
Joints Of Lower Limb Question And Answers
Question 1. Explain in detail about hip joint under the headings—type, articular surfaces, ligaments, factors providing stability to the joint, relations, bursae around the joint, blood supply, nerve supply, movements, and muscles involved.
Answer:
Hip Joint
- It is homologous with the shoulder joint of upper limb.
- But it is more stable at the cost of mobility compared to shoulder joint which is more mobile at the cost of stability.
Hip Joint Type
- Ball and socket type of synovial joint.
- It is simple and multiaxial joint.
Hip Joint Articular Surfaces
- Head of the femur articulates with the acetabulum of the hip bone.
- Head of femur is covered with hyaline cartilage except at the fovea capitis.
- Acetabulum have a horse shoe-shaped lunate articular surface with an acetabular notch and an acetabular fossa.
- The articular surface of the acetabulum is also covered with cartilage.
Read And Learn More: Anatomy Question And Answers
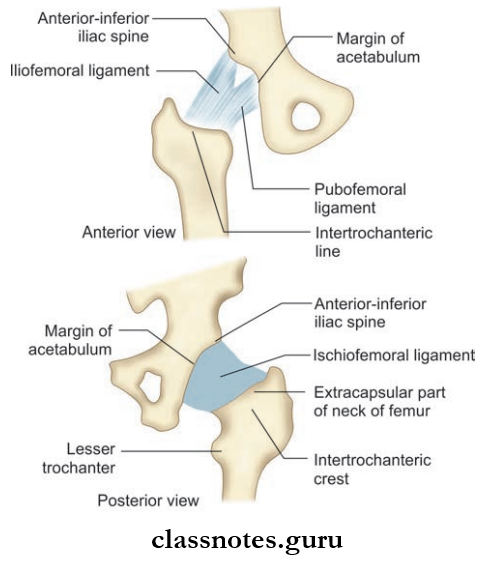
Hip Joint Ligaments
- Capsular Ligament
- Unlike in the shoulder joint, joint capsule is strong and dense limiting the wide range of movements.
- Attachments:
- Medially on the hip bone, on the outer aspect of the acetabular labrum, and transverse acetabular ligament.
- Laterally on the femur, anteriorly to the intertrochanteric line, and posteriorly about 1 cm in front of the intertrochanteric crest.
- The joint capsule is thick and strong anterosuperior where maximum stress occurs especially when standing and running.
- It is thin and loose posteroinferiorly through which dislocation of hip joint occurs commonly.
- The capsule is made up of two layers of fibers. The inner circular and outer longitudinal fibers.
- Joint capsule is lined inside by a synovial membrane.
- The joint capsule is thick and strong anterosuperior where maximum stress occurs especially when standing and running.
- Iliofemoral Ligament/Ligament of Bigelow
- It is an inverted yshaped ligament located anterior aspect of the joint and it is blended with the joint capsule.
- Its apex is attached to the lower half of the anterior inferior iliac spine and the base to the intertrochanteric line.
- It is one of the strongest ligaments of the body preventing falling body backwards in a standing posture
- Pubofemoral Ligament
- It is a triangular-shaped ligament located anteromedially to the joint.
- Its base is directed upwards and attached to the iliopubic eminence, superior pubic ramus, and obturator crest.
- Its apex is directed downwards and blends with the anteroinferior part of the capsule and medial band of iliofemoral ligament.
- Ischiofemoral Ligament
- It is a relatively weak ligament located posteriorly.
- It is attached superiorly to the ischium and inferiorly to the greater trochanter deep to the iliofemoral ligament.
- Ligament of Head of Femur/Round Ligament/ligament
- Terms of Head of Femur
- It is a flt triangular ligament.
- Its apex is attached to the fovea of head of femur and the base to the transverse acetabular ligament.
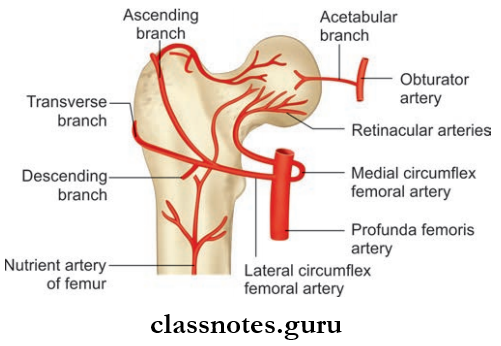
- It transmits arterial branches from the obturator and medial circumflex femoral arteries to the head of femur.
- Acetabular Labrum
- It is a fibrocartilaginous rim attached to the acetabular margin.
- It deepens the acetabulum and grasps the head of femur in its position.
- Transverse Acetabular Ligament
- It bridges the acetabular notch making it into the acetabular foramen.
- The acetabular foramen transmits the vessels and nerves to the hip joint.
- Terms of Head of Femur
Hip Joint Factors Providing Stability To The Hip Joint
- Acetabulum is deep and the depth is increased by the presence of acetabular labrum
- Strong ligaments.
- Strength of the surrounding muscles.
- Length and obliquity of the neck of femur.
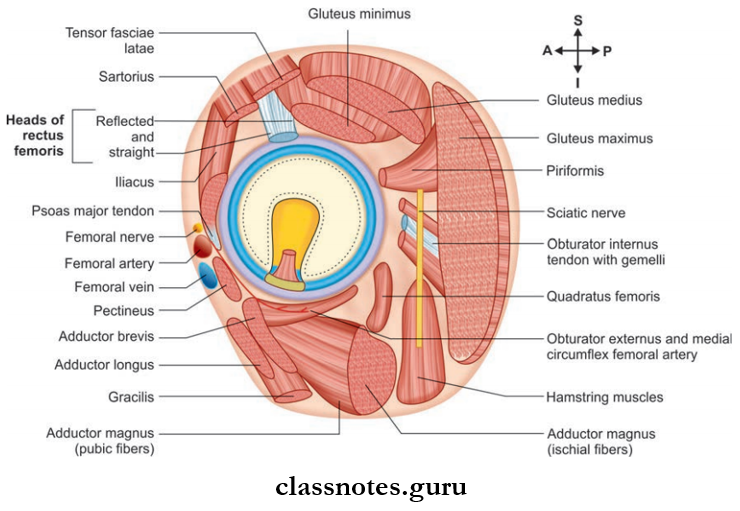
Hip Joint Relations
- Anteriorly: Tendon of iliopsoas separated from the joint capsule by the bursa, femoral vessels, and nerve.
- Posteriorly: From below upwards:
- Tendon of obturator externus covered by Quadratus femoris
- Obturator internus and gemelli
- Piriformis
- Sciatic nerve
- Gluteus maximus
- Superiorly: Reflcted head of rectus femoris covered by gluteus minimus, gluteus medius and gluteus maximus.
- Inferiorly: Lateral fiers of pectineus and obturator externus, gracilis, adductor longus, brevis, Magnus, and hamstring muscles.
Bursae Around Hip Joint
- Subgluteal bursa
- Subpsoas bursa.
Hip Joint Arterial Supply
- Medial circumflex femoral artery
- Lateral circumflex femoral artery
- Obturator artery
- Superior gluteal artery
- Inferior gluteal artery.
Hip Joint Nerve Supply
- Femoral nerve via nerve to rectus femoris
- The anterior division of obturator nerve
- Nerve to quadratus femoris
- Superior gluteal nerve.
