
Fractures General Principles Important Notes
- Fracture – It Is Loss Of Continuity Of Bone
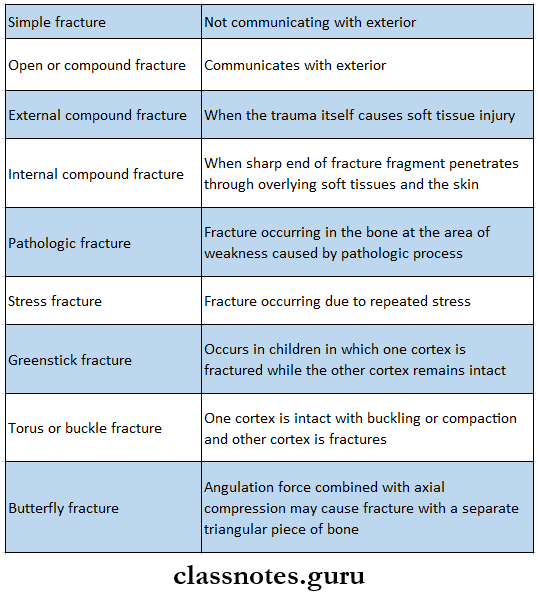
- Types Of Fractures
- Stages Of Healing Of Fracture
- Stage of hematoma formation
- Stage of cellular proliferation
- Stage of callus formation
- Stage of new bone formation
- Stage of remodeling
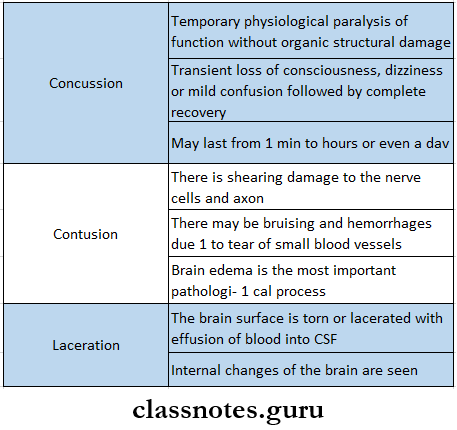
- Brain Injuries
- Sequele Of Contusion And Laceration
- Post traumatic amnesia
- Cerebral irritation
- Post contusional syndrome
- Traumatic epilepsy of Jacksonian type
- Cerebral compression
- Lucid Interval
- In the case of extradural hemorrhage when the hematoma has reached a considerable size it causes a sufficient rise in intracranial pressure to cause cerebral compression
- This causes unconsciousness due to pressure on the reticular system of the midbrain
- The time taken to form such a big hematoma is known as a lucid interval
- Complications Of Head Injury
- Early complication
- Leakage of CSF
- Aerocele
- Meningitis
- Fat embolism
- Brain stem injury
- Posterior fossa injury
- Pituitary failure
- Late complication
- Chronic subdural hematoma
- Post-traumatic epilepsy
- Headache
- Hydrocephalus
- Early complication
Read And Learn More: General Surgery Question and Answers
Fractures General Principles Short Answers
Question 1. Clicking jaw
Answer:
Clicking Jaw Causes:
- Normal jaw mechanics
- Temporomandibular joint disorders
- Masticatory muscles disorders
- Maxillo-mandibular alignment disorder
- Occlusal discrepancies
- Bruxism
Types of fractures questions and answers
Question 2. Black eye
Answer:
Black Eye
- Feature of Lefort 2 fracture
Black Eye Appearance:
- Presence of bilateral circumorbital edema
- Presence of bilateral circumorbital ecchymosis
Black Eye Diagnosis:
- Difficult due to rapid development of swelling of eyelids
Question 3. Lefort I fracture
Answer:
Lefort I Clinical Features:
- Oedema of lower part of face
- Ecchymosis in buccal vestibule
- Bilateral epitaxis
- Mobility of upper teeth
- Disturbed occlusion
- Pain
- Upward displacement of fragment- telescopic fracture
- ‘Cracked cup’ sound on percussion of upper teeth
- ‘Guerin sign’- ecchymosis in the greater palatine region
Lefort I Management:
- Reduction
- Reduction of the impacted fragment with the help of disimpaction forceps (Rowe’s and William’s forceps)
- Placement of Rowe’s forceps:
- The straight blade is placed into the nostrils
- The curved blade is placed over the palate
- Placement of William’s forceps:
- Placed over the buccal aspect
- Displaces maxilla in mesiodistal direction
- Fixation:
- Zygomatic suspension fixation is done
- Holes are drill over the zygomatic arch
- Pass wire through it
- Bring it up to the arches
- Twisted over are arch bars
- 3.Inter Maxillary Fixation
- IMF done for 3-4 weeks
Question 4. Extradural hematoma
Answer:
Extradural Hematoma
- Extradural Hematoma is the hemorrhage in the space outside the dura mater but inside the skull
Extradural Hematoma Causes:
- Injury to the main trunk of the middle meningeal artery
- Injury to middle meningeal vein
- Bleeding in the posterior cranial fossa
- Fractures of the anterior fossa
- Bleeding from one of the venous sinuses
Extradural Hematoma Clinical Features:
- Bleeding in the epidural spaces
- They can quickly expand and compress the brain stem
- Unconsciousness
- Abnormal posture
- Abnormal pupil responses to light
Extradural Hematoma Treatment:
- Blood may be aspirated surgically to remove the mass and reduce the pressure on the brain
- Hematoma is evacuated through a burr hole or craniotomy
Bone fracture types Q&A
Question 5. Subdural hematoma
Answer:
Subdural Hematoma
- Subdural hematoma is a type of hematoma in which blood gathers within the outermost meningeal layer between the duranater which adheres to the skull and the arachnoid mater enveloping the brain
Subdural Hematoma Causes:
- Laceration of the cortex
- Rupture of superior cerebral veins
Subdural Hematoma Clinical Features:
- Severe brain damage
- No definite lucid interval
- Early unconsciousness
- Cerebral compression
- When subdural hematoma is less dramatic and delayed by several days, it is called subacute subdural hematoma
- When subdural hematoma appears further late, it is called chronic subdural hematoma
Subdural Hematoma Treatment:
- Extensive craniotomy
- Hemorrhagic vessels are secured and ligated
- Hematomas are cleared off
- Subdural Hematoma
Question 6. Temporomandibular Dislocation
Answer:
Temporomandibular Dislocation
- Dislocation refers to the condition in which the condyle is placed anterior to the articular eminence with collapse of the articular space
Temporomandibular Dislocation Clinical Features:
- Pain
- Inability to close the mouth
- Tense masticatory muscles
- Difficulty in speech
- Excessive salivation
- Open bite
- Protuding chin
- Deviation of the lower jaw
Question 7. An immediate complication of fracture
Answer:
An Immediate Complication Of Fracture
- Anesthesia
- Anesthesia of lower lip occurs in case of neuropraxia, axonometric or, neurotmesis
- Malunion
- Improper alignment of the fracture ends leads to malunion
- Infection
- It may be initiated as a localized abscess but later progresses to osteomyelitis
- Superior orbital fissure syndrome
- Hematoma within the fissure causes damage to the 3rd, 4th and 6th cranial nerves
- Nonunion
- It is a lack of bony fusion of the fractured ends
- Delayed union
- If the fracture does not heal in 4-6 weeks, it is called delayed healing
- It is a temporary condition and can be corrected
- Derangement of occlusion
- If there is traumatic occlusion it is corrected by selective grinding of teeth
- Ankylosis of TMJ
- Prolonged immobilization causes ankylosis
- Other complications
- Diplopia
- Enophthalmos
- Blockade of nares
- Anosmia
- epiphora
Short questions on fractures
Question 8. Head injury management
Answer:
Head Injury Management
- Management of the head injury depends on the Glasgow Coma Scale
- A less than 8 score- indicates severe injury
- Score 9-12- moderate injury
- Score 13-15- mild injury
- Measures include
- Examination of the wound
- Continued ventilation
- Intensive care unit management of intracranial pressure
- Oxygenation
- Frequent neurological examination
- CT scan
Question 9. Artificial Respiration
Answer:
Artificial Respiration
- Artificial respiration is required whenever there is arrest of breathing which occurs during
- Accidents
- Drowning
- Asphyxia
- Gas poisoning
Artificial Respiration Purpose:
- Ventilation of alveoli
- Stimulation of respiratory centers
Artificial Respiration Methods:
- Manual method
- Mouth to mouth method
- Holger Neilson method
- Mechanical methods
- Drinker’s method
