
Dental Caries
Question 1. Zinc polycarboxylate cement.
Answer:
Zinc polycarboxylate cement Composition:
1. Powder:
- Zinc oxide Basic ingredient
- Magnesium oxide
- Modifier
- Aids in sintering
- Bismuth and aluminum oxide occur in small amounts
- Stannous fluoride
- Increase strength
- Modifies setting time
- Imparts anti-cariogenic properties
2. Liquid:
- Polyacrylic acid
- The copolymer of acrylic acid with other unsaturated carboxylic acids
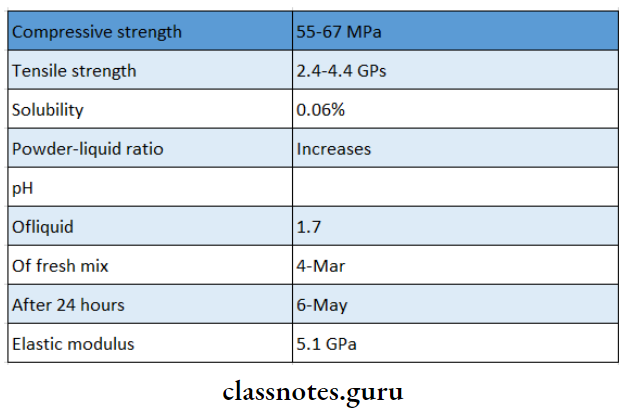
Zinc Polycarboxylate Cement Properties:
1. Physical Properties:
2. Biocompatibility:
- Mild pulpal response
3. Adhesion:
- Excellent adhesion
- Polyacrylic acid reacts with calcium ions via car¬boxyl groups on the surface of enamel and dentin
- The bond strength of enamel is greater
4. Optical Properties:
- Optical Properties are very opaque
5. Thermal Properties:
- Thermal Properties is a thermal insulator
Zinc Polycarboxylate Cement Uses:
- Cementation of restoration
- As bases and liners
- As intermediate restoration
- Luting of permanent restoration
- In orthodontics cementation of bands
- In endodontics as root canal filling material
Question 2. Define and classify caries. Add a note on the diagnosis of caries.
Answer:
Caries Definition:
- Dental caries is defined as a multifactorial, transmissible, infectious oral disease caused primarily by the complex interaction of cariogenic oral flora with fermentable dietary carbohydrates on the tooth surface over time
Caries Classification:
1. According To Location
- Primary Caries
- Pit and fissure caries
- Smooth surface caries
- Root caries
- Secondary Caries
2. According To The Direction
- Forward caries
- Backward caries
3. According To The Extent
- Incipient caries
- Cavitated caries
4. According to Rate
- Acute caries
- Chronic caries
5. According To A Histological Depth Of Penetration
- Enamel caries
- Dentinal caries
Diagnosis Of Caries
1. Visual Tactile Examination:
- Visual Method:
- Cavitation
- Opacification
- Discoloration
- Surface roughness
- Tactile Method:
- Softness of enamel
- Catch obtained by an explorer
- Illumination:
- UV light creates decreased fluorescent in carious lesions as compared to healthy tissue
- Cavitation produces echoes of higher amplitude
2. Caries Detecting Dyes:
- Dyes For Enamel Caries:
- Procion Staining is irreversible
- Reacts with nitrogen and hydroxyl groups
- Calcein Bounds with calcium
- Zyglo ZL22 Visible by UV illumination
- Dyes For Dentin Caries:
- Infected and affected dentin layers are present
- Basic Fuschia in propylene glycol stains only the infected dentin
- Radiographic Methods:
- Requires 50% tooth destruction
- Seen as a radiolucent lesion
Caries Types
1. Caries Conventional:
- IOPA
- Bitewing For proximal caries
- Occlusal
- Xeroradiography
- Edge enhancement
2. Caries Advanced:
- Digital radiography
- Subtraction radiography
- RVG
3. Caries Electrical Conductance:
- Electrical conductivity is directly proportional to the amount of demineralization
4. Lasers:
Question 3. Methods of Diagnosis of Proximal Caries.
Answer:
1. Bitewing Radiograph:
- It includes occlusal surfaces of both arches in the same radiograph
- It must be differentiated from cervical bum out
- It describes the extent of the carious lesion
- 0 Normal
- 1 – Only enamel is involved
- 2- Caries extends upto DEJ/Dentinoenamel junction
- 3 – Caries involve the whole of the enamel and the outer half of the dentin
- 4 – Caries involve complete enamel and dentin
2. – Separation Of Teeth:
- With the help of separators, teeth are moved apart and viewed for carious lesions
3. Dental Floss:
- Dental floss is used through the proximal surface
- Fraying of it indicates the presence of a lesion
4. Transillumination:
- It is based on the refractory index between the carious and sound tooth
- Carious tooth appears as a dark shadow when compared to normal tooth
Question 4. Pit and fissure Caries.
Answer:
- The shape of pit and fissure make it more susceptible to caries
Pit And Fissure Caries Features:
- Initial Brown/Black in color
- Catch with an explorer
- DecalciFication of enamel
- Enamel involvement in the direction of the rod
- Shape Triangular, base towards DE
- Progress to the involvement of dentinal tubules
- Result in cavitation
- Undermining of enamel
Question 5. Root Caries/Cemental Caries.