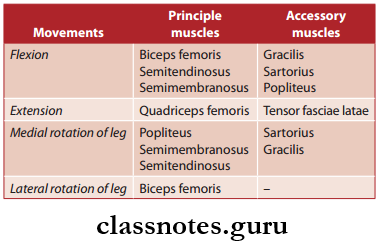
Movements And Muscles Involved
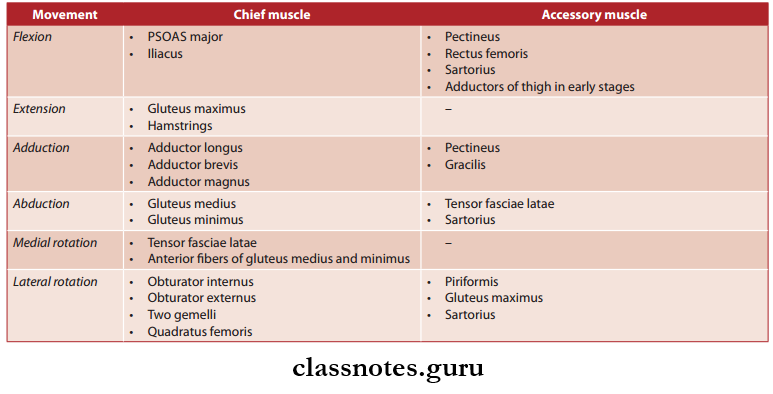
Mnemonics
- Hip: Lateral rotators “Play Golf Or Go On Quaaludes”:
- From top to bottom:
- Piriformis
- Gemellus superior
- Obturator internus
- Gemellus inferior
- Obturator externus
- Quadratus femoris
Hip Joint Clinical Anatomy
- Dislocation Of Hip Joint
- Hip joint can dislocate congenitally or accidentally.
- Congenital dislocation of the hip joint should be identified soon after birth and treated.
- Accidental dislocation of the hip occurs most commonly posteriorly because the joint capsule and ligaments on the posterior aspect of the joint is weak.
- This type of dislocation can injure the sciatic nerve.
- Anterior dislocations of the hip joint are very rare because the joint capsule and the ligaments of the anterior aspect of the joint are very strong.
- Fracture Of Neck Of Femur
- Fractures of the neck or femur can occur in individuals, especially females after the age of 60 due to osteoporosis. The limb is shortened and laterally rotated because of the pull of the muscles of the back. It leads to avascular necrosis of the neck of the femur.
- A time gap is given for the fracture segment to unite if it is young individuals. Hip replacement surgeries are preferred in elderly patients.
- Shenton’s line is a continuous curve formed by the upper border of the obturator foramen and lower margin of the neck of the femur seen in a normal Xray pelvis. But following posterior dislocation and fracture of the neck of the femur, this line is disrupted.
- Shoemaker’s line is a line extending from the greater trochanter, advancing through the anterior superior iliac spine, to pass through the umbilicus. But in fracture of neck of the femur or in posterior dislocations, this line passes below the umbilicus.
Question 2. Explain in detail about the knee joint under the headings—type, articular surfaces, ligaments, bursae around the joint, blood supply, nerve supply, movements and muscles involved, and locking and unlocking of the knee joint.
Answer:
Knee Joint
The Knee Joint is the largest joint in the body. It is also more complex than other joints due to the presence of three articulations.
Knee Joint Type
- Knee Joint is a modified hinge type of synovial joint.
- Knee Joint is a compound joint. It incorporates two condylar joints between the condyles of femur and tibia and one saddle joint between the femur and patella.
Knee Joint Ligaments
- Fibrous articular capsule
- Knee Joint is very thin and deficient anteriorly where it is replaced by quadriceps femoris, patella and ligamentum patellae.
Knee Joint Articular Surfaces
- The lateral and medial condyles of the femur articulate with the lateral and medial condyles of the tibia respectively. It is of condylar type.
- The patella articulates with the femur. It is of saddle type.
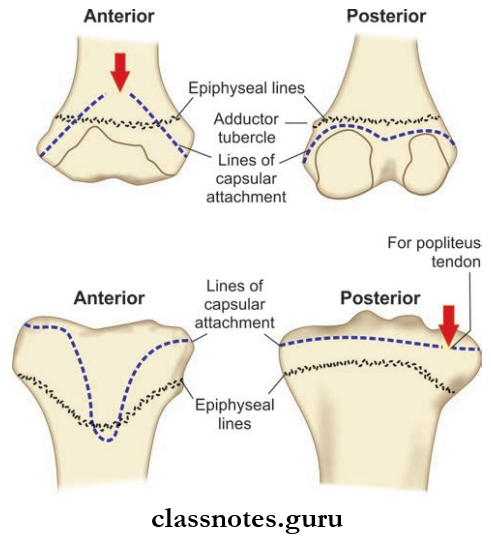
- Attached on
- Femur
- ½ to 1 cm beyond the articular margins except:
- Anteriorly where it is replaced by the suprapatellar bursa in the middle
- Posteriorly where it is attached to the intercondylar line
- Laterally where it encloses the origin of the popliteus muscle.
