
Cysts And Tumours Of Odontogenic Origin Important Notes
- Cyst
- Cyst Definition
- A cystis a soft fluctuant swelling containing fluid in a sac lined by epithelium and endothelium
- Cyst Classification
- Congenital cysts
- Sequestration dermoid
- Tubulodermoid or tubuloembryonic cyst
- Cysts of embryonic remnants
- Acquired cyst
- Retention cyst
- Distension cyst
- Exudation cyst
- Degeneration cyst
- Cystic tumours
- Implantation dermoid
- Traumatic cyst
- Parasitic cysts
- Congenital cysts
- Cyst Definition
- Radiological Types Of Dentigerous Cyst
- Central
- Covers crown of unerupted teeth
- Circumferential
- Covers the crown from all sides t. Lateral
- Covers Crown From Side
- Seen in partially erupted and mesioangular impaction of mandibular molar
- Central
- Complications Of Dentigerous Cyst
- Ameloblastoma
- Epidermoid carcinoma
- Mucoepidermoid carcinoma
- Phases Of Aneurysmal Bone Cyst
- Osteolytic initial phase
- Active growth phase
- Mature stage
- Healing phase
- Odontogenic Keratocyst
- Arises from
- Dental lamina
- The primordium of developing tooth germ
- The basal layer of oral epithelium
- Characteristic histological feature
- Cystic lumen containing a large amount of desquamated cells
- Formation of multiple small micro cysts called satellite cysts
- The fibrous capsule is devoid of inflammatory cells
- Hyalinization may occur
- Arises from
- Phases Of Development Of Radicular Cyst
- Phase of proliferation
- Phase of mystification
- Phase of enlargement
- Gorlin’s Cyst
- Gorlin’s Cyst is an odontogenic cyst of the jawbone
- Causes bony hard swelling of the jaw
- Ghost cells are characteristic features of it
- Classification Of Odontogenic Tumors
- Benign Tumors
- Epithelial origin
- Ameloblastoma
- Calcifying epithelial odontogenic tumor
- Epithelial origin
- Mesenchymal Origin
- Ameloblastic fibroma
- Calcifying epithelial odontogenic cyst
- Odontoma
- With Epithelial And Mesenchymal Origin
- Odontogenic fibroma
- Malignant Tumour
- Odontogenic carcinoma
- Malignant Ameloblastoma
- Primary intraosseous carcinoma
- Odontogenic carcinoma
- Odontogenic Sarcoma
- Ameloblastic fibrosarcoma
- Ameloblastic fibrodentinosarcoma
- Odontogenic Carciosarcoma
- Benign Tumors
- Pindborg Tumour
- Arises From
- Cells of stratum intermedium of darnel organs
- Reduced enamel epithelium
- Remnants of dental lamina
- Consists of sheets or islands of closely packed cells arranged in a cribriform pattern
- Amyloid gets deposited between tumor cells
- Arises From
- Ameloblastoma
- It is a true neoplasm of enamel organ-type tissue which does not undergo different to the point enamel formation
- Derived From
- Cell rests of Serres or epithelium rests of Malassez
- Epithelium of odontogenic cyst
- Disturbances of developing epithelium of jaws
- Heterotropic epithelium in other parts of the body
- AOT Arises From
- Enamel organ
- Epithelial lining of dentigerous cyst
- Epithelial rests of Malassez
- Remmants of dental laminma
- Odontomes
- They are common hamartomatous odontogenic lesions with limited growth potential
- Odontomes Types
- Complex odontoma
- Compound odontoma
- Radiograph Appearance
- Complex odontoma – sunburst appearance
- Compound odontoma – a big teeth appearance
Cysts And Tumours Of Odontogenic Origin Long Essays
Question 1. Classify benign and malignant tumors of the oral cavity. Write in detail about the clinical features histological features and radiographical features of ameloblastoma.
Answer:
Benign And Malignant Tumors Of The Oral Cavity Classification:
- Benign Tumors
- Epithelial origin
- Ameloblastoma
- Calcifying epithelial odontogenic tumor
- With mesenchymal origin
- Ameloblastic fibroma
- Calcifying epithelial odontogenic cyst
- Odontoma
- With epithelial and mesenchymal origin
- Odontogenic fibroma
- Epithelial origin
- Malignant Tumors
- Odontogenic carcinoma
- Malignant ameloblastoma
- Primary intraosseous carcinoma
- Odontogenic sarcoma
- Ameloblastic fibrosarcoma
- Ameloblastic fibrodentinosarcoma
- Odontogenic carcinosarcoma
- Odontogenic carcinoma
Ameloblastoma: Ameloblastoma is a benign locally aggressive neoplasm arising from odontogenic epithelium
Read And Learn More: Oral Pathology Questions and Answers
Ameloblastoma Clinical Features:
- Age- 1st-7th decade of life
- Sex- both sexes are equally affected
- Pain and swelling occur in the involved area
- Swelling is slow enlarging, painless, ovoid, bony hard
- expansion and distortion of cortical plates
- Pain and paraesthesia
- Inflammation
- Dental trauma
- Ulceration of mucosa
- Loosening of teeth
- Epitaxis
- Nasal obstruction
- Larger lesions cause fluctuations in the affected area
- Thin shell of bone near lesion cracks under digital pressure called eggshell crackling
- Pathological fractures
- Extraosseous ameloblastoma produces small, nodular growth in the gingiva
Ameloblastoma Types:
- Solid or multicystic ameloblastoma
- Slow-growing locally invasive ameloblastoma
- High recurrence rate
- Unicystic type
- The lesion can be enucleated
- Rarely seen in maxilla
- Recurrence rate is low
- Peripheral ameloblastoma
- Does not invade bone
- Treated in early stages of development
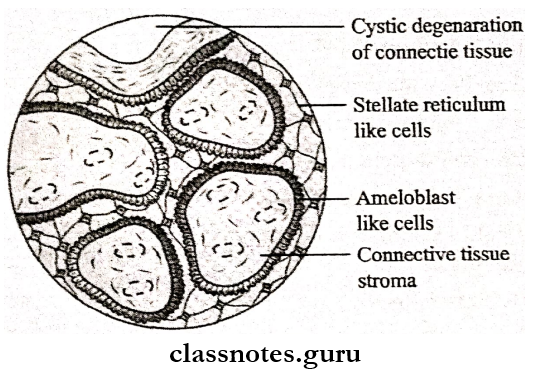
Ameloblastoma Histopathology:
- Plexiform Ameloblastoma
- Neoplastic epithelial cells proliferate in the form of long continuous anastomosing strands or cords
- Form fishnet pattern
- Peripheral cells are tall columnar resembling ameloblasts
- The center portion of strands consists of triangular-shaped cells resembling stellate reticulum cells
- Cells between columnar and stellate reticulum cells resemble stratum intermedium
- Connective tissue is loose and vascular
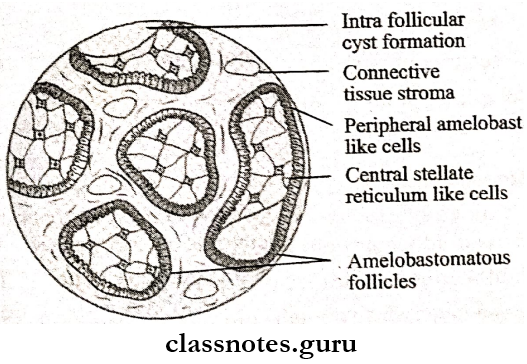
- Follicular Ameloblastoma
- Epithelial cells proliferate in the form of multiple, discrete follicles or islands
- It resembles an enamel organ
- Peripheral cells are tall columnar resembling ameloblasts with reverse polarization
- The center of the follicles consists of loosely arranged, polyhedral or triangular
- Cells between a peripheral and central group of cells appear stratum intermedium
- Microcyst formation is seen within connective tissue stroma
- Connective tissue consists of collagen bundles, fibroblasts, and blood vessels
Ameloblastoma Radiological Features
- Presents as well well-defined multilocular radiolucent area
- If locules are large it gives a soap bubble appearance
- If locules are small present as a honeycomb
- Causes expansion and distortion of cortical plates
- Margins are irregular and scalloped
- Root resorption is seen
- Causes expansion of the lower border of the mandible
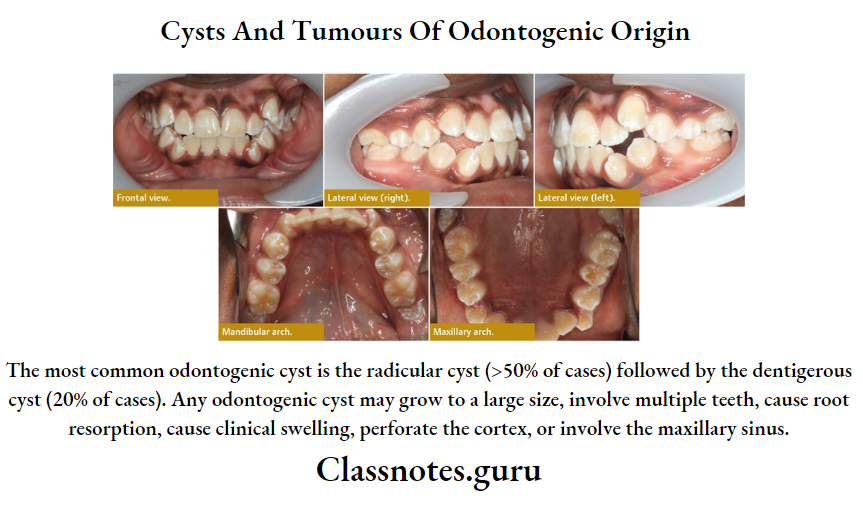
Question 2. Define cyst. Classify cysts of odontogenic origin. Write in detail about the dentigerous cyst.
