
Anterior Abdominal Wall Question And Answers
Question 1. Describe about abdominal cavity and briefly mention its contents.
Answer:
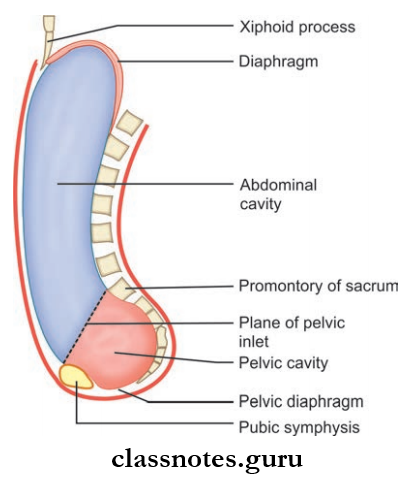
- Abdominal Cavity is the lower part of the trunk, below the diaphragm
- Walls surrounding the abdomen forms the abdominal cavity
- Boundaries Of The Abdominal Cavity
- Superiorly: Diaphragm
- Inferiorly: Pelvic diaphragm
- Anteriorly: Anterior abdominal wall (muscles)
- Posteriorly: Posterior abdominal wall (muscles and lumbar vertebrae)
- Both Sides: Lateral ends of muscles of anterior abdominal wall, lower ribs.
Anatomy Of Anterior Abdominal Wall
Read And Learn More: Abdomen And Pelvis
Abdominal Cavity Contents
- Liver and gallbladder
- Pancreas
- Stomach
- Small intestine and major portion of large intestine
- Kidneys and upper part of ureters
- Suprarenal glands
- Spleen
- Arteries, veins, lymphatics, nerves, etc.
Question 2. Describe about the various abdominal planes and mention the abdominal quadrants.
Answer:
The Various Abdominal Planes And Mention The Abdominal Quadrants
Transumbilical Plane
- A transverse plane passing through the umbilicus
- Lies between L3 and L4 vertebrae.
Median Vertical Plane
The Median Vertical Plane is a plane passing through the suprasternal notch and pubic symphysis.
The lateral Vertical Plane is a plane passing through, the midway between mid inguinal point and middle of the clavicle.
Anterior Abdominal Wall Layers
Transpyloric Plane of Addison
- A plane passing through the tip of 9th costal cartilage and midway between median vertical plane
- Anteriorly it passes through tip of 9th costal cartilage and posteriorly it passes through lower part of body of L1 vertebra
- The Pylorus, inferior margin of liver, neck of the gallbladder, anterior end of spleen, hilum of kidney, portal vein, etc. lie at this level.
Subcostal Plane
- A transverse plane passing just below 10th rib
- Lies at the upper border of L3 vertebra.
Transtubercular Plane
- Transverse passing through the level of tubercle on the iliac crest
- Lies at the upper border of L5 vertebra
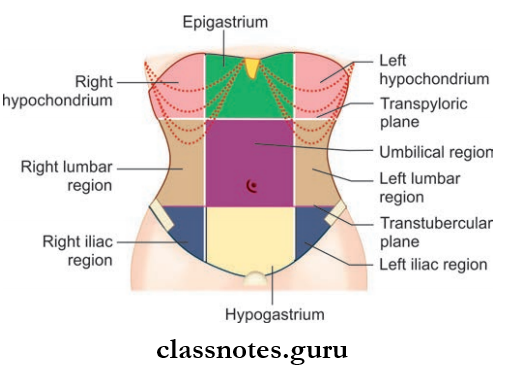
The Abdominal Cavity Is Divided Into Nine Regions By
- Two transverse planes
- Two vertical planes
- Upper Transverse Plane: Transpyloric plane
- Lower Transverse Plane: Transtubercular plane
- Vertical Planes: Right and left lateral vertical planes.
- Nine regions from above to downwards and from right to left are:
- Right hypochondrium
- Right lumbar
- Right iliac fossa
- Epigastrium
- Umbilical
- Hypogastrium
- Left hypochondrium
- Left lumbar
- Left iliac fossa
Question 4. Describe about the features, formation, and contents of the rectus sheath.