- ½ to 1 cm beyond the articular margins except:
- Tibia
- ½ to 1 cm beyond the articular margins except:
- Posteriorly where it encloses the tendon of the popliteus muscle.
- It is lined inside by a synovial membrane.
- ½ to 1 cm beyond the articular margins except:
- Femur
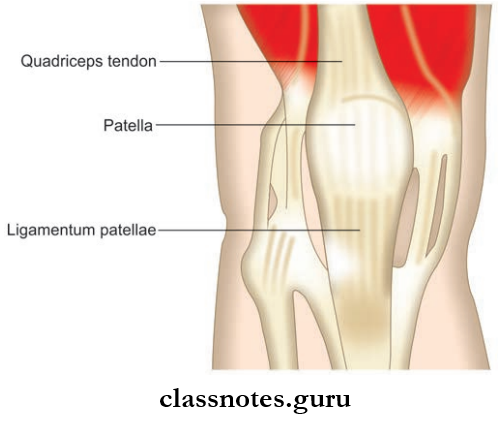
Knee Joint Ligamentum Patellae
- Knee Joint Ligamentum is the central part of the common tendon of insertion of quadriceps femoris (the remaining portion of tendon forms lateral and medial patellar retinacula)
- Knee Joint Ligamentum is 7.5 cm in length and 2.5 cm in width.
- Superiorly, it is attached to the apex of the patella and inferiorly to smooth upper part of the tibial tuberosity.
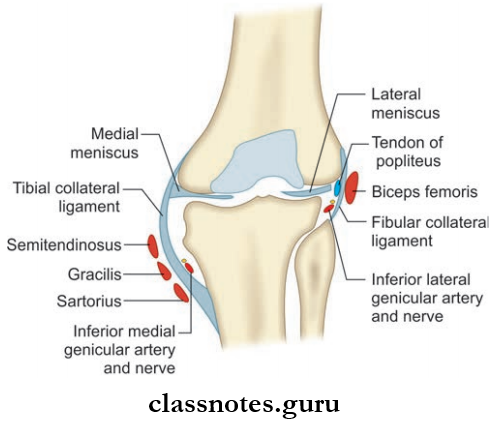
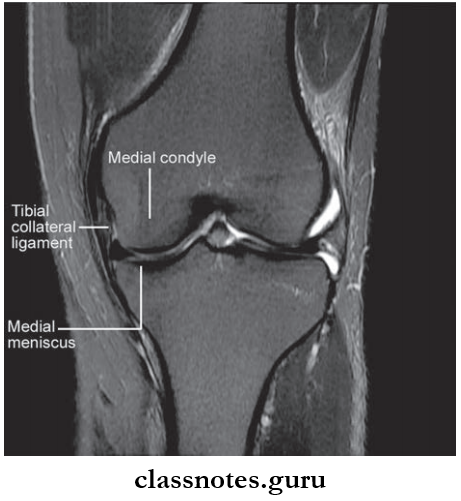
Tibial Collateral Ligament/Medial Ligament
- Tibial Collateral Ligament is a long and strong fibrous band located at the medial side of the knee joint.
- Tibial Collateral Ligament has two parts—superficial and deep.
- The superficial part is longer, attached above to the medial epicondyle of femur just below the adductor tubercle and below to the medial border and posterior part of the medial surface of the shaft of the tibia.
- The Tibial Collateral Ligament covers the inferior medial genicular nerves and vessels, and the anterior part of the tendon of the semimembranosus.
- The Tibial Collateral Ligament is crossed superficially by the tendon of the sartorius, gracilis, and semitendinosus.
- The deep part is shorter, attached above the medial epicondyle of the femur just below the adductor tubercle and below to the medial condyle of tibia above the groove for the tendon of the semimembranosus.
- The Tibial Collateral Ligament blends with the fibrous capsule and peripheral margin of the medial meniscus in the middle.