Answer:
Cyst: It is a pathological cavity containing fluid, semi-fluid, or gas which is usually lined by epithelium and is not formed by the accumulation of pus
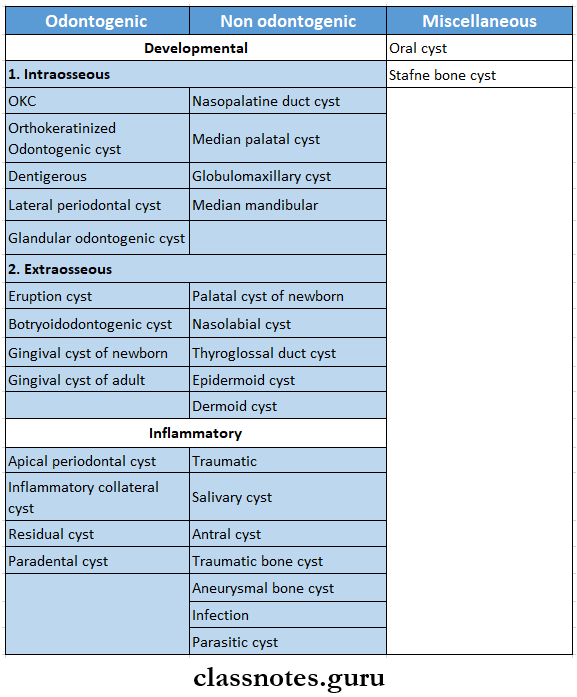
Cysts Of Odontogenic Origin Classification:
- Epithelial Cyst
- Odontogenic cysts
- Developmental cysts
- Primordial cyst
- Gingival cysts of infants
- Dentigerous cyst
- Calcifying epithelial odontogenic cyst
- Inflammatory cyst
- Radicular cyst
- Residual cyst
- Paradental cyst
- Developmental cysts
- Nonodontogenic cysts
- Nasopalatine cyst
- Globulamaxillary cyst
- Nasolabial cyst
- Odontogenic cysts
- Non-epithelial Cyst
- Simple bone cyst
- Traumatic bone cyst
- Solitary bone cyst
- Aneury bone cyst
Dentigerous Cyst: It is an odontogenic cyst covering the crown of impacted teeth
Dentigerous Cyst Clinical Features:
- An age-1st-3rd decade of life
- Sex- common in males
- Site- Mandibular 3rd molar, maxillary canines, maxillary 3rd molar
- Causes expansion of bone
- Palpation of the affected area of bone gives the crepitus-like sensation
- Smaller lesions are asymptomatic
- Pain occurs when it gets secondarily infected
- Facial asymmetry
- Displacement of adjacent teeth
- Resorption of roots
- Paraesthesia and anesthesia on the affected area
- Pathological fractures may occur
Dentigerous Cyst Radiological Features:
- Unilocular, well-defined radiolucency
- Has sclerotic margin
- Displacement of the tooth is seen
- Large cyst look multiloeular
- Expansion and distortion of cortical plates
- Resorption of roots
Dentigerous Cyst Types:
- Central
- Covers the crown of an unerupted tooth
- Pushes involved tooth away from its direction eruption
- Circumferential
- Covers the crown from all sides
- Lateral Type
- Covers the crown from the side
- Seen in partially erupted and mesioangular impaction of mandibular molar
Dentigerous Cyst Histopathology:
- The cystic cavity is lined by a thin Liver of non-keratinized, odontogenic epithelium
- Cells are flat or cuboidal in shape
- They may undergo mucous metaplasia
- Nest islands and strands of odontogenic epithelium are set within the capsule
- Localized areas of the bud-like proliferation of cystic epithelial cells known as mua proliferation
- Discontinuity of epithelium is seen when the cyst gets secondarily infected
- The epithelium is- supported by loosely arranged connective tissue
- Connective tissue stroma consists of young fibroblast cells separated by mucopolysaccharides and collagen bundles
Question 3. Describe the pathogenesis and histological features of odontogenic keratocyst and radiographical features.
(or)
Give clinical features and histological features of the primordial cyst.