- Ventilation method
Fracture classification Q&A
Question 10. Cardiopulmonary resuscitation
Answer:
Cardiopulmonary Resuscitation
- Cardiopulmonary resuscitation is done by external cardiac compression which is a rhythmic application of pressure over the lower half of the sternum
Cardiopulmonary Resuscitation Steps:
- Position yourself in kneeling position on the side of the patient
- Place the heel of one hand on the position of pressure
- Place the heel of other hand on top of first one and interlock the fingers
- Apply pressure to depress the sternum at least 11/2 – 2 inches
- The rate of compression should be 60 per min.
- Apply 15 compressions on the chest followed by 2 full ventilation
- Repeated to form 4 complete cycles in a minute
Cardiopulmonary Resuscitation Effects:
- Pressure in the thorax increases
- Thorax causes the blood from the periphery to flow back into the heart and refill the chambers
- This increases cardiac output
Question 11. Malunion
Answer:
Malunion
- Improper alignment of the fractured ends leads to malunion
- Usually it does not require any treatment
- But if it affects patient’s occlusion, function, and esthetics it should be treated
Malunion Treatment:
- Osteotomy of fragment segments
- Realignment
- Fixation
- Use of elastics to correct malocclusion
Question 12. Depressed fractured skull
Answer:
Depressed Fractured Skull
- Depressed fractured skull can be of two types
- Open
- Closed
- Depressed Fractured Skull may lead to
- Dural tear
- Pressure on the cerebral cortex
- Underlying hemorrhage
- Epilepsy
- Pressure on dural venous sinuses
Depressed Fractured Skull Treatment:
- Shaving of the head
- Detect neurological deficit
- Debridement of the scalp
- A burr hole is made by the side of the fractured portion
- Through it an elevator is introduced and the underlying dura is gently separated
- The depressed fragments are lifted up and dura is inspected
Fracture types viva questions
Question 13. Cerebral concussion
Answer:
Cerebral Concussion
- Cerebral Concussion is a type of brain injury
Cerebral Concussion Features
- Temporary physiological paralysis of function without organic structural damage
- Transient loss of consciousness, dizziness, or mild confusion followed by complete recovery
- May last from 1 min to hours or even a day
Question 14. causes of nasal bleeding
Answer:
causes Of Nasal Bleeding
- Trauma
- Exposure to warm, dry air for long time
- Nasal and sinus infection n Allergic rhinitis
- Nasal foreign body
- Vigorous nose blowing
- Deviated nasal septum
- Cocaine use
- Use of anti-coagulant
- Hypertension
- Bleeding disorders
Important questions on bone fractures
Fractures General Principles Viva Voce
- The mass of new bone formation at the site of fracture is known as a callus
- Crepitus is a sensation of grating which may be felt or heard
- Perkin’s formula helps to estimate the time required for union of fracture and consolidation
- If time taken for union for fracture is unduly prolonged it is called a delayed union
- When bony union cannot takes place naturally without operation it is called non-union
- Meningitis is very common complication of skull fractures
- Post-traumatic amnesia is loss of memory for events after the occurrence of trauma
- Retrograde traumatic amnesia means loss of memory for events before the occurrence of the accidents