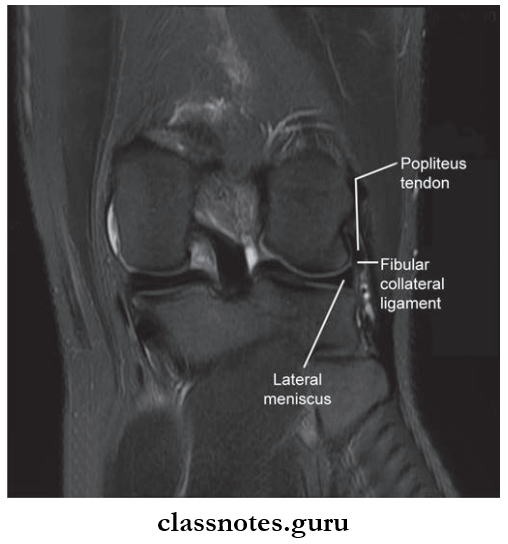
Fibular Collateral Ligament/Lateral Ligament
- The fibular Collateral Ligament is a short, strong, and cord-like ligament located on the lateral side of the knee joint.
- The fibular Collateral Ligament is attached to the lateral epicondyle of the femur just above the popliteal groove and below, it is attached to the head of the fibula in front of its apex.
- In the lower part, the ligament is crossed by the tendon of the biceps femoris.
- Unlike the medial ligament, the lateral ligament does not blend with the lateral meniscus due to the presence of the tendon of the popliteus.
- The fibular Collateral Ligament is also free from the capsule separated by inferior lateral genicular nerves and vessels.
Oblique Popliteal Ligament
- The Oblique Popliteal Ligament is an expansion from the tendon of the semimembranosus muscle located posteriorly.
- The Oblique Popliteal Ligament runs upwards and laterally blends with the capsule of the knee joint.
- The Oblique Popliteal Ligament is attached to an intercondylar line of the femur.
- The Oblique Popliteal Ligament strengthens the capsule posteriorly and is in close relation with the knee joint.
- The Oblique Popliteal Ligament is pierced by middle genicular vessels and nerves, the posterior division of the obturator nerve.
Arcuate Popliteal Ligament
- It is a posterior expansion from the short part of the fibular collateral ligament.
- Anterior and Posterior Cruciate Ligaments
- They are two thick and strong intracapsular fibrous bands crossing each other like ‘X’, hence the name
cruciate. - They are named anterior and posterior according to their site of attachment in the tibia.
- They are considered to be the direct bonds of union between the tibia and femur.
- They maintain anteroposterior stability of the knee joint.
- They are two thick and strong intracapsular fibrous bands crossing each other like ‘X’, hence the name
- Anterior and Posterior Cruciate Ligaments
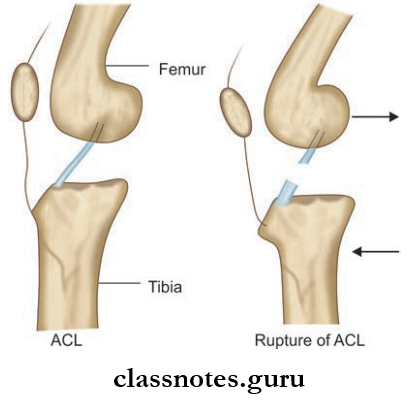
An Anterior Cruciate Ligament (ACL)
- ACL is attached below to the anterior part of the intercondylar area of the tibia and runs upwards, backward, and laterally to get attached on the posterior part of the medial surface of the lateral condyle of femur.
- ACL prevents the anterior displacement of tibia.
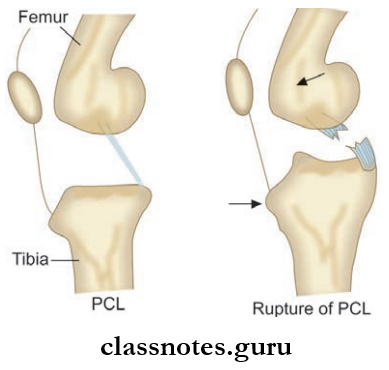
Posterior Cruciate Ligament (PCL)
- PCL is attached below the posterior part of the intercondylar area of tibia and runs upward forward and medially to the anterior part of the lateral surface of the medial condyle of femur.
- PCL prevents the posterior displacement of tibia.
