
Retention And Relapse Definition
- Retention
- Maintaining newly moved teeth in position, long enough to aid in stabilizing their correction.
- Relapse
- It is the loss of any correction achieved by orthodontic treatment.
Retention And Relapse Important Notes
Types of retention:
- Limited retention:
- Class 1 non-extraction
- Deep bites
- Class 1, Class 2 Div. 1 and Div. 2 extraction
- Natural retention:
- Anterior cross bites
- Serial extraction
- Highly placed canines
- Posterior crossbite
- Permanent retention:
- Midline diastemas
- Rotation
- Class 2 div.2 deep bites
- Abnormal musculature
- Cleft palate patients
Types of retainers:
- Removable:
- Hawely’s appliance
- Begg retainers
- Clip on retainers
- Wrap-around
- Kesling tooth position
- Invisible retainers
- Fixed:
- Fixed appliance
- Banded canine to canine
- Bonded lingual
- Band and spur retainer
Read And Learn More: Orthodontics Short And Long Essay Question And Answers
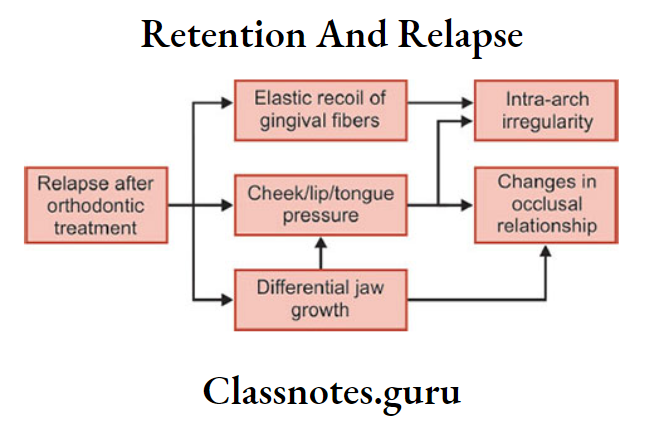
Causes of relapse:
- Periodontal ligament traction
- Growth related changes
- Bone adaptation
- Muscular forces
- Failure to eliminate the original cause
- Role of the third molar
- Role of occlusion
Retention And Relapse Long Essays
Question 1. Enumerate theories of retention. Add a note on causes of relapse.
Answer.
Retention
Definition of retention: By Moyers
- Maintaining newly moved teeth in position, long enough to aid in stabilizing their correction.
Theorems: 9 theorems by Riedel and 10th Moyers
- Moved teeth return to their former position
- Elimination of cause prevents relapse
- Malocclusion should be over-corrected
- Proper occlusion should be achieved
- Bone and adjacent tissues should be provided time to readapt around moved teeth
- Lower incisors must be placed upright
- Corrections carried out during growth periods are less likely to relapse
- Farther the teeth have been moved, the lesser the risk of relapse
- Arch form, particularly mandibular, cannot be permanently altered by appliance therapy
- Many treated malocclusions require permanent retaining devices
Types of retention
Limited retention:
- Class 1 non-extraction
- Deep bites
- Class 1, Class 2 Div. 1 and Div. 2 extraction
Natural retention:
- Anterior crossbite
- Serial extraction
- Highly placed canines
- Posterior crossbite
Permanent retention:
- Midline diastema
- Rotation
- Class 2 div.2 deep bites
- Abnormal musculature
- Cleft palate patients
Retainers: Passive appliances that help in maintaining and stabilizing the position of teeth long enough to permit readaptation of supporting structures
Types of retainers
- Removable retainers
- Hawely’s appliance
- Begg retainer
- Clip on retainer
- Wrap-around
- Kesling tooth position
- Invisible retainer
- Fixed retainers
- Fixed appliance
- Banded canine to canine
- Bonded lingual
- Band and spur retainer
Relapse: It is the loss of any correction achieved by orthodontic treatment
Causes of Relapse:
- Periodontal ligament traction:
- Due to orthodontic tooth movement, PDL and gingival fibres are stretched
- They readapt to the newly moved teeth
- Different fibres require different periods for it
- Principle fibres – 4 weeks
- Gingival fibres – 40 weeks
- If not provided sufficient time, leads to relapse
- Growth-related changes:
- Due to the continuation of abnormal growth pattern
- Bone adaptation:
- Normal, bony trabeculae are arranged perpendicular to the long axis of teeth
- During orthodontic treatment, arranged parallel to the long axis of teeth
- After treatment returns to original position
- Muscular forces:
- Abnormal muscle balance
- Failure to eliminate the original cause:
- The cause should be properly diagnosed and a treatment plan must be done accordingly
- Role of the third molar:
- Eruption time – 18-21 years i.e. usually after completion of orthodontic treatment
- Produces pressure
- Results in crowding recurrence
- Role of occlusion:
- Failure to eliminate habits like bruxism
- Failure to achieve centric occlusion
Retention And Relapse Short Essays
Question 1. Define retention, and explain schools of retention.
Answer.
Retention: Maintaining newly moved teeth in position long enough to aid in stabilizing their correction – By Moyers
Schools Of Retention:
- Occlusion School – By Kingsley
- Proper occlusion is important as it safeguards the stability in the new position of patients
- Apical base school:
- By Alex Lundstorm, Mc.Cauley and Nance
- By Alex Lundstorm – Suggest apical base as an important factor in the correction of malocclusions
- Mc. Cauley – Added inter-canine and intermolar width should be maintained
- Nance – Noted arch length cannot be permanently increased to a major extent.
- By Alex Lundstorm, Mc.Cauley and Nance
- Mandibular Incisor School – Grieves and Tweed
- Stability increases if mandibular incisors are placed upright
- Musculature School – Rojer
- Functional muscle is necessary for post-treatment stability.
Question 2. Permanent retention.
Answer.
Conditions of Permanent Retention:
- Midline diastema
- Severe rotations
- Generalized spacing
- Patients with abnormal musculature
- Arch expansion
- Cleft palate patients
- