Oral Medicine Developmental Disorders Short Answers
Question 1. Causes of angular cheilitis.
Answer:
Causes Of Angular Cheilitis
- Micro-organisms- Candida albicans, staphylococci, and streptococci
- Mechanical Factors:
- Overclosure of jaws in edentulous patients
- Nutritional deficiency:
- Due to Riboflavin
- Folate deficiency
- Iron deficiency
- General protein deficiency
- Diseases Of The Skin:
- Atopic dermatitis
- Seborrhoeic dermatitis
- Other Factors
- Hypersalivation
- Down’s syndrome
- Large tongue
- Presence of developmental sinus
Question 2. Concrescence.
Answer:
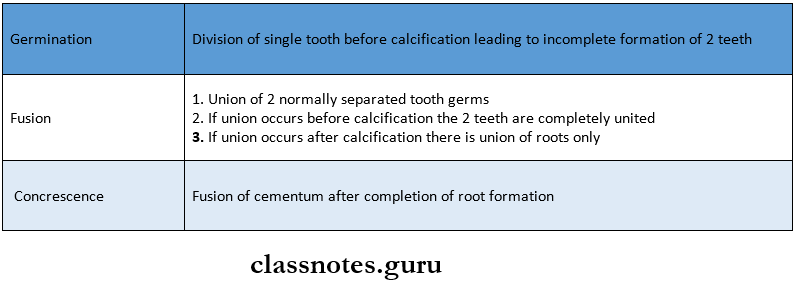
Concrescence
Concrescence is the union of the roots of two or more adjoining teeth due to the deposition of cementum
Etiology:
- Traumatic injury
- Crowding of teeth
- Hypercementosis
Concrescence Clinical Features:
- It is an acquired defect
- It occurs in both erupted or unerupted teeth
- There is no sex predilection
- Union or fusion does not occur between the enamel, dentin, or pulp of the involved teeth
- The union mostly occurs between two teeth, however, there may be a union between more than two teeth
- Permanent maxillary molars are usually affected
- It can occur between the normal molar and supernumerary molar
- It rarely involves deciduous dentition
- The condition is frequently seen in those areas of the dental arch where the roots of the neighboring teeth lie close to each other
Concrescence Significance:
- Concrescence may complicate extraction
Read And Learn More: Oral Medicine Question and Answers
Question 3. Taurodontism.
Answer:
Taurodontism
- Taurodontism is a peculiar developmental condition in which the crown of the tooth is enlarged at the expense of its roots
Taurodontism Pathogenesis:
- Taurodontism occurs due to failure of the Hertwig’s Epithelial root sheath to invaginate at the proper horizontal level
Taurodontism Clinical Features:
- Taurodontism involves both the sex
- Taurodontism commonly affects multi-rooted permanent molar teeth and sometimes premolar
- Taurodontism rarely occurs in primary dentition
- Taurodontism was relatively common in Neanderthal men
- The affected tooth exhibits an elongated pulp chamber with rudimentary roots
- The teeth are usually rectangular in shape with mini¬mum constriction at the cervical area
- The furcation area of the teeth is more apically placed
- The teeth often have greater apical-occlusal height
- Clinically the teeth exhibit certain morphological changes
Taurodontism Associated Syndrome:
- Down’s syndrome
- Klinefelter syndrome
- Poly X syndrome
Taurodontism Treatment:
Question 4. Four Causes of Macroglossia.
Answer:
- Congenital Or Developmental
- Inflammatory
- Syphilis
- Ludwig’s angina
- Typhoid
- Tuberculosis
- Infected wound
- Neoplasm
- Neurofibromatosis
- Lymphangioma
- Systemic
- Pellagra
- Down’s syndrome
- Acromegaly
- Uremia
- Amyloidosis
- Diabetes
- Scurvy
- Hurler’s syndrome
Question 5. Bald tongue/ Differential diagnosis of the bald tongue.