Answer:
Rectus Sheath
- Rectus Sheath is an aponeurotic sheath formed from the aponeurosis of felt muscles of the anterior abdominal wall
- Rectus Sheath encloses:
- Rectus abdominis muscle
- Pyramidalis muscle
- Rectus Sheath Has Two Walls: Anterior And Posterior
- Anterior Wall:
- Rectus Sheath Anterior Wall is complete, and covers the entire extend of muscle from the upper end to the lower end
- Rectus Sheath AnteriorWall fimly adheres to tendinous intersections of the rectus abdominis muscle
- Posterior Wall
- Rectus Sheath Posterior Wall is incomplete, it is deficient above and below
- Rectus Sheath Posterior Wall is free from the Rectus abdominis muscle.
- Anterior Wall:
Anterior Abdominal Wall Muscles
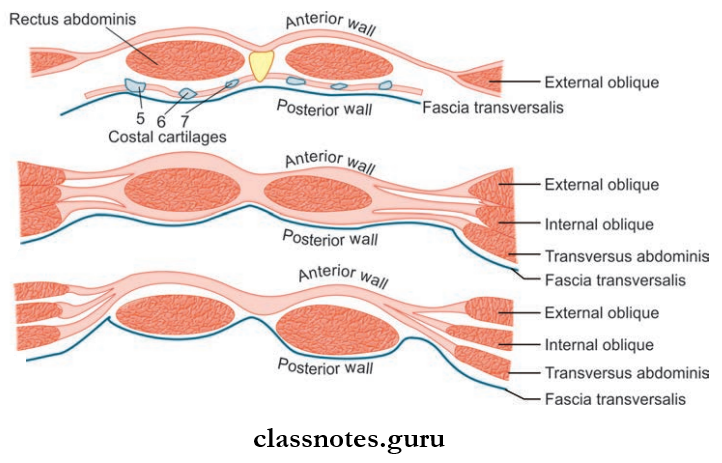
Rectus Sheath Formation
- AboveThe Costal Margin
- Anterior Wall: By external oblique aponeurosis
- Posterior Wall: It is deficient (here rectus abdominis lies directly on 5th 6th and 7th costal cartilages)
- Between The Costal Margin And Arcuate Line (Lies At The Level Of The Anterior Superior Iliac Spine).
- Anterior Wall:
- By external oblique aponeurosis
- Anterior lamina of aponeurosis of internal oblique
- Posterior Wall:
- Transversus abdominis aponeurosis
- Posterior lamina of aponeurosis of internal oblique
- Anterior Wall:
- Below The Arcuate Line
- Anterior Wall:
- By the aponeurosis of all three flt muscles of anterior abdominal wall (internal oblique, external oblique, transversus abdominis)
- External oblique aponeurosis contributes separately whereas aponeurosis of internal oblique and transversus abdominis fuses with each other
- Posterior Wall: It is deficient.
- Anterior Wall:
Rectus Sheath Contents
- Muscles: Rectus abdominis and pyramidalis
- Blood Vessels: Superior and inferior epigastric arteries and veins
- Nerves: Terminal parts of:
- Lower fie intercostal nerves
- Subcostal nerves.
Rectus Sheath Applied Anatomy
- Rectus sheath maintains the strength of the anterior abdominal wall
- Rectus sheath also checks the boing of the rectus abdominis muscle, thus increasing the efficiency of the rectus muscle.
Question 5. What is fascia transversalis, Briefly describe its extent and modifications.
Answer:
Fascia Transversalis
- Fascia lining the inner surface of the transversus abdominis muscle
- Fascia transversal is separated from the peritoneum by the extraperitoneal connective tissue
Anterior Abdominal Wall Nerve Supply
Fascia Transversalis Extent:
- Superiorly: Continuous with the diaphragmatic fascia
- Inferiorly: Continuous with fascia iliaca
- Anteriorly: Adherent to linea alba at a level above the umbilicus
- Posteriorly: Continuous with an anterior layer of the thoracolumbar fascia
Modifiations Of Fascia Transversalis
- In the fascia transversalis there is an oval opening of about 1.2 cm above the midinguinal point, known as deep inguinal ring.