Menisci/Semilunar Cartilages Of Knee Joint
- They are crescent or semilunar-shaped intraarticular discs made up of fibrocartilage.
- They divide the joint cavity into two. The upper compartment (meniscofemoral) and the lower compartment (meniscotibial).
- Each meniscus has:
- Two ends: Anterior and posterior attached to the tibia
- Two borders: Thck, convex, fixed outer border and thin, concave, free inner border
- Two surfaces: Concave upper surface for the articulation with the femur. The flat lower surface which rests on the peripheral 2/3rd of the tibial condyle
- The peripheral part is vascular and the inner part is avascular nourished by the synovial fluid.
Medial Meniscus
- Almost semicircular.
- Has anterior and posterior horns and both are attached to the intercondylar area of the tibia.
- It is attached to the deep part of the tibial collateral ligament.
Lateral Meniscus
- Almost circular.
- It also has anterior and posterior horns and both are attached to the intercondylar area of the tibia.
- The posterior horn of the lateral meniscus is attached to the medial condyle of the femur by anterior and posterior meniscofemoral ligaments.
- The medial part of the tendon of the popliteus muscle is attached to the lateral meniscus.
- This, the movements of the lateral meniscus is controlled by the popliteus muscle and anterior and posterior meniscofemoral ligaments.
Mnemonics
Menisci attachments in the knee ‘Each meniscus has something attached to it:
- The medial meniscus has the medial collateral ligament.
- The lateral meniscus is attached to the popliteal muscle.
Functions of Menisci
- Menisci increase the concavity of the condylar surface of the tibia ensuring the best congruence with the condylar surface of the femur.
- They act as shock absorbers.
- They help to lubricate the joint cavity.
- Flexion and extension of the knee joint take place in the upper compartment made by the menisci where as medial and lateral rotation take places in the lower compartment.
- Since they are innervated by sensory nerves, they have a proprioceptive role too.
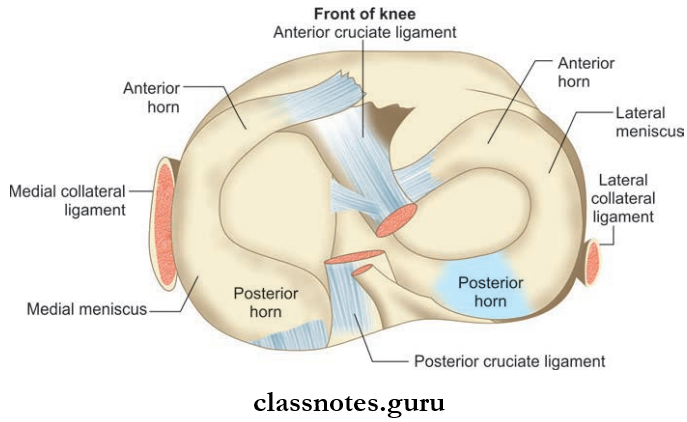
Transverse Ligament:
- It connects the anterior end of the lateral and medial menisci.
- Bursae Around Knee Joint
- Around 13 bursae are found around the knee.
- Anteriorly
- Subcutaneous prepatellar bursa
- Subcutaneous infrapatellar bursa
- Deep infrapatellar bursa
- Suprapatellar bursa.
- Laterally
- Bursa deep to the lateral head of the gastrocnemius
- Bursa in between the fibular collateral ligament and biceps femoris
- Bursa in between the fibular collateral ligament and tendon of popliteus
- Bursa in between tendon of popliteus and lateral condyle of tibia.
- Medially
- Bursa deep to the medial head of gastrocnemius
- Anserine bursa
- Bursa deep to the tibial collateral ligament
- Bursa deep to the semimembranosus.