Answer:
- Congenital
- Familial dysplasia
- Epidermolysis bullosa
- Endocrine candidiasis
- Developmental
- Geographic tongue
- Median rhomboid glossitis
- Central papillary atrophy
- Chronic Trauma
- Nutritional Deficiency
- Pellagra
- Riboflavin
- Conditional deficiency
- Medication
- Antibiotic
- Cancer chemotherapy
- Peripheral Vascular Disease
- Chronic Candidiasis
- Tumor
- Squamous cell carcinoma
- Epidermoid carcinoma
- Miscellaneous
- Diabetes mellitus
- Oral submucous fibrosis
Question 6. Supernumerary teeth.
Answer:
Supernumerary Teeth
- The presence of any extra tooth in the dental arch in addition to the normal series of teeth is called supernumer¬ary teet
- Mode Of Formation:
- It may develop either from an accessory tooth bud in the dental lamina
- It may develop due to the splitting of regular normal tooth bud during the initial phase of odontogenesis
Supernumerary Teeth Clinical Features:
- It can occur in both the sex
- It may resemble the corresponding tooth
- However, most of the teeth exhibit a conical shape
- They may be either erupted or impacted
Supernumerary Teeth Types:
- Mesiodens- Located between two upper central incisors
- Distomolars- Located on the distal aspect of the regular molar teeth
- Paramolars- They are located either in the buccal or the lingual aspect of the normal molars
- Extra lateral incisors- they are more common in the maxillary arch
Supernumerary Teeth Significance:
- Supernumerary Teeth may produce crowding or malocclusion
- They may cause cosmetic problems
- They may be directly or indirectly responsible for increased caries incidence and periodontal problems
- The dentigerous cyst may sometimes develop from an impacted supernumerary teeth
Supernumerary Teeth Treatment:
- They are mostly non-functional and they should be extracted
- Impacted supernumerary teeth should be removed surgically since they interfere with normal tooth alignment or can develop some pathology
Question 7. Dilaceration.
Answer:
Dilaceration
- Dilaceration refers to an angulation or sharp bend or curve anywhere along the root portion of the tooth
- Pathogenesis
- Trauma to partially calcified tooth germ may cause displacement of the hard calcified crown portion
- It may occur as a result of continued root formation during curved or tortuous path
- Idiopathic cause
Dilaceration Clinical Features:
- Dilaceration may involve both the dentition
- There is no sex predilection
- Dilaceration is observed at the coronal portion of the teeth
Dilaceration Treatment:
- Such teeth are extracted as they are prone to fracture
Question 8. Fordyce’s granules.
Answer:
Etiology:
- It is a developmental variation
- It is caused by an accumulation of sebaceous glands in the submucosal connective tissue
Fordyce’s Granules Features:
- Multiple, small, white to yellow nodules
- Usually located on the Buccal mucosa, occasionally on the labial mucosa
- Commonly bilateral
- It is a painless and persistent lesion
Fordyce’s Granules Treatment:
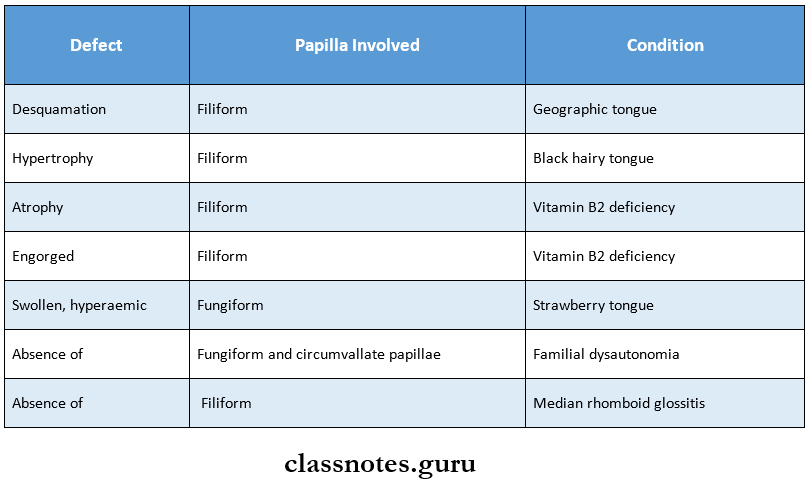
Question 9. Name papillae of the tongue.