- Mid Inguinal Point: Midpoint between the anterior superior iliac spine and the symphysis pubis.
- MidPoint Of Inguinal Ligament: Midpoint of the anterior superior iliac spine and pubic tubercle.
- Two Prolongations:
- Internal Spermatic Fascia: Tubular prolongation of fascia transversalis, which surrounds the spermatic cord
- The Anterior Wall Of Femoral Sheath: Prolongation of fascia transversalis into the thigh over the femoral vessels
- Iliopubic tract: Thckened inferior margin of fascia transversalis.
Question 6. Describe the inguinal canal including its boundaries, contents, and inguinal rings, and also give a brief description about the spermatic cord and its contents.
Answer:
Inguinal Canal
- Inguinal Canal is an oblique intermuscular passage in the lower part of anterior abdominal wall (site of potential weakness in the lower part of anterior abdominal wall)
- Lies just above the medial half of the inguinal ligament
- The inguinal Canal is larger in males than in females
- The inguinal Canal allows the passage of structures, from the testis to the abdomen in males and round ligament in females
- Inguinal Canal Length: 4 cm
- Inguinal Canal Extent: From deep inguinal ring to superficial inguinal ring
- Inguinal Canal Direction: Downwards, forwards, and medially.
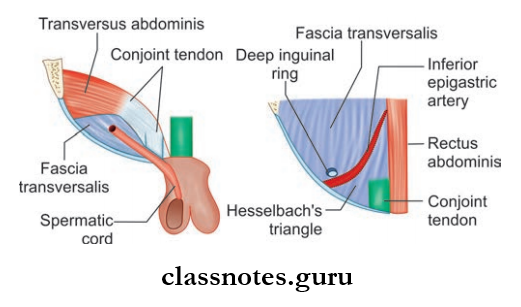
Deep Inguinal Ring: Oval opening in the fascia transversalis, 1.25 cm above the mid inguinal point.
Anterior Abdominal Wall Blood Supply
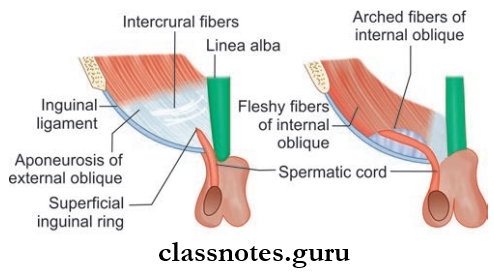
Superfiial Inguinal Ring
- The triangular gap in the external oblique aponeurosis
- Lies above and lateral to the pubic crest
- Base of the triangle is formed by the pubic crest
- Lateral or medial margins or crura form the sides of triangle
- Length – 2.5 cm, breadth – 1.25 cm.
Inguinal Canal Boundaries
- Anterior Wall
- In The Whole Extent
- Skin
- Superficial fascia
- External oblique aponeurosis
- Lateral 2/3 rd
- Internal oblique muscle
- In The Whole Extent
- Posterior Wall
- In The Whole Wxtent
- Fascia transversal
- Extraperitoneal tissue
- Parietal peritoneum
- Medial 2/3 rd
- Conjoint tendon
- Reflcted part of inguinal ligament
- Lateral 1/3 rd
- Interfoveolar ligament
- In The Whole Wxtent
- Roof: Arched fiers of internal oblique and transversus abdominis muscle.
- Floor: Inguinal ligament and lacunar ligament.
Inguinal Canal Contents
- Male: Spermatic cord, ilioinguinal nerve
- Female: Round ligament of uterus, ilioinguinal nerve.