Answer:
Odontogenic Keratocyst: Odontogenic keratocyst is a common cystic lesion of the jaw that arises from remnants of tire dental lamina
Odontogenic Keratocyst Pathogenesis: Odontogenic keratocyst arises from
- Dental lamina
- The primordium of developing tooth germ
- Basal lover of oral epithelium
- Develops due to cystic degeneration of cells of stellate reticulum in developing tooth germ
Odontogenic Keratocyst Clinical features:
- Age- 2nd-3rd decade of life
- Sex- common in males
- Site- common in the mandible
- It is an asymptomatic condition
- If gets secondarily infected, causes the expansion of cortical plates
- Mobility of teeth
- Pain and tenderness of the involved area
- Extradsseous lesions may develop over gingiva
- Multiple lesions develop in association with nevoid basal cell carcinoma syndrome
- Paraesthesia of lower lip and teeth
- Discharge of pus
- Maxillary lesions cause displacement or destruction of the floor of the orbit and protrusion of the eyeball
Odontogenic Keratocyst Histopathology:
- The cystic cavity is lined by uniform keratinized stratified odontogenic epithelium
- Epithelium exhibits para-keratinization
- The basal layer consists of tall columnar or cuboidal cells
- Cells have basophilic nuclei with reverse polarity
- Howell-defined granular layer
- Cells in the suprabasal layer are polyhedral in shape
- Mitotic activity is high
- Cystic lumen contains large amounts of desquamated keratin
- Formation of multiple small micro cysts called daughter cysts or satellite cysts
- A fibrous capsule is usually thin and devoid of inflammatory cells
- Syndrome-associated cysts consist of thick epithelium lining and nests of basaloibudding offending-off from cystic lining
- Hyalinization may occur in the cyst capsule
Odontogenic Keratocyst Radiological features
- Unilocular or multilocular radiolucency
- Margins: well-defined sclerotic margins
- Scalloping of border
- In the multilocular variant, the central cavity with satellite cysts is observed
- Expansion of cortical plates
- Proximity of cortical plates
- Soap bubble appearance
Odontogenic Keratocyst Classification:
Question 4. Write the etiology and histological features of Gorlin’s cyst.
Answer:
Calcifying Epithelial Odontogenic Cyst/Gorlin’s Cyst: It is a rare odontogenic cystic lesion of the jawbone
Gorlin’s Cyst Clinical Features:
- Age- 2nd decade of life
- Sex- both sexes are equally affected
- Site- mandibular premolars, anterior of maxilla
- Size- 2-3 cm in diameter
- Causes bony bard swelling of the jaw
- Expansion and distortion of cortical plates
- Involved teeth are vital
- Extraosseous lesions are circumscribed, sessile, or pedunculated gingival swelling
- Perforation of cortex
Gorlin’s Cyst Histopathology:
- The cystic cavity is lined by keratinized epithelium
- Some cells resemble stellate reticulum
- Basal cells are columnar or cuboidal
- The presence of many ghost cells occurs
- They are swollen, eosinophilic, abnormally keratinized, devoid of nuclei
- They become paler leaving a faint outline
- Ghost cells fuse to form a larger cellular mass which fills up the cystic lumen
- Ghost cells undergo calcification
- Cystic lumen consists of multiple, small, basophilic calcified bodies
- Melanin pigmentation occurs in cysts
- Connective tissue capsule contains satellite micro cysts and multiple multi-nucleated giant cells
Question 5. Describe pathogenesis, clinical features, histopathology, radiological features, and differential diagnosis of calcifying epithelial odontogenic tumor or Pindborg tumor
Answer:
Calcifying Epithelial Odontogenic Tumour/ Pindborg Tumour:
Calcifying Epithelial Odontogenic Tumour is a locally aggressive neoplasm
Pindborg Tumour Pathogenesis:
- It arises from
- Cells of stratum intermedium of enamel organ
- Reduced enamel epithelium
- Remnants of dental lamina
Pindborg Tumour Clinical Features:
- Age- Middle age
- Sex- both sexes are equally affected
- Site- mandible over gingiva
- Present as slow enlarging bony hard swelling
- Causes expansion of cortical plates
- Displacement of teeth
- Pain
- Paresthesia
- Maxillary lesions lead to nasal airway obstruction
- Nodular swelling over the gingiva occurs
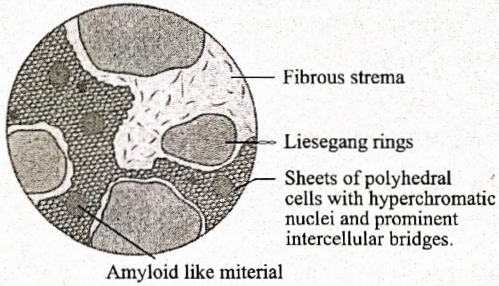
Pindborg Tumour Histopathology:
- Tumour consists of sheets or islands of closely packed, polyhedral epithelial cells
- Neoplastic cells have a cribriform arrangement
- Cells contain oval-shaped nuclei, prominent nucleoli, eosinophilic cytoplasm
- The presence of prominent intercellular bridges
- Amyloids get deposited between tumor cells
- Several calcified bodies or masses occur within the lesion
- These masses are arranged as concentrically laminated rings