- Bursae Around Knee Joint
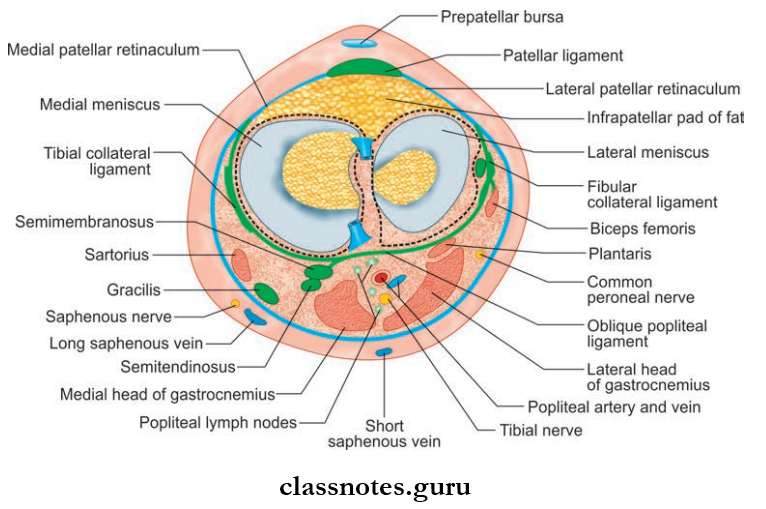
Relations of Knee Joint
- Anteriorly
- Anterior bursae
- Ligamentum patellae
- Patellar plexus of nerves
- Posteriorly
- At the middle
- Popliteal vessels
- Tibial nerve
- Posterolaterally
- The lateral head of the gastrocnemius
- Plantaris
- Common peroneal nerve
- Posteromedially
- The medial head of the gastrocnemius
- Semitendinosus
- Semimembranosus
- Gracilis
- Popliteus at its insertion
- At the middle
- Medially
- Sartorius
- Gracilis
- Semitendinosus
- Great saphenous vein
- Saphenous nerve
- Semimembranosus
- Laterally
- Biceps femoris
- Tendon of origin of popliteus
Relations of Knee Joint Blood Supply
- Five genicular branches of the popliteal artery
- Descending genicular branch of femoral artery
- Descending branch of lateral circumflex femoral artery
- Two recurrent branches of the anterior tibial artery
- Circumflex fibular branch of the posterior tibial artery.
Relations of Knee Joint Nerve Supply
- Sciatic nerve through its genicular branches of tibial and common peroneal nerve
- Femoral nerve
- Obturator nerve through its posterior division.
Movements And Muscles Involved
- Locking and Unlocking of the Knee Joint
- The locking mechanism helps the knee to remain in a standing position without much muscular effort.
- This is possible due to the fact that the anteroposterior diameter of the medial condyle of the femur is larger than that of the lateral condyle.
- As a result, towards the end of extension movement, the lateral condyle of the femur is fully occupied whereas a portion of the medial condyle is still unused by the tibia.
- So the lateral condyle acts as an axis around which the femur rotates medially on the tibia to engage the medial condyle completely.
- This is done by the extensors of the knee joint, especially vastus medialis.
- Now the knee joint is locked and the muscles around the joint can relax at the expense of taut ligaments.
- This mechanism is a blessing when one stands.
- Unlocking is done by the popliteus muscle by laterally rotating the femur on the tibia.
- Now the flexors can act and flex the knee joint.
- Clinical Anatomy
- The knee joint is:
- Largest joint in the body
- Compound joint
- Weight-bearing joint.
- The knee joint is:
- Due to these specialties, it is more prone to injuries and damages.
- Injury to the anterior cruciate ligament causes anterior dislocation of the tibia and the anterior drawers sign will be positive. Injury to the posterior cruciate ligament causes posterior dislocation of the tibia, and the posterior drawers sign will be positive.
- The medial meniscus is more prone to injury than the lateral meniscus. this is due to the fact that the medial meniscus is fied to the capsule and tibial collateral ligament whereas the lateral meniscus is protected by the pull of the popliteus muscle with which it is attached.
- As age advances, the knee joint is more prone to osteoarthritis.
- If fluid is collected in the joint cavity, the patellar tap shows a floating patella, and fluid is aspirated from either side of the ligamentum patellae.
Question 3. Write a short note on the deltoid ligament.
Answer:
Deltoid Ligament
- The Deltoid Ligament is a very strong triangular ligament seen on the medial side of the ankle joint
- Deltoid Ligament has superficial and deep parts.
