
Oral Medicine Bone Disorders Important Notes
1. Fibrous Dysplasia:
- Fibrous Dysplasia Classification:
- Monostotic – Only one bone is involved
- Polyostotic – More than one bone is involved
- Jaffe’s type – Polyostotic along with cafe-au-lait-skin pigmentation
- Albright syndrome – is characterized by polyostotic fibrous dysplasia, cafe-au-lait skin pigmentation, and endocrine disturbances
2. Cleidocranial Dysplasia:
- It is characterized by abnormalities of the skull, shoulder girdle, jaws, and teeth
- Skull – delayed closure of sutures and wormian bones
- Shoulder – the partial or complete absence of clavicles
- Teeth – prolonged retention of deciduous and delayed eruption of permanent
- Numerous supernumerary teeth are found in the mandibular premolar and incisor areas.
3. Paget’s Disease:
- It is characterized by excessive and abnormal remodeling of bone
- Affects the adult skeleton
- Patients suffer from deafness, blindness, and facial paralysis
- There is a progressive enlargement of the skull and maxilla because of which the patient has to change the hats and dentures frequently
4. Cherubism:
- Manifests by the age of 3-4 years
- Painless symmetric swelling of the mandible or maxilla occurs
- Results in chubby face appearance
- The deciduous teeth shed prematurely and numerous teeth are absent
- X-ray shows numerous unerupted teeth floating in cyst-like spaces
Read And Learn More: Oral Medicine Question and Answers
5. Eagle’s Syndrome: Elongation Of Styloid Process Or Ossification Of Stylohyoid Ligament Leading To
- Dysphagia
- Sore throat
- Otalgia
- Glossodynia
6. Albright Syndrome:
- Precocious puberty
- Polyostotic fibrous dysplasia
- Cafe-au- lait pigmentation
7. Marfan’s Syndrome:
- Long thin extremities
- Hyperextensibility of joints
- Spidery fingers
- Arachnodactyly
- Bifid uvula
- CVS complications
8. Cafe-Au-Lait Pigmentation:
- It has brownish pigmentation
- Seen in
- Neurofibromatosis
- Fibrous dysplasia
- Peutzjeghers syndrome
- Hypothyroidism
9. Blue Sclera Is Seen In:
- Osteogenesis imperfect
- Marfan’s syndrome
- Cherubism
- Ehlers Danlos syndrome
- Osteopetrosis
- Fetal rickets
10. Ground Glass Appearance Is Seen In::
- Primary hyperparathyroidism
- Monostotic fibrous dysplasia
- Cherubism
11. Cotton Wool Appearance Is Seen In:
- Paget’s disease
- Chronic sclerosing diffuse osteomyelitis
- Fibrous dysplasia
- Cemento-osseous dysplasia
12. Hypermobility Of Joints Is Seen In:
- Ehler Danlos syndrome
- Marfan’s syndrome
- Osteogenesis imperfecta
- Down’s syndrome
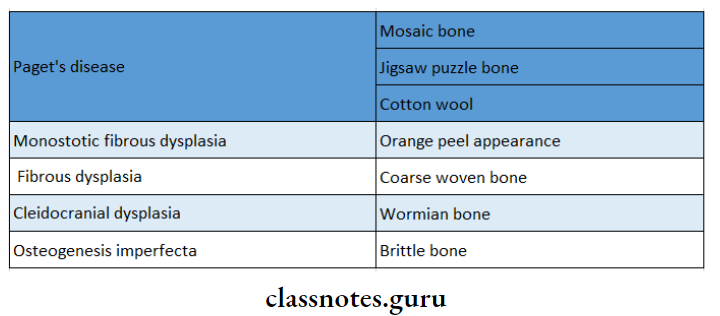
13. Radiographic Features In Different Diseases:
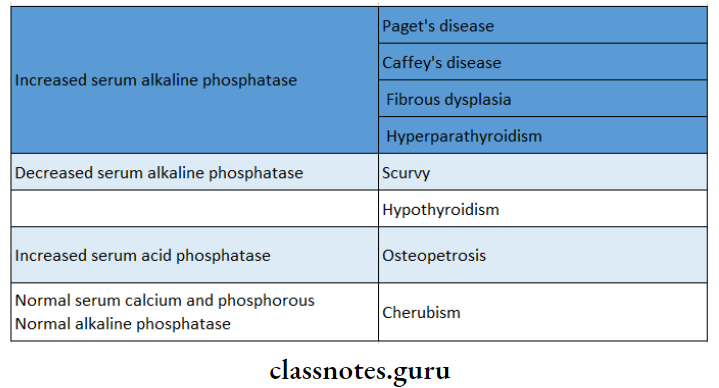
14. Laboratory Investigations
Oral Medicine Bone Disorders Short Essays
Question 1. Fibrous Dysplasia.