- Such masses fuse to form large complex masses within tissue
- A large number of clear cells are found
- It is a non-capsulated lesion
Pindborg Tumour Radiological Features:
- Presents as a well-defined, multilocular radiolucent area
- Calcification within the tumor appears as multiple, small, radiopaque foci
- This produces a driven snow appearance
- The border of the lesion is scalloping
- Expansion and destruction of cortical plates
- Perforation of cortical plates
Pindborg Tumour Pathological fractures
- Larger lesions produce mixed features of radiolucency and radiopacity
- Peripheral lesions cause superficial cupped-out erosion of the cortical bone
Calcifying Epithelial Odontogenic Tumour Differential Diagnosis:
- Calcifying epithelial odontogenic cyst
- Adenomatoid odontogenic tumor
- Poorly differentiated carcinoma
- Ameloblastoma
- Dentigerous cyst
- Central ossifying fibroma
Question 6. Classify odontogenic tumor. Describe in detail odontomas
Answer:
Odontomes: Common hamartomatous odontogenic lesions with limited growth potential
Pindborg Tumour Types:
- Complex Odontoma: Consists of a mass of haphazardly arranged enamel, dentin, and cementum
- Compound Odontoma: Consists of collections of numerous small, discrete, tooth-like structures
Pindborg Tumour Clinical Features:
- Age: children and young adults
- Sex: both
- Site: compound- in the maxilla
- Complex- mandible
- Small asymptomatic lesion
- Size- varies from small to 6 cm in diameter
- Expansion of cortical plates
- Displacement of regional teeth
- Impacted or retained deciduous teeth
- Pain, inflammation
- Ulceration
- Fistula formation
Pindborg Tumour Radiographic Features:
- Appears as well-defined radiolucencies with well-corticated borders
- Surrounded by a thin radiolucent zone representing a capsule
- Pindborg Tumour Compound- A bag of teeth appearance
- Appear as numerous, small miniature teeth or tooth-like structures projecting from a single focus
- Present between roots of erupted permanent teeth or above the crown of impacted teeth
- Pindborg Tumour Complex- sunburst appearance
- Radiopaque mass within jawbone is present
- Pindborg Tumour Compound- A bag of teeth appearance
Pindborg Tumour Histopathology:
- Small islands of epithelial host cells are seen
- Odontomes contain soft tissue consisting of odontogenic epithelium, secretory ameloblasts, developing enamel organs, reduced enamel epithelium, odontoblasts, and cementoblasts
- Compound Odontoma
- There is the presence of multiple separate denticles embedded in fibrous tissue stroma
- Consist of enamel, dentin, cementum, and- pulp tissues
- Number of denticles- varies from 2-3 to 20-30
- Complex Odontoma
- Consists of irregularly arranged enamel, dentin, cementum, and pulp
- Enamel is fully calcified and appears as small clefts or circular empty spaces
- Dentin forms the bulk of tissue
- It lies in direct contact with connective tissue
- Cementum is present as a thin layer at the periphery of the tumor
- Compound Odontoma
Pindborg Tumour Treatment: Surgical enucleation
Question 7. Describe the clinical and histological features of adenoameloblastoma.
(or)
Describe in detail about adenomatoid odontogenic tumour
Answer:
Adenomatoid Odontogenic Tumour:
- Also known as adenoameloblastoma or ameloblastic-adenomatoid tumor
- It is a well-circumscribed tumor characterized by the formation of multiple duct-like structures by neoplastic epithelial cells
- Origin: Reduced enamel epithelium
Adenomatoid Odontogenic Tumour Clinical Features:
- Age: Young age
- Sex: Common in Female
- Site- Maxillary anterior region
- Present as slow enlarging, small, bony hard swelling
- Elevation of the upper lip
- Displacement of teeth
- Expansion of cortical plates
- Associated with unerupted teeth
- Nodular swelling occurs over gingiva
Adenomatoid Odontogenic Tumour Radiographic Features:
- Well-defined, unilocular, radiolucent area enclosing tooth or tooth-like structure
- Multiple interior small radiopaque foci are seen
- This is known as snow-flake calcifications
- Unilocular lesions are present between the roots of erupted teeth
- Expansion and distortion of cortical plates are seen
- There is displacement of roots
- The border of the lesion is not well-corticated
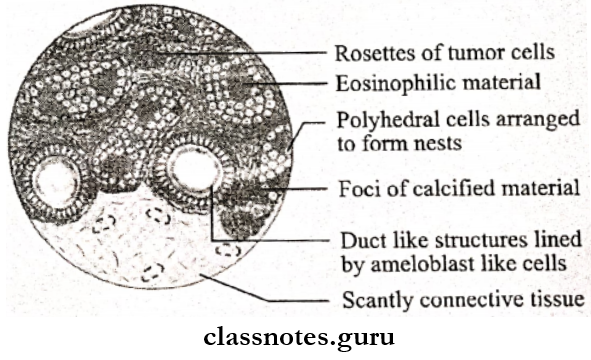
Adenomatoid Odontogenic Tumour Histopathology:
- Adenomatoid Odontogenic Tumour shows spindle-shaped, neoplastic odontogenic epithelial cells proliferating multiple duct-like patterns
- Each such structure is lined by a single layer of tall columnar cells resembling ameloblasts
- The nuclei of these cells are polarized away from central space
- Lumen of it is filled with homogenous eosinophilic coagulum
