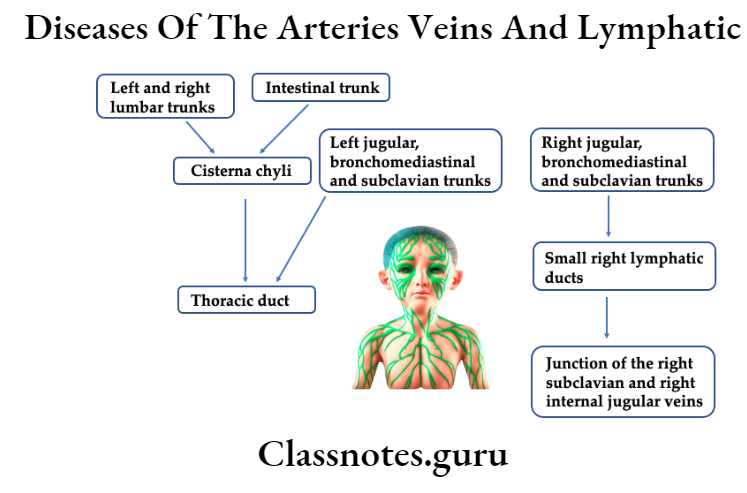
Diseases Of The Arteries Veins And Lymphatic System Short Answers
Question 1. Aneurysm of aorta.
Answer:
Aneurysm Of Aorta
Aneurysm Of Aorta is an abnormal enlargement of the wall of the aorta.
Aneurysm Of Aorta Types:
- Abdominal aortic aneurysm.
- Aneurysm occurs in the section of the aorta that runs through the abdomen.
- Thoracic aorta aneurysm.
- It is an aneurysm occurring in the chest area.
- Thoracoabdominal aortic aneurysm.
- Involves the aorta as it flows through both the abdomen and chest.
Aneurysm Of Aorta Features:
- Pain in the jaw, neck, upper back, or chest
- Coughing.
- Hoarseness of voice.
- Difficulty breathing.
- Pulsating enlargement.
Question 2. Mycotic aneurysm.
Answer:
Mycotic Aneurysm
- Mycotic aneurysm is an aneurysm arising from bacterial infection of the arterial wall.
- It is caused by streptococcus pneumonia.
Read And Learn More: General Surgery Question and Answers
Mycotic Aneurysm Symptoms:
- Fever
- Leucocytosis
- Palpable mass.
Question 3. Cricoid aneurysm/Aneurysmal bone cyst.
Answer:
Cricoid Aneurysm
Circoid aneurysm involves the bone anywhere in the body including the jaws.
Cricoid Aneurysm Clinical Features:
- Age – 10 – 19 years of age.
- Sex – occurs commonly in females.
- Rapid, enlarging, diffuse, firm swelling occurs.
- Swelling is painful.
- Perforation of cysts causes profuse bleeding.
- Paraesthesia.
Arterial diseases short notes
Question 4. Signs of Aneurysm.
Answer:
Signs Of Aneurysm
- Expansile pulsation in the course of the artery.
- Pulsation diminishes when pressure is applied
- Compressible swelling.
- The thrill is palpable over swelling
- Bruit is heard.
Question 5. Arteriography.
Answer:
Arteriography
- Arteriography is the most reliable method of determining the state of the main arterial tree.
- Arteriography gives information about.
- Size of the lumen of the artery.
- The course of the artery.
- Constriction and dilatation of arteries.
- Condition of collateral circulation.
Arteriography Methods:
- Retrograde percutaneous catheterization.
- Direct arterial puncture.
Question 6. Embolism.
Answer:
Embolism Definition: Embolism is the partial/complete obstruction of some part of the cardiovascular system by any mass carried in the circulation.
Embolism Types:
- Depending upon the matter in the emboli.
- Solid emboli.
- Liquid emboli.
- Gaseous emboli.
- Depending upon whether infected or not
- Sterile
- Septic.
- Depending upon the source of emboli.
- Cardiac
- Arterial
- Venous
- Lymphatic
- Depending upon the flow of blood.
- Paradoxical embolus.
- Retrograde embolus.
Venous disorders: short answers
Question 7. Pulmonary embolism.
Answer:
Pulmonary Embolism Definition: Pulmonary embolism is the most common and fatal form of venous thromboembolism in which there is occlusion of the pulmonary arterial tree by thrombotic emboli.
Pulmonary Embolism Etiology:
- Varicosities in superficial veins of legs.
Pulmonary Embolism Complication:
- Acute corpulmonale
- Chronic corpulmonale
- Pulmonary hypertension
- Pulmonary infarction.
- Pulmonary hemorrhage.
- Sudden death.
Question 8. Raynaud’s disease.
Answer:
Raynaud’s Disease Definition: It is a condition characterized by episodic attacks of vasospasm in response to cold exposure or emotional stimuli.
Raynaud’s Disease Phases:
- Intense pallor
- Cyanosis
- Rubor.
Raynaud’s Disease Etiology:
- Unknown etiology.
- Secondary to systemic diseases like
- Buerger’s disease.
Question 9. Subclavin steal syndrome.
Answer:
Subclavian Steal Syndrome
- Subclavian Steal Syndrome is a condition in which there is atherosclerotic stenosis of the subclavian artery proximal to the site of origin of the vertebral artery.
Subclavian Steal Syndrome Clinical features:
- Reduction in pressure in the subclavian beyond the stenosis.
- Retrograde blood flow
- Syncopal attack.
- Visual disturbances.
- Decreased pulse and blood pressure
- Localized bruit in the supraclavicular space.
Question 10. Trendelenburg’s test.
Answer:
Trendelenburg’s Test
- Trendelenburg’s test is used to determine the incompetency of the saphenofemoral valve.
- It can be performed in two ways.
- The patient is placed in a recumbent position.
- Legs are raised
- Sapheno-femoral junction is compressed with the thumb of the clinician and the patient is asked to stand up quickly.
- Pressure is released.
- If the varies fill very quickly, it indicates a positive Trendelenburg test.
- The patient is placed in a recumbent position.
- Legs are raised
- Sapheno-femoral junction is compressed and the patient is asked to stand up quickly.
- Pressure is maintained for 1 minute.
- Gradual filling of varices indicated positive Trendelenburg’s test.
Question 11. Commando’s operation.
Answer:
Commando’s Operation Indication: When carcinoma of tongue is fixed to the mandible
Commando’s Operation Steps:
- Hemiglossectomy.
- Hemimandibulectomy.
- Removal of floor of the mouth.
- Radical neck dissection.
Commando’s Operation Structure Removed:
- Fat, fascia, lymphatics.
- Lymph nodes – submental, submandibular deep cervical nodes, posterior group of nodes.
- Submandibular salivary gland.
- Sternomastoid.
- Internal jugular vein.
- Spinal accessory nerve.
Lymphatic system diseases Q&A
Question 12. Clinical staging of Hodgkin’s lymphoma.
Answer:
Clinical Staging of Hodgkin’s Lymphoma
Stage 1: Involvement of single lymph node.
Stage 2: Involvement of 2/ more lymph nodes on the same side of the diaphragm.
Stage 3: Involvement of 2/more lymph nodes on both sides of the diaphragm.
Stage 4: Diffuse involvement of extra-lymphoid organs with or without lymph node involvement.
Question 13. Histological classification of Hodgkin’s lymphoma.
Answer:
Histologica Classification of Hodgkin’s Lymphoma
- Type 1 – Lymphocyte predominant type.
- Reed Sternberg (RS) cells are scanty; scattered among large number of matured lymphocytes.
- Type 2 – mixed cellularity.
- There is significant number of eosinophils, neutrophils, plasma cells, and atypical histio- cytesalongwith. RS cells and lymphocytes.
- Type 3 – Nodular sclerosis.
- Presence of broad collagen bands separating the lymphoid tissue.
- Type 4 – lymphocyte depletion.
- Lymphocytes are few
- Presence of malignant appearing histiocytes.
Question 14. Non-Hodgkin’s lymphoma.
Answer:
Non-Hodgkin’s lymphoma
Non-Hodgkin’s lymphoma is a group of primary malignancies of lymph-reticular tissue.
Non-Hodgkin’s Lymphoma Classification:
- Histological.
- Lymphocyte predominant
- Mixed cellularity
- Nodular sclerosis.
- Lymphocyte depletion.
- Based on the prognosis.
- Nodular – favorable prognosis.
- Diffuse-unfavorable prognosis.
Non-Hodgkin’s Lymphoma Clinical features:
- Extranodal involvement.
- Fever with night sweats
- Weight loss
- Local invasion of adjacent structures
- Regional lymphadenopathy.
Non-Hodgkin’s Lymphoma Management:
- Staging laparotomy is required
- Splenectomy.
Question 14. Lymphadenitis.
Answer:
Lymphadenitis
Lymphadenitis is the inflammation of lymph nodes.
Lymphadenitis Clinical features:
- The site involved – lymph nodes under the neck, in the axilla, or in the groin.
- Lymph nodes are enlarged.
- Firm, painful enlargement occurs
- Hyperaemic overlying skin.
- Fever
Lymphadenitis Treatment:
- Analgesic
- Antibiotic
- Abscess drainage.
Question 15. Lymphosarcoma.
Answer:
Lymphosarcoma Definition: It is defined as a malignant neoplastic disorder of the lymphoid tissue characterized by the proliferation of atypical lymphocytes and their localization. In various parts of the body.
Lymphosarcoma Clinical Features:
- Age – common in children.
- Lymph nodes involved – in the neck, mediastinum, and abdomen.
- Extra-nodal involvement – spleen, tonsil, pharynx, bowel.
- Enlargement of lymph nodes.
- Constitutional symptoms – fever, loss of weight, anemia, anorexia, weakness.
- The overlying skin is shiny and tense
- The surface is irregular.
Lymphosarcoma Treatment:
- Radiotherapy.
- Chemotherapy – in case of diffuse involvement.
Common diseases of arteries and veins
Question 16. Microscopic appearance of tuberculous lymphadenitis.