Answer:
- Fungiform
- They are round in shape
- They are situated over the anterior surface of the tongue near the tip
- The number of taste buds in each is moderate
- Filiform
- They are small and conical in shape
- They are situated over the dorsum of the tongue
- They contain less number of taste buds
- Circumvalate papillae
- They are large structures present on the posterior part of the tongue
- They are many in number
- They are arranged in the shape of ‘V’
- They contain up to 100 tastebuds
Question 10. Natal teeth.
Answer:
Natal Teeth
- Natal Teeth are the teeth that are present at the time of birth
Etiology:
- Hereditary- superior position of the tooth bud
- Hormonal influence
Natal Teeth Clinical Features:
- Teeth may appear conical or may be normal in size and shape
- They may be opaque or yellow-brownish in color
- They are hypermobile
- Teeth appear to be attached to a small mass of soft tissue
- There may be a danger of aspiration of the teeth
- Riga fede ulcer- develops on the ventral surface of the tongue due to sharp edges of the incisors
- It leads to interference with the proper suckling and feeding activities
Natal Teeth Associated Syndromes:
- Ellis van Creveld syndrome
Natal Teeth Management:
- Extraction- to avoid interference with feeding activities
- Rounding of the sharp angles
- Retaining of the tooth- if it doesn’t create any problem
Question 11. Median rhomboid glossitis
Answer:
Median Rhomboid Glossitis
- Median Rhomboid Glossitis is an asymptomatic, elongated, erythematous patch of atrophic mucosa on the middorsal surface of the tongue
Median Rhomboid Glossitis Clinical Features:
- Age: it is seen in adults
- Sex: it is common in males
Median Rhomboid Glossitis Site:
- Anterior to the foramen cecum and circumvallate papillae
- In the midline on the dorsum of the tongue
- It starts as a narrow mildly erythematous area located along the median fissure of the tongue
- The lesion is asymptomatic
- It enlarges slowly often remaining unnoticed by the patient
- The fully developed lesion appears as a diamond or lozenge-shaped area devoid of the papilla
- The color of the lesion varies from pale pink to bright red
- There is the presence of a white halo
- The surface is usually smooth, flat or slightly raised
- It is sometimes fissured or lobulated
- The lesion exhibits an erythematous and nodular hyperplasia
- Some patients may develop similar lesions over the midline of the palate
- It may cause slight soreness or burning sensation
- It may regress spontaneously
Median Rhomboid Glossitis Management:
- Antifungal and antiseptic agents are used during irrita¬tion
Question 12. Etiology of median rhomboid glossitis.
Answer:
- Developmental
- Persistent tuberculum impar
- Fungal infection
- Candida albicans is many times found in the lesion
- Metabolic
- It is more common in diabetic patients than in nondiabetic patients
Question 13. Mesiodens.
Answer:
Mesiodens
- They are the most common type of supernumerary teeth
- Mesiodens is located between the two maxillary central incisors
Mesiodens Mode Of Formation:
- Mesiodens may develop either from an accessory tooth bud in the dental lamina
- Mesiodens may develop due to the splitting of regular normal tooth bud during the initial phase of odontogenesis
Mesiodens Clinical Features:
- Mesiodens can occur in both the sex
- Mesiodens may resemble the corresponding tooth
- However, most of the teeth exhibit a conical shape
- They may be either erupted or impacted
Mesiodens Significance:
- Mesiodens may produce crowding or malocclusion
- They may cause cosmetic problems
- They may be directly or indirectly responsible for increased caries incidence and periodontal problems
- The dentigerous cyst may sometimes develop from impacted supernumerary teeth
Mesiodens Treatment:
- They are mostly nonfunctional and they should be ex¬tracted
- Impacted supernumerary teeth should be removed surgically since they interfere with normal tooth alignment or can develop some pathology
Question 14. Black hairy tongue.
Answer:
Etiology:
- Formation of excess keratin causes elongation of the filiform papillae on the dorsal tongue
- May be infected with Candida albicans
Black Hairy Tongue Features:
- Elongation of the filiform papillae
- White to yellow in color
- Located on the posterior dorsal tongue
- Patients often have poor oral hygiene
- Patients may complain of bad taste
Black Hairy Tongue Treatment:
- Elimination of predisposing factors
- Cleaning the dorsal tongue with a soft toothbrush
- Treat Candidiasis if present
Question 15. Ankyloglossia.
Answer: Ankyloglossia
- Ankyloglossia is a result of a short, tight, thick, lingual frenulum
Ankyloglossia Classification:
- Based On The Anatomical Appearance
- Type 1: Frenulum attached to the tip of the tongue in front of the alveolar ridge in the low lip sulcus
- Type 2: Attaches 2-4 mm behind tongue tip and attaches on the alveolar ridge
- Type3: Attaches to mid-tongue and middle of the floor of the mouth, usually tighter and less elastic the tip of the tongue appears “heart-shaped”
- Type 4: Attaches against the base of the tongue, is shiny and very inelastic
- Based On The Distance Of The Insertion Of The Lingual Frenum To The Tip Of The Tongue
- Normal: 16 mm
- Class 1 [Mild]: 12-16 mm
- Class 2 [Moderate]: -12 mm
- Class 3[Severe]: 4- mm
- Class 4 [Complete]: 0-4 mm
Ankyloglossia Significance:
- In majority of the cases, it resolves spontaneously
- They are asymptomatic
- It may lead to
- Difficulty in breastfeeding, articulation problems
- Gingival recession
- Open bite
- Abnormal facial development
Ankyloglossia Treatment:
Question 16. Angular cheilitis
Answer:
Etiology:
- It occurs at the angle of the mouth among persons having deep commissural folds secondary to the overclosure of the mouth
- It can occur among persons with lip-licking habits, den¬ture wearing, or deficiency of riboflavin, vitamin Bn, and folic acid
Angular Cheilitis Clinical Features:
- The infection starts due to the colonization of fungi in the skin folds following the deposition of saliva due to re¬peated lip-licking
- Patients often have soreness, erythema, and Assuring at the corner of the mouth
- In some cases, it may extend over the adjacent skin sur¬faces
Question 17. Talon’s cusp.
Answer:
Talon’s Cusp
- Talon’s Cusp is an anomalous projection from the lingual aspect of the maxillary and mandibular permanent incisors
Talon’s Cusp Clinical Features:
- This anomalous cusp arises from the cingulum area of the tooth which extends to the incisal edge as a prominent T-shaped projection
- It is usually an asymptomatic condition
- In some cases, it may cause problems in esthetics
- It may be susceptible to caries
- It usually consists of normal-appearing enamel, dentin, and vital pulp tissue
- Occasionally lingual pits develop on either side of the talon’s cusp, where it join the lingual surface of the tooth
Talon’s Cusp Associated Syndrome:
- Rubinstein Taybi syndrome
Talon’s Cusp Treatment:
- Restorative measures are carried out to prevent caries
- When it interferes with occlusion, it is corrected with endodontic or restorative treatment
Question 18. Neonatal teeth.
Answer:
Neonatal Teeth
Neonatal Teeth are the teeth that are present within 30 days after the birth
Neonatal Teeth Etiology:
- Hereditary- superior position of the tooth bud
- Hormonal influence
Neonatal Teeth Clinical Features:
- Teeth may appear conical or may be normal in size and shape
- They may be opaque or yellow-brownish in color
- They are hypermobile
- Teeth appear to be attached to a small mass of soft tissue
- There may be a danger of aspiration of the teeth
- Riga fede ulcer- develops on the ventral surface of the tongue due to sharp edges of the incisors
- It leads to interference with the proper suckling and feeding activities
Neonatal Teeth Associated Syndromes:
- Ellis van Creveld syndrome
Neonatal Teeth Management:
- Extraction- to avoid interference with feeding activities
- Rounding of the sharp angles
- Retaining of the tooth- if it doesn’t create any problem
Question 19. Fissured Tongue.
Answer:
Fissured Tongue Synonyms:
- Scrotal tongue
- Lingua plicata
Fissured Tongue Etiology:
- Hereditary
- Aging
- Chronic trauma
- Vitamin deficiency
Fissured Tongue Features:
- It is seen in childhood
- It becomes prominent with age
- It exhibits multiple grooves or furrows of 2-6 mm depth
- It is of varied patterns on the dorsal surface
- Patients may rarely present with a burning sensation or soreness
- Food debris may get lodged into the furrows and cause irritation
Fissured Tongue Associated Syndromes:
- Melkersson-Rosenthal syndrome
- Down syndrome
Fissured Tongue Management:
- Advice the patient to use soft bristle brushes over the area
- To cleanse the fissures on a regular basis
Question 20. Actinic cheilitis.
Answer:
Actinic Cheilitis
Actinic Cheilitis is a pre-malignant squamous cell lesion resulting from long-term exposure to solar radiation
Actinic Cheilitis Clinical Features:
- Site: commonly occurs over the lower lip
- Age and sex: common in adult males
- Features:
- There may be redness and edema over the area
- The lips become dry and scaly
- Tiny bleeding spots are seen
- Gradually the scales become thick and horny
- Vertical Assuring and crusting occur
- There is a blurring of the margins
- Vesicles are formed which rupture to form superficial erosions
- Warty nodules may form There is the possibility of malignant transformation
Actinic Cheilitis Management:
- Topical fluorouracil
- Applied in 5% cone. For three times daily for 10 days
- CO2 snow: used to remove superficial lesions