- Small foci of calcification are scattered all over the lesion
- Neoplastic cells are arranged in solid nests, sheets, or rosette-like patterns in some cases
- Connective tissue is loose and thin
- Neoplasm is well-capsulated
Cysts And Tumours Of Odontogenic Origin Short Essays
Question 1. Lateral periodontal cyst
Answer:
Lateral Periodontal Cyst
A lateral periodontal cyst develops in association with the lateral root surface of the erupted vital tooth
Lateral Periodontal Cyst Clinical Features:
- Occurs in adult males
- Commonly seen in maxillary and mandibular anterior region
- It is usually asymptomatic
- It appears as small, painless soft tissue swelling anterior to interdental papillae
- The overlying mucosa is normal
- Color- may be bluish
- Associated teeth are vital
- Size- less than 1 cm in diameter
Lateral Periodontal Cyst Histopathology:
- Present as a small cystic cavity lined by non-keratinized stratified squamous epithelium
- Epithelial cells appear flattened resembling reduced enamel epithelium
- Some papillary infolding is seen
- The epithelium contains a cluster of glycogen-rich, clear cells with vacuolated cytoplasm
- Connective tissue is non-inflamed
Question 2. Radicular cyst/ Periapical cyst
Answer:
Radicular Cyst
A radicular cyst is an odontogenic cystic lesion associated with the apex of a non-vital tooth
Periapical Cyst Pathogenesis:
- Phase Of Initiation
- Bacterial infection leads to stimulation of cell rest of Malassez
- Phase Of Proliferation
- Excessive and exuberant proliferation of cell rests
- Phase Of Mystification
- Deprivement of nutrition of central cells results in necrosis
- Cyst formation occurs
- Phase Of Enlargement
- Enlargement of the cavity occurs due to
- Higher osmotic tension of the cystic fluid
- Release of bone resorting factors
- Enlargement of the cavity occurs due to
Periapical Cyst Clinical Features:
- Age- young age
- Sex- common in males
- Site- common in maxillary anterior
- Involved teeth are nonvital
- Smaller cysts are asymptomatic
- Larger lesions produce slow enlarging, bony hard swelling
- Expansion and distortion of cortical plates
- Severe bone destruction
- The springiness of jaw bones
- Pain occurs if a secondary infection is present
- Intraoral and extraoral pus discharge
- Pathological fractures
- Formation of an abscess called “cyst abscess”
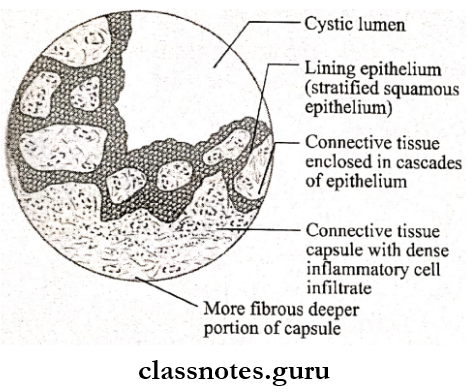
Periapical Cyst Histopathology:
- The cystic cavity is lined by nonkeratinized stratified squamous epithelium
- This epithelium is encircled by all the sides by a connective tissue capsule in an arcading pattern
- This capsule is made up of chronic inflammatory cell infiltration
Periapical Cyst Structures Seen Are:
- Goblet Cells
- Present in the lining of the cyst
- They are mucous-secreting cells
- Cholesterol Clefts
- They are multiple small, ribbon-shaped or needle-shaped, cleft-like spaces
- Present in the cystic lumen or connective tissue capsule
- Multiple Laminated Crescent-Shaped Or Hairpin-Shaped Hyaline Structures
- Rushton Bodies
- Present within cystic lining or in connective tissue
- Russell Bodies
- These are plasma cells surrounded by immunoglobulin
- Round Or Irregularly Shaped squamous epithelial islands within the capsule
Question 3. Aneurysmal bone cyst
Answer:
Aneurysmal Bone Cyst
An aneurysmal bone cyst is a cystic lesion involving bone anywhere in the body
Aneurysmal Bone Cyst Clinical Features:
- Age- second decade of life
- Sex- common in females
- Site-Mandibular molar-ramus area and maxillary posterior area
- Present as rapidly enlarging, diffuse, firm swelling of the jaw
- Causes facial asymmetry
- Swelling is painful
- Expansion and thinning of bone results in egg-shell crackling
- Perforation of cortical bone
- Pathological fracture of affected jawbone
- Paraesthesia of regional teeth
- Difficulty in mouth opening due to impingement on the capsule of TMJ
- Maxillary lesions cause nasal bleeding, pressure sensation in the eye and nasal obstruction
Aneurysmal Bone Cyst Radiological Features:
- Reveals multilocular radiolucent area resembling the honey-comb appearance
- The border is well-demarcated or diffuse
- There is a ballooning expansion of cortical plates
- Displacement of teeth and resorption of roots are seen
- Blow-out bulging of the lower border of the mandible is seen
Aneurysmal Bone Cyst Histopathology:
- Consists of multiple blood-filled spaces lined by spindle-shaped or flat endothelial cells
- Spaces are separated by loose connective tissue
- There is the presence of multiple multinucleated giant cells, scattered osteoids, areas of hemorrhage, and hemosiderin pigmentation
- The Cyst wall consists of a lace-like pattern of calcification
Question 4. Ameloblastic fibroma?