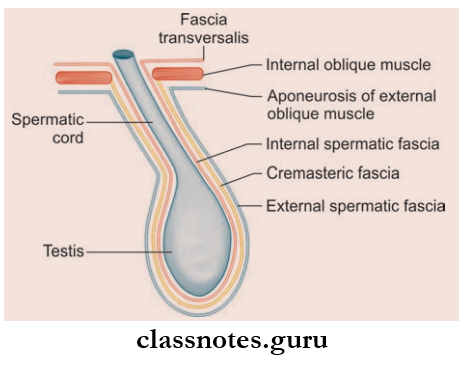
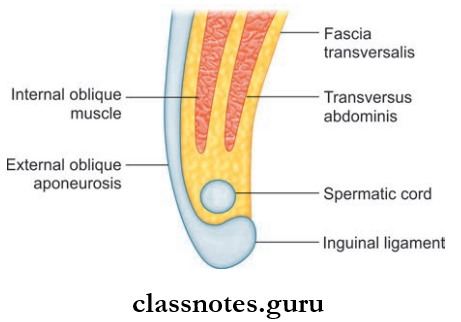
Coverings Of The Spermatic Cord
- Internal Spermatic Fascia: Derived from fascia transversalis, covers the cord completely
- Cremasteric Fascia: Derived from internal oblique and transversus abdominis muscles, covers the cord above the level of the above-mentioned muscles
- External Spermatic Fascia: Derived from external oblique aponeurosis, covers the cord below the superficial inguinal ring.
Contents Of The Spermatic Cord
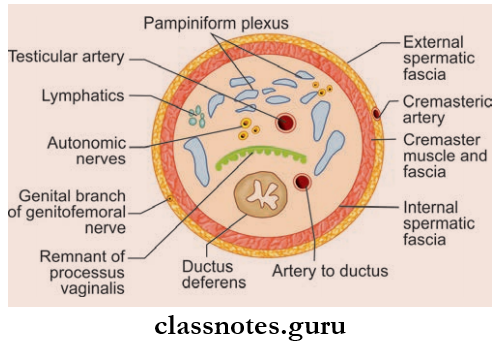
- Ductus deferens
- Arteries: Testicular artery, cremasteric artery, artery to ductus deferens
- Pampiniform plexus of veins
- Nerves:
- Genital branch of genitofemoral nerve
- Sympathetic nerve plexus around the artery to ductus deferens
- Lymphatics from the testis
- Remnants of processus vaginalis.
Mnemonics: Inguinal canal walls: ‘MALT: 2M, 2A, 2L, 2T’:
- Starting from the superior, moving around in order to posterior
- Superior Wall (Roof): 2 Muscles:
- Internal oblique Muscle
- Transverse abdominis Muscle
- Anterior Wall: 2 Aponeuroses:
- Aponeurosis of external oblique
- Aponeurosis of internal oblique
- Lower Wall (Flor): 2 Ligaments:
- Inguinal Ligament
- Lacunar Ligament
- Posterior Wall: 2Ts:
- Transversalis fascia
- Conjoint Tendon
Anterior Abdominal Wall Landmarks
Question 7. Describe about the mechanism of the inguinal canal preventing inguinal herniation and write a note on the inguinal hernia and Hesselbach’s triangle.
Answer:
The Mechanism Of The Inguinal Canal Preventing Inguinal Herniation:
- The presence of the inguinal canal causes a weakness in the lower part of the anterior abdominal wall as a result there is a chance of herniation of abdominal viscera into the inguinal canal
- But this is prevented by the following mechanisms:
- Flap Valve Mechanism:
- The inguinal canal is oblique (in children it is straight)
- Deep and superficial inguinal rings do not lie opposite to each other
- So when the intra-abdominal pressure increases, the anterior and posterior walls of the canal get approximated, like a flip obliterating the passage
- Guarding Of Inguinal Rings:
- Deep Inguinal Ring: Guarded by internal oblique muscle
- Superfiial Inguinal Ring: Guarded by conjoint tendon and reflcted part of inguinal ligament
- Shutter Mechanism:
- Internal oblique muscle forms the anterior wall, roof, and posterior wall of the canal
- When it is contracted the roof is pulled and gets approximated on the floor, like a shutter— obliterating the passage
- Ball Valve Mechanism:
- Contraction of cremasteric muscle pulls the testis up and this helps the spermatic cord to plug the superficial inguinal ring
- Slit Valve Mechanism:
- Contraction of the external oblique approximates the two crura of the superficial inguinal ring (like a slit valve).