Answer:
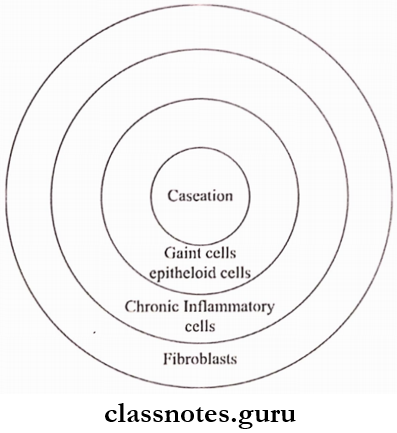
Microscopic Appearance Of Tuberculous Lymphadenitis
- Tubercles are seen consisting of epithelial cells and giant cells with peripherally arranged nuclei.
- Next lymphocytes with darkly stained nuclei and scanty cytoplasm appear.
- As the disease progresses caseation necrosis occurs.
- Thus, in the center of the follicle caseation occurs
- This is surrounded by giant cells, epitheloid cells, zone of chronic inflammatory cells, and fibroblasts.
Question 17. Malignant secondary lymph node.
Answer:
Malignant Secondary Lymph Node
Can occur commonly from malignant melanoma.
Malignant Secondary Lymph Node Clinical Features:
- Site
- Painless swelling
- Constitutional symptoms – anorexia, weight loss, weakness.
- Lymph nodes are irregular, and discrete.
- They fuse to form a large mass.
- Nodes are usually hard.
- Gradually they gets fixed to the surrounding structures.
Question 18. Use of MRI ion head and neck.
Answer:
Use Of MRI Ion Head And Neck
- For the study of TMJ deformities in the sagittal plane.
- To evaluate various spaces in the head and neck region.
- For nasopharynx, skull base, tongue pathology.
- Posturgical evaluation of TMJ.
- To identify and localize orofacial soft tissue lesions.
- Provides an image of salivary gland parenchyma.
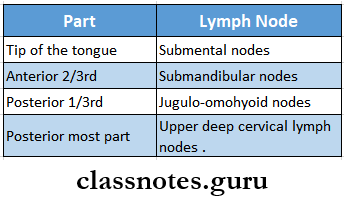
Question 19. Lymphatic drainage of the tongue.
Answer:
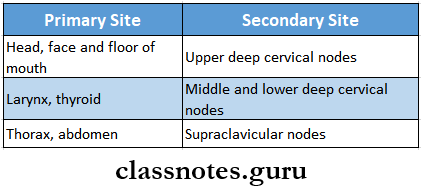
Lymphatic Drainage Of The Tongue
Vascular system disorders short answer questions
Question 20. Waldeye’s ring.
Answer:
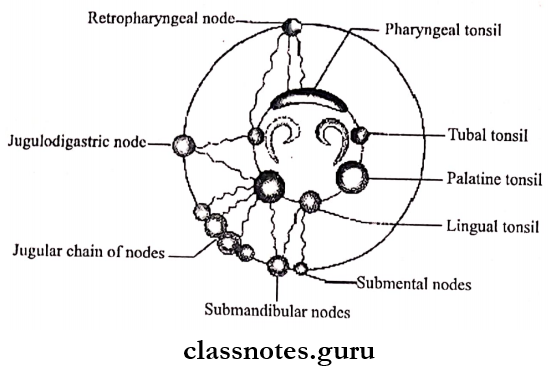
Waldeyer’s Ring Consists Of
- Pharyngeal tonsil-posteriorly and above
- Tubal tonsil – laterally and above
- Lingual tonsil – Inferiorly.
- Submandibular nodes
- Retropharyngeal nodes
- Submental nodes
- Jugulodigastric nodes
- Jugular chains of nodes.
- Retropharyngeal node
- Tubal tonsil Palatine tonsil Lingual tonsil
- Jugular chain of nodes
Question 21. Causes of wet gangrene
Answer:
Causes Of Wet Gangrene
- Gangrene from acute inflammation
- Long-standing venous thrombosis
- Bed sores
- Gas gangrene
Peripheral artery disease short answer
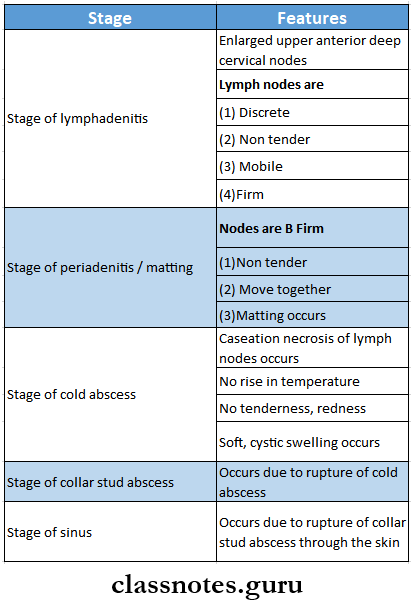
Question 22. Stages of tubercular lymphadenitis
Answer:
Stages Of Tubercular Lymphadenitis