Answer:
Ameloblastic Fibroma
Ameloblastic fibroma is a benign odontogenic tumor containing both epithelial and mesenchymal components
Ameloblastic Fibroma Clinical Features:
- Age- below 20 years of age
- Sex- common in females
- The site commonly involved are mandibular posterior region
- Present as slow-growing, painless, bony hard swelling of the jaw
- It is asymptomatic
- Causes mobility of regional teeth and facial asymmetry
- It is associated with impacted or unerupted molar teeth
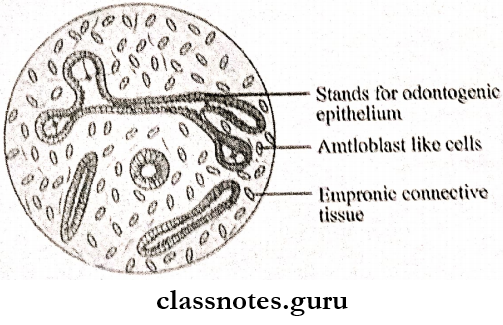
Ameloblastic Fibroma Histopathology: Ameloblastic fibroma consists of epithelial and mesenchymal components
- Epithelial Component
- Consist of multiple sharply defined strands, islands, or narrow cords
- Cells at the periphery of the cord are tall columnar resembling ameloblasts
- Center cells resemble stellate reticulum cells
- The epithelium component is bordered by a narrow cell-free zone of hyaline connective tissue
- Mesenchymal Component
- Consist of plump stellate or ovoid cells and loose fibroblastic stroma
- It resembles dental papilla
Question 5. Malignant potential of dentigerous cyst
Answer:
Malignant Potential Of Dentigerous Cyst
- A Dentigerous Cyst Leads To
- Epidermoid carcinoma
- Mucoepidermoid carcinoma of salivary gland
- Features Of Dentigerous Cyst That Leads To Malignancy Are
- Hyperchromatism of basal cell nuclei
- Polarization of basal cells
- Cytoplasmic vacuolization
- Presence of budding and protruding epithelial islands from lining epithelium
- Mucous secreting celts present leads to malignancy
Question 6. Potential complications of dentigerous cyst
Answer:
Potential Complications Of Dentigerous Cyst
- Ameloblastoma
- Arises from lining epithelium or nests of odontogenic epithelium
- Scellous Celt Carcinoma
- Mucoepidermoid Carcinoma
- Arises from lining epithelium of event
Question 7. Epidermoid cyst
Answer:
EpidermoidCyst
Epidermal cysts are the result of the implantation of epidermal elements and their subsequent cystic transformation
Epidermoid Cyst Etiology:
- Sequestration and implantation of epidermal rest during the embryonal period
- Iatrogenic or surgical implantation of the epithelium into jaw mesenchyme
Epidermoid Cyst Clinical Features:
- Age- third to fourth decade of life
- Sex- common in males
- Associated with Gardner syndrome
- Asymptomatic
- Pain and tenderness occur when the cyst becomes inflamed or infected
- Discharge of foul-smelling cheese-like material
- Difficulty in swallowing and feeding
- Difficulty in speech
- Appear as firm, round, mobile subcutaneous nodules
- Color- flesh-colored, yellow or white
Question 8. Gingival cyst of adult
Answer:
Gingival Cyst Of Adult
Gingival cysts in adults are small developmental odontogenic cysts of gingival soft tissue
Gingival Cyst Of Adult Clinical Features:
- Age- fifth and sixth decade of life
- Sex- common in females
- Site- common in the mandible
- Present over gingiva as firm, fluid-filled, dome-like swelling over gingiva
- Present over attached gingiva or interdental papil- lain canine-premolar area
- Size- less than 1 cm in diameter
- It is well-circumscribed
- Surface- smooth
- Color- normal or bluish
- Adjacent teeth are vital
Gingival Cyst Of Adult Histopathology:
- The cyst cavity is lined by thin epithelial lining made up of lat or cuboidal cells
- Cells contain pyknotic nuclei with perinuclear cytoplasmic vacuoles
- The cystic lumen contains layers of keratin
- Epithelial cells are arranged in a whorled pattern
- It may contain clear cells
Question 9. Hemorrhagic cyst
Answer:
Hemorrhagic Cyst
A hemorrhagic cyst is characterized by a cavity in bone lined by fibrous tissue
Hemorrhagic Cyst Clinical Features:
- Age- in young peoples
- Sex- common in females
- Site involved
- Mandibuar body, symphysis or ramus
- Maxillary anterior region
- It is asymptomatic
- It produces pain when secondarily infected
- Paraesthesia of lip
- Expansion of cortical plates
- Displacement of regional teeth
Hemorrhagic Cyst Pathogenesis:
Hemorrhagic Cyst Radiographic Features:
- Unilocular radiolucent area
- The cystic margin is well-demarcated
- It appears scalloping between the roots of the teeth
- Root resorption of adjacent teeth
Question 10. Cholesterol crystals
Answer:
Cholesterol Crystals
- Cholesterol crystals appear as clear needle-like spaces or cleft
- They get dissolved on histological examination
- Associated with multinucleated giant cells
- Seen in radicular cyst and odontogenic keratocyst
- Source
- Disintegration of RBC