- Vermillionectomy:
- Vermillion borders are excised
- Laser ablation- to vaporize Vermillion
- Electrodesiccation- it leads to dehydration by the insertion of electrodes into the tissues.
Oral Medicine Developmental Disorders Viva Voce
- Micrognathia of the maxilla is due to a deficiency in the pre-maxillary area
- Ankyloglossia causes difficulty in articulation of 1, r, t, d,n, th, sh, and z
- Ghost teeth are due to defects in mineralization
- Ghost teeth are seen in regional odontodysplasia
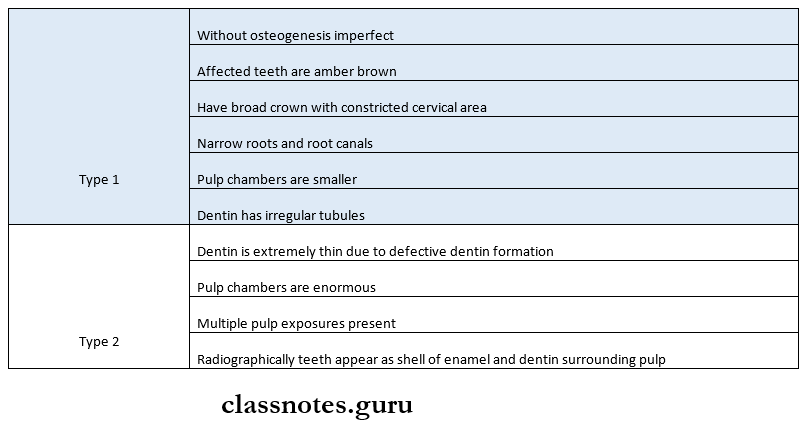
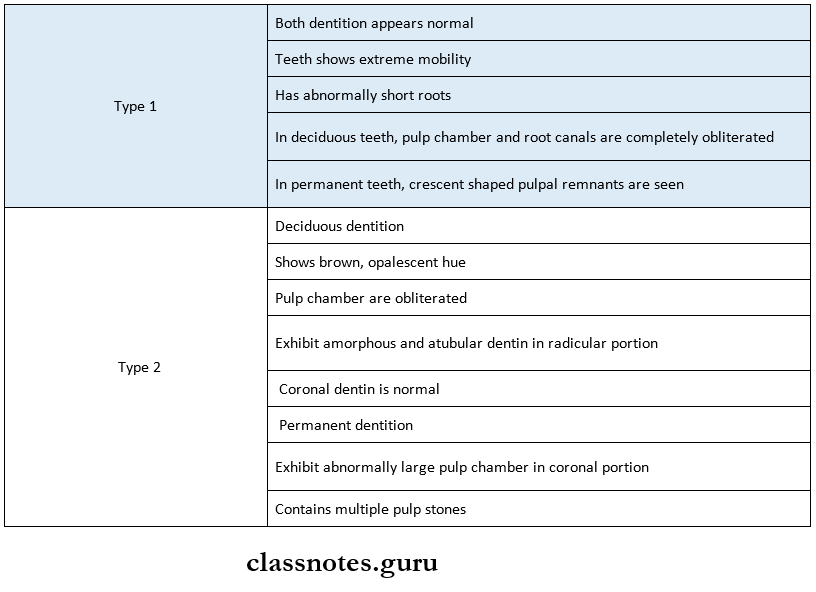
- Shell teeth are seen in dentinogenesis imperfect
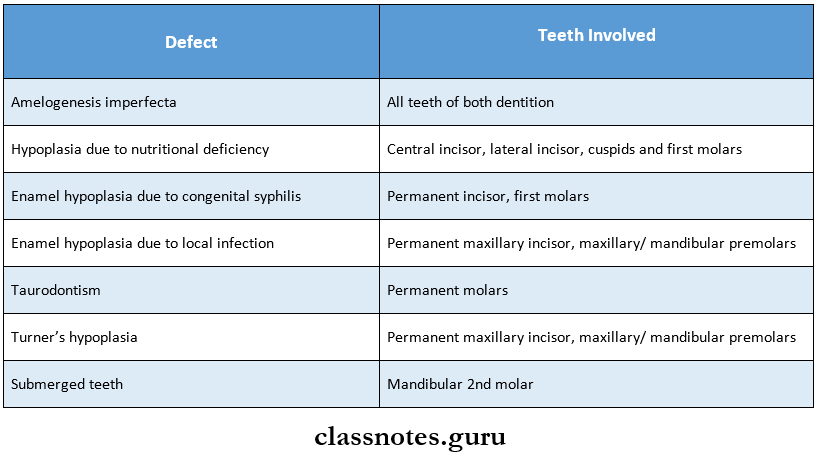
- Permanent molars are most commonly affected by taurodontism
- Torus mandibularis is commonly seen on the lingual surface of the mandible opposite to the premolar
- Mesiodens is the most common supernumerary teeth
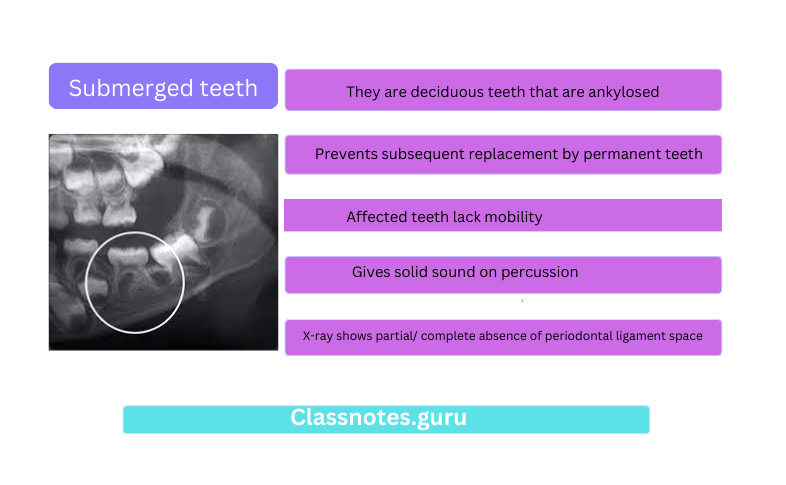
- Deciduous mandibular second molar is the most common ankylosed teeth
- Commonly missing teeth are
- Primary – maxillary and mandibular lateral inci¬sors
- Permanent – third molar
- Bohn’s nodules are seen at the junction of the hard and soft palate
- Epstein pearls are seen along the median raphe of the hard palate
- Dental lamina cysts of newborn are seen on alveolar ridges
- False anodontia is due to multiple extracted teeth
- Pseudo anodontia is due to multiple unerupted teeth
- Infusion patient will have one tooth less than normal
- In germination, the patient has one tooth extra of normal