Answer:
Fibrous Dysplasia Definition:
Fibrous Dysplasia is an idiopathic condition, in which an area of normal bone is gradually replaced by abnormal fibrous connec¬tive tissue, which then again undergoes osseous metaplasia, and eventually, the bone is transformed into a dense lamellar bone.
Fibrous Dysplasia Classification:
- Monostotic – Only one bone is involved
- Polyostotic – More than one bone is involved
- Jaffe’s type: Polyostotic along with cafe-au-lait-skin pigmentation
- Albright syndrome: Characterized by polyostotic fibrous dysplasia, cafe-au-lait skin pigmentation, and endocrine disturbances
Etiology:
- Developmental – Developmental anomaly occurring during the growth period of life
- Endocrine disturbances – Complex endocrine disturbances
- Liver damage
- Infections
- Trauma
- Abnormal osteoclastic maturation of bone-forming – mesenchyme
Fibrous Dysplasia Clinical Features:
- Age – It commonly occurs in the first and second decade of life
- Sex – It commonly occurs in females
Fibrous Dysplasia Sites:
- Commonly affected sites are
- Skull
- Facial bones: Maxilla more affected than the mandible
- Clavicles
- Pelvic bones
- Long bones – femur, tibia, humerus
Fibrous Dysplasia Presentations:
- Skeletal Lesions
- Unilateral distribution of the lesion
- Swelling is seen on the affected side
- Recurrent bone pain is common
- There may be a cessation of growth but proliferation may occur
- Spontaneous fracture is a common complication
- Skin Lesion
- Cafe-au-lait pigmentation is seen
- It consists of irregularly, pigmented, light brown, flat, melanotic spots
- Oral Symptoms
- Slow enlarging, painless, unilateral swelling of the jaw
- This leads to facial deformity
- Expansion and distortion of the cortical plate
- Displacement of teeth
- Disturbances in tooth eruption
- Severe malocclusion
- Maxillary lesions
- They extend into the maxillary sinus and upto orbital floor leading to exophthalmos proptosis and nasal obstructions
- Mandibular lesions
- Protuberances in the premolar-molar area result in increased depth of the jaw
- Other – Precocious puberty leading to premature vaginal bleeding, breast development, and axillary and pubic hair at the age of 2-3 years.
Fibrous Dysplasia Radiographic Appearance:
- Radio Density – Unilocular or multilocular radiolucent lesion
- Borders – Ill-defined
- Lamina Dura – Loss of lamina dura
- Teeth – Resorption of roots occurs
- Jaw – Expansion and distortion of cortical plates
- Granular Appearance – Surrounding the margins of the radiolucent area, there may be a wider band of increased density, but granular in appearance
- Ground Glass Appearance – It may demonstrate areas of whorled amorphous partially calcified materials that are well-circumscribed
Fibrous Dysplasia Differential Diagnosis:
- Lesion And Their Distinguishing Feature:
- Traumatic bone cyst – Absence of cortical expansion
- Aneurysmal bone cyst – Hemorrhagic aspirate
- Chronic osteomyelitis – Occurs in older age
Fibrous Dysplasia Management:
- Surgical – Removal of lesion surgically
- Osseous contouring – for esthetic purpose
Question 2. Pathogenesis and management of Osteoradionecrosis.
Answer:
Pathophysiology:
- When small particles of high-energy radiation strike tumor cells or normal tissue cells, the cellular water undergoes radiolysis and is converted into free radicals
- These free radicals interact with the DNA of these cells and disrupt them
- This resultant DNA destruction is manifested differently at various levels
- On a cellular level, this is seen as a chromosomal break-age or disintegration
- The cell may then change like
- The cell may die
- It may repair its DNA to survive with impaired function
- It may repair DNA damage and function normally
- The tissues responsible for developing osteoradionecrosis are endothelium, bone, periosteum, and fibrous connective tissue of mucosa, and skin.
- At the tissue level, these radiation effects are seen as endothelial death, hyalinization, and thrombosis of the vessel
- Fibrosis of marrow spaces takes place
- At the organ level, it is seen as a composite tissue that is hypocellular, hypovascular, and hypoxic.