Answer:
- Root Caries is a soft, progressive lesion that is found anywhere on the root surface that has lost its connective tissue attachment and is exposed to the environment
Root Caries Features:
- Periodontal attachment loss
- Soft, irregular lesion
- Round or oval in shape
- Irregular outline
- Common in males
- Common in mandibular molars
Root Caries Etiology:
- Streptococcus mutants
- Lactobacillus
- Actinobacillus
Root Caries Prevention:
- Plaque removal
- Diet modification
- Use of topical fluoride
- Soft tissue management
- Use of xylitol-containing chewing gum
Question 6. Roles of fluoride in caries prevention
Answer:
1. Increased Enamel Resistance/ Reduction In enamel Solubility
- Dental caries involves the dissolution of enamel by acid formation
- This dissolution is inhibited by fluoride as the fluoride forms fluorapatite which reduces enamel solubility
- Fluoride reduces enamel solubility also by promoting the precipitation of hydroxyapatite and phosphate mineral
- Fluoride inhibits demineralization by
- Reducing bacterial acid production
- Reducing equilibrium solubility of apatite
- By fluoridation of apatite crystal
2. Increased Rate Of Post-Eruptive Maturation
- Newly erupted teeth have hypomineralised areas and the enamel surface is also prone to dental caries
- Fluoride increases the rate of mineralization of these areas
- Organic material is also deposited over the enamel surface which increases its resistance to dental caries
3. Remineralization Of Incipient Lesions
- Fluoride enhances remineralization by the deposition of minerals into the damaged areas
- This reduces enamel solubility through the growth of crystals which are more resistant to acid
- Fluoride enhances remineralization from calcium phosphate solution by the formation of calcium fluoride which prevents hydroxyapatite crystal growth
4. Interference With Microorganisms
In Two Ways
- In High-Concentration Bacteriocidal
- By reducing plaque
- In low-concentration bacteriostatic
- Inhibits enzymes responsible for acid metabolism
5. Modification In Tooth Morphology
- If fluoride is ingested during tooth development it results in the formation of
- More caries-resistant tooth
- A tooth with smaller and shallow fissures
- Smaller diameter and cusp depth
- All these make them more self-cleansing
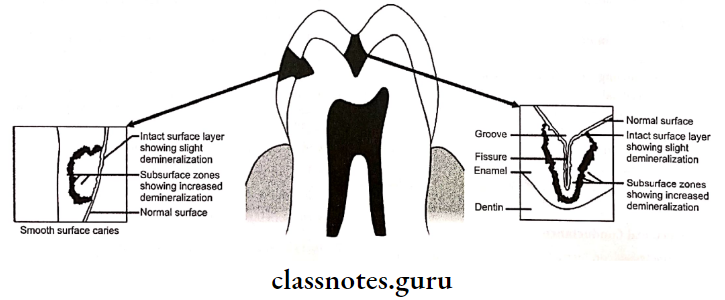
Question 7. Zones of enamel caries
Answer:
1. Zone 1 Translucent zone
- It is the deepest zone
- It is slightly more porous
- Contains 1% by volume
- Pores are larger than usual pores seen in normal enamel
- Dissolution of mineral occurs at the junction of prismatic and interprismatic enamel
2. Zone 2 Dark zone
- Located superficial to the translucent zone
- Excessive demineralization of enamel occurs
- It is narrow in rapidly advancing caries and wide in slowly advancing caries
- Contains 24% pore volume
- Pores are smaller than that of the translucent zone
- There is some degree of remineralization
3. Zone 3 Body Of The Lesion
- Present between dark zone and surface zone
- Represents the area of greatest demineralization
- Pore volume is between 525%
- Contains larger apatite crystals
- Reprecipitation of minerals occurs
- Dissolution of minerals occurs
- Lost minerals are replaced by unbound water and organic matters
4. Zone 4 Surface Zone
- Zone 4 Surface Zone remains unaffected
- Zone 4 Surface Zone is 40 pm thick
- Surface remineralization occurs due to the active precipitation of mineral ions
Question 8. Zones of dentinal caries.
Answer:
- Zone 1: Normal dentin
- Zone of fatty degeneration of odontoblast
- Represents thinner most layer of carious dentin
- No crystals are present in the lumen of tubules
- No bacteria present in tubules
- Intertubular dentin has normal collagen
Zone 2: Subtransparent dentin
- Zone of dentinal sclerosis characterized by deposition of calcium salts in dentinal tubules
- The superficial layer shows areas of demineralization and damage of odontoblastic processes
- Subtransparent dentin is capable of remineralization
- No bacteria is present in tubules
Zone 3: Transparent dentin
- Zone of decalcification of dentin, a narrow zone preceding bacterial invasion
- Transparent dentin is softer than normal dentin
- Large crystals are present within the lumen of dentinal tubules
- No bacteria is present in tubules
- Transparent dentin is capable of self-repair and remineralization
Zone 4: Turbid dentin
- Zone of bacteria] invasion of decalcified but intact dentin
- Widening and distortion of dentinal tubules
- Cannot undergo self-repair or remineralization
- Must be removed before restorative treatment
Zone 5: Infected dentin
- Zone of decomposed dentin
- Infected dentin is the outermost zone of carious dentin
- Characterized by complete destruction of dentinal tubules
- Areas of decomposition of dentin occur along the direction of dentinal tubules called liquefaction foci of Miller
- Transverse clefts are seen due to the decomposition of dentin
- Bacteria invade and destroy peri and intertubular dentin