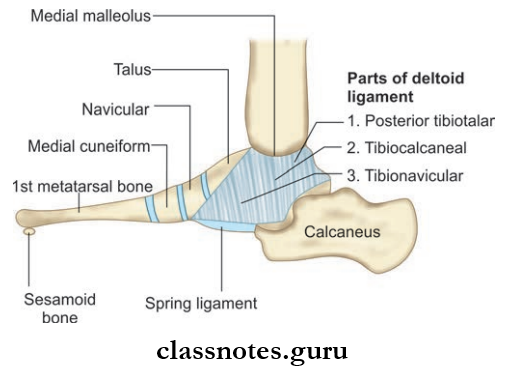
The Deltoid Ligament Superficial Part
- It has 3 sets of filters and all of them have a common superior attachment to the apex and margins of medial malleolus.
- But they have different attachments in the inferior part.
- Anterior fibers or talonavicular fiers are attached inferiorly to the tuberosity of the navicular bone and to the medial margin of the spring ligament.
- Middle fibers or talocalcaneal fiers are attached inferiorly to the whole length of sustentaculum tali.
- Posterior fibers or posterior tibiotalar fibers are attached to the medial tubercle and to the adjoining part of the medial surface of the talus.
The Deltoid Ligament Deep Part
- It has the same superior attachment as that of the superficial part.
- Inferiorly it is attached to the anterior part of the medial surface of the talus.
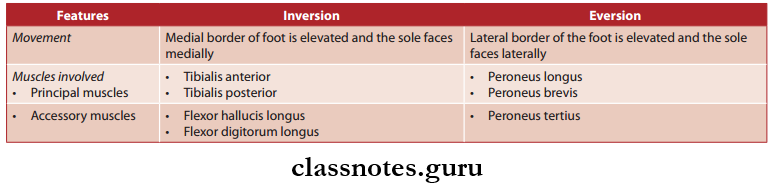
Question 4. Explain about inversion and eversion of the foot by comparing them.
Answer:
Inversion And Eversion Of The Foot By Comparing Them
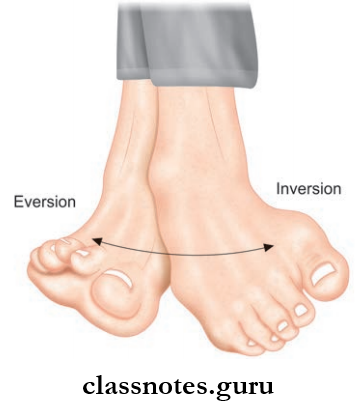
Inversion And Eversion Of The Foot Joints Taking Part
- Subtalar joint
- Talocalcaneonavicular joint
- Transverse tarsal/midtarsal joint.
Inversion And Eversion Of The Foot Axis of Movement
- Around the oblique axis
Inversion And Eversion Of The Foot Functional Significance
- Helps to walk in uneven and sloppy ground.
- When the foot is in the ground, this movement occurs in its modified form called supination and pronation.
Mnemonic
Inversion vs Eversion Muscles in Leg
- Second letter rule for inversion/eversion:
- Eversion muscles:
- pEroneus longus
- pEroneus brevis
- pEroneus tertius
- Inversion muscles:
- tIbialis anterior
- tIbialis posterior.
- Eversion muscles:
Joints Of Lower Limb Multiple Choice Questions
Question 1. The number of ossification centers in the lower limb (on one side) in full term newborns are_____:
- Six
- Five
- Two
- One
Answer: 2. Five
Question 2. In Clergyman’s knee, which bursa is affected?
- Prepatellar
- Suprapatellar
- Subcutaneous infrapatellar
- Semimembranosus
Answer: 3. Subcutaneous infrapatellar
Question 3. What is the deformity if patient walks on the toes?
- Talipes varus
- Talipes valgus
- Talipes equinus
- Talipes calcaneus
Answer: 3. Talipes equinus
Question 4. Which of the following is maximally taut while walking downhill?
- Medial collateral ligament
- Posterior cruciate ligament
- Lateral collateral ligament
- Anterior cruciate ligament
Answer: 2. Posterior cruciate ligament
Question 5. What is true about lateral meniscus?
- Attached to fibular collateral ligament
- Attached to popliteus
- Bucket hand tear is common
- Semicircular in shape
Answer: 2. Attached to the popliteus