoplasms.
- Based on nucleic acid content, oncogenic viruses are divided into 2 groups.
- DNA viruses
- KNA viruses.
DNA oncogenic viruses: DNA oncogenic viruses have direct access to the host cell nucleus and are incorporated to the genome of the host cell DNA.
Classified into 5 groups.
- Pap ova virus: Responsible for skin warts (squamous cell papillomae and invasive cervical cancer.
- Herpes virus: Epstein- ban virus (EBV] Burkitt’s lymphoma and human herpes virus 8 kaposi’s sar¬coma.
- Adenovirus: Causes respiratory tract infections and pharyngitis
- Poxvines: They cause moluscum contagiosum
- Hepadna virus: Hepatitis B virus.
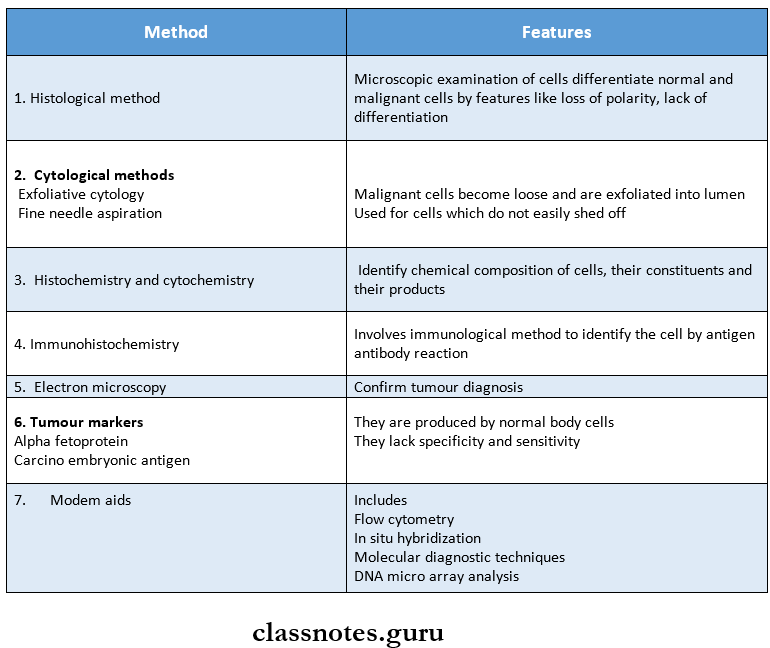
Question 3. Lab diagnosis of cancer
Answer:
Question 4. Burkitt’s lymphoma
Answer:
- It is a distinctive type of B-cell lymphoma caused by Epstein-Barr virus [EBV] infection.
- 3 sub-groups of Burkitt’s lymphoma are:
- African endemic
- Sporadic
- Immunodeficiency associated.
Burkitt’s lymphoma Etiology – EBV infection and immune suppression.
Burkitt’s Lymphoma Features:
- The disease affects children and adolescents
- Involves extranodal sites, particularly the jaw, gas- tro intestinal tract and gonads.
Histological appearances: Tightly packed lymphoblasts interspersed with phagocytic macrophages which impart a starry-sky appearance in histological sections.
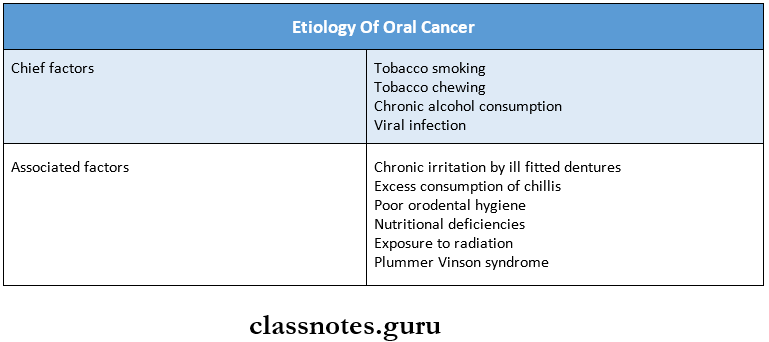
Question 5. Etiology of oral cancer
Answer:
Question 6. Ionizing radiation
Answer: Ionizing radiation like X-rays, alpha, beta and gamma rays can cause cancer
Ionizing radiation Mechanism:
- It causes DNA damage by one of the following mechanism
- Direct damage to cellular DNA
- Dislodges ions from water and other molecules of the cell and result in the formation of highly reactive free radicals that causes damage
Effects of Radiation:
- Chromosomal breakage
- Translocation
- Point mutation
Question 7. Tumour markers
Answer:
- Tumour markers are biochemical assays of products elaborated by the tumour cells in blood/other body flu¬ids.
- These methods clack sensitivity as well as specificity and can be used.
- As an adjacent to pathologic diagnosis arrived at by other methods and not for primary diagnosis of can¬cer.
- Can be used as prognostic and therapeutic purposes
- Tumour markers include:
- Oncofetal antigens
- Alpha foetoprotein
- Carcinoembryonic antigen.
- Enzymes
- Prostrate acid phosphatase
- Lactic dehydrogenase
- Hormones
- Human chronic gonadotropin
- Calcitonin
- Ectopic hormone production
- Cancer-associated proteins.
- Oncofetal antigens