Hesselbach’s Triangle Or Inguinal Triangle: Situated on the posterior wall of inguinal canal
Anterior Abdominal Wall Hernias
Hesselbach’s Triangle Or Inguinal Triangle Boundaries
- Medially: Lateral border of rectus abdominis muscle (lower 5 cm)
- Laterally: Inferior epigastric artery
- Inferiorly: Medial half of the inguinal ligament
- Floor:
- Fascia transversalis
- Peritoneum
- Extraperitoneal tissue.
Hesselbach’s Triangle Or Inguinal Triangle Applied Anatomy
Direct hernias occur commonly through Hesselbach’s triangle.
Inguinal Hernia
- It is the abnormal protrusion of a viscus or a part of it through the inguinal canal
- There Are Two Types Of Inguinal Hernias:
- Direct
- Indirect
Indirect Inguinal Hernia
- Most common type of hernia
- In an indirect inguinal hernia, the hernia sac enters the inguinal canal through the deep inguinal ring into the inguinal canal
- Common in children and young adults, male > female
- Commonly occurs due to persistent processus vaginalis sac
- It Can Be:
- Congenital: Persistent processus vaginalis sac
- Acquired: Increased intra-abdominal pressure, for example, weight lifting.
Types Of Indirect Hernia
- Complete Hernia: Hernial sac extent from deep inguinal ring to superficial inguinal ring to bottom of scrotum
- Funicular: Hernial sac extent from deep inguinal ring to root of scrotum
- Bubonocele: Hernial sac is present in the inguinal canal only.
Direct Inguinal Hernia
- Occurs through Hesselbach’s triangle (due to weakness in the posterior wall of the inguinal canal)
- Always congenital
- The precipitating factor is the weakness of fiers of transversus abdominis
- Occurs in elderly due to chronic cough, in smokers (decreased strength of abdominal muscles due to decreased elastin).
Boundaries Of Anterior Abdominal Wall
Coverings of Hernial Sac (outside to inside)
- Indirect hernia
- Skin
- Superfiial fascia (campers and scarpas)
- External spermatic fascia
- Cremaster muscle and fascia
- Internal spermatic fascia
- Extraperitoneal fat
- Peritoneum
- Direct hernia
- Skin
- Superfiial fascia (campers and scarpas)
- External oblique aponeurosis
- Conjoint tendon
- Fascia transversalis
- Peritoneum
Anterior Abdominal Wall Multiple Choice Questions And Answers
Question 1. All the following structures pass through the inguinal canal except:
- Inferior epigastric artery
- Ilioinguinal nerve
- Spermatic cord
- Genital branch of genitofemoral nerve
Answer: 1. Inferior epigastric artery
Question 2. The posterior wall of the inguinal canal is mainly formed by:
- Fascia transversalis and conjoint tendon
- Internal oblique
- External oblique
- All of the above
Answer: 1. Fascia transversal and conjoint tendon
Question 3. Which of the following is a common structure in Hesselbach’s triangle and femoral (scarps) triangle?
- Conjoint tendon
- Rectus femoris
- Inguinal ligament
- Inferior epigastric artery
Answer: 3. Inguinal ligament
Anterior Abdominal Wall Examination
Question 4. The superior ¾ of the posterior rectus sheath is comprised of what layers?
- Aponeurosis of external abdominal oblique and internal abdominal oblique
- The aponeurosis of internal abdominal oblique and transverse abdominal muscle
- The aponeurosis of external and internal abdominal oblique and transverse abdominal muscle
- Transversalis fascia
Answer: 2. Aponeurosis of internal abdominal oblique and transverse abdominal muscle
Question 5. The median umbilical fold contains which of the following embryonic remnant(s)?
- Urachus
- Umbilical arteries
- Superior epigastric arteries
- Inferior epigastric arteries
Answer: 1. Urachus