- Degeneration and disintegration of lymphocytes and plasma cells
- Giant cells
- Circulating plasma lipids
- Cholesterol Crystals Complications
- Fistula formation
- Osteomyelitis
- Cellulitis
- Squamous cell carcinoma
Question 11. Globulomaxillary cyst
Answer:
Globulomaxillary Cyst
Globulomaxillary Cyst is a developmental or fissural cyst arising from bony suture between the maxilla and pre-maxilla
Globulomaxillary Cyst Clinical Features:
- Present as small swelling between the upper lateral incisor and canine
- Asymptomatic
- Pain occurs only when it is secondarily infected
- Elevation of the upper lip
- Associated teeth are vital
Globulomaxillary Cyst Radiographic Features:
- Shows the inverted pear-shaped radiolucent area between the roots of the upper lateral incisor and canine
- Causes divergence of roots of teeth
Globulomaxillary Cyst Histopathology:
- The cystic cavity is lined by stratified or pseudostratified ciliated columnar epithelium
- Connective tissue capsule consists of chronic inflammatory cell infiltration
Question 12. Rushton bodies
Answer:
Rushton Bodies
- Rushton bodies or hyaline bodies are linear or curved bodies
- They are brittle and fracture immediately
- Present within the lining epithelium of cyst-like a dentigerous cyst
- Source
- Keratinized secondary enamel cuticle
- Odontogenic epithelium
- Hematogenous origin from thrombi
Question 13. Enamel pearl
Answer:
Enamel Pearl
- Enamel pearl is also called ectopic enamel
- It is hemispheric or dome-shaped white calcified projections of enamel
- It is a localized bulging of the odontoblastic layer
- Appears radiopaque area
- Enamel Pearl Seen in
- Roots of maxillary molars
- Furcation areas
- Composed of normal enamel
Question 14. Ghost Cells
Answer:
Ghost Cells
- Ghost Cells occurs in a variety of odontogenic and nonodontogenic lesions
- Ghost cells contain nuclear remnants of cytoplasmic organelles and numerous tonofilaments
- They are large, vacuolated cells
- Their presence indicates proliferative odontogenic epithelium
- Reason For Its Formation
- Intracellular edema
- Presence of dilated degenerated membranous organelles
- Ghost Cells Seen In
- Odontomes
- Ameloblastoma
- Ameloblastic fibro-odon to mas
- Ameloblastic odontomas
Question 15. Golln Goltz syndrome
Answer:
Golln Goltz Syndrome
Golln Goltz Syndrome is transmitted as an autosomal dominant trait
Golln Goltz Syndrome Clinical Features: It is composed of
- Cutaneous Anomalies
- Basal cell carcinoma
- Benign dermal cysts and tumors
- Palmar pitting
- Palmar and plantar keratosis
- Dermal Calcinosis
- Dental Anomalies
- OKC
- Mild mandibular prognathism
- Rib anomalies
- Vertebral anomalies
- Brachymetacarpalism
- Cleft lip and palate
- Ophthalmologic Abnormality
- Hypertelorism with wide nasal bridge
- Dystopia canthorum, internal strabismus
- Congenital blindness
- Neurologic Anomalies
- Mental retardation
- Dural calcification
- Agenesis of corpus callosum
- Congenital hydrocephalus
- Medulloblastoma
- Sexual Abnormality
- Hypogonadism in males
- Ovarian tumours
Question 16. Liesegang rings
Answer:
Liesegang Rings
- Seen in CEOT or Pindborg tumour
- They are calcified masses or bodies found within the lesion
- They are hematoxyphilic around degenerating tumor cells
- Some of these structures are fused to form large complex masses
Cysts And Tumours Of Odontogenic Origin Viva Voce
- Odontogenic cysts are derived from epithelium associated with the development of dental apparatus
- Odontogenic keratocyst is derived from the rest of the dental lamina
- Odontogenic keratocyst (OKC) represents a central cavity having a satellite cyst
- A dentigerous cyst surrounds the crown of Impacted teeth
- Epstein’s pearls are found along Midpalatine raphe
- Bohn’s nodules are scattered over the palate mostly along the junction of the hard and soft palate
- A hyaline body called Rushton body is found in great numbers in the epithelium of residual cysts
- A globulomaxillary cyst is found within the bone between the maxillary lateral incisor and canine teeth
- The nasolabial cyst arises at the junction of the globular process, lateral nasal process, and maxillary process
- Liesegang rings are a form of calcification seen in the Pindborg tumor
- Hyaline rings found in AOT are duct-like structures lined by Eosinophilic rims of varying thickness
- Ghost cells are a characteristic feature of odontomas
- Adenoameloblastoma is commonly associated with missing teeth
- Snowflake calcifications are seen in adenoameloblastoma