- This irradiated bone is thus unable to replace the nor¬mal cell loss with new cells and wound healing is thus severely compromised
- This creates a wound in which the demand for oxygen is much more than what can be provided
- Therefore there is tissue breakdown and it manifests as a chronic non-healing wound.
Management Of Osteoradionecrosis:
- The patient is made to breathe 100% oxygen via a pilot’s face mask
- The patient is exposed to 24 atmospheres of absolute pressure of chamber compression
- The oxygen exposure is for 90 minutes, once a day for 5 days a week
- Each exposure to hyperbaric oxygen (HBO) is called a dive
- Protocol
Stage 1 – 30 dives
↓
Condition improved
↓
The next 30 dives are given
↓
No improvement
↓
Stage 2 – Sequestrictomy
↓
Mucosal closure
↓
60 dives are given
↓
If the condition doesn’t improve
↓
Stage 3 – 30 dives
↓
Resection
↓
30 dives
↓
After 10 weeks
Additional 60 dives
are given
Oral Medicine Bone Disorders Short Answers
Question 1. Cherubism.
Answer:
Cherubism
Cherubism was first described by Jones in 1933
Cherubism Classification:
- Based on the severity and location of the lesion
- Grade 1 – Affects ramus of mandible
- This leads to bilateral and symmetrical expansion of bone
- Grade 2 – Affects ramus and body of mandible maxillary tuberosity
- Grade 3 – Affects maxilla and mandible entirely
- Grade 1 – Affects ramus of mandible
Etiology:
- Autosomal dominant trait
- Hormonal – latent hyperparathyroidism
- Trauma
- Disturbance in bone-forming mesenchyme
Cherubism Clinical Features:
- Age and sex – 2-3 years males are affected
- Site – Angle of mandible bilaterally
- Appearance
- Bilateral, painless, symmetrical swelling giving a chubby appearance
- Swelling is firm to hard on palpation
- Associated symptoms
- Maxillary swelling pressurizes the floor of the orbit
- This leads to an upward turn of the pupils of the eyes referred to “heavenward look”
- Difficulty in speech, deglutition, mastication, and respiration
- Limited jaw movement
- Expansion and widening of the alveolar ridge
- Flattening of palatal vault
- Chronic lymphadenopathy
- Malocclusion
- Syndrome Associated: Noonan syndrome
Cherubism Radiographic Features:
- Well-defined, well-corticated cyst-like radiolucency of the mandible
- Teeth appear as hanging in the air
- Displacement of the inferior alveolar canal
- Destruction of maxillary autrium
- Expansion of cortical plates
- Displacement of teeth
Question 2. Cleidocranial Dysplasia.
Answer:
Cleidocranial Dysplasia
Cleidocranial Dysplasia is a hereditary disorder characterized by abnormal growth of the bones in the face, skull, and clavicles with a tendency for the failure of tooth eruption
Cleidocranial Dysplasia Clinical Features:
- Absence or hypoplasia of one/both clavicles
- Hypermobility of shoulder joints
- Elongated frontal and occipital skull plates
- Underdeveloped entire midface
- Delayed closure of fontanelles
- High and narrow arched palate
- Underdeveloped paranasal sinuses
- Photophobia
- Multiple unerupted and impacted teeth
Radiographic Features – Radiograph Reveals:
- Open sutures
- Open fontanelles
- Partial/complete loss of clavicles
- Multiple impacted teeth
- Thin roots of teeth
Cleidocranial Dysplasia Treatment
- No treatment is possible
Question 3. Enumerate diseases with cafe-au-lait.
Answer:
Pigmentation:
- Albright syndrome
- Von Recklinghausen’s Neurofibromatosis
- Bloome’s syndrome
- Fanconi anemia
- Cowden’s syndrome
- Tuberculosis sclerosis
- Watson’s syndrome
- Ataxia telangiectasia
Oral Medicine Bone Disorders Viva Voce
- Paget’s disease shows the cotton wool appearance
- The development of osteosarcoma is the most serious complication of Paget’s disease
- Central giant cell granuloma commonly involves mandible
- Cherubism gives a floating tooth appearance
- Cherubism shows eye to heaven look appearance
- In osteopetrosis, there is endosteal production of bone
- Mosaic bone is due to partially resorbed and repaired bone
- Osteogenesis imperfecta is characterized by extreme fragility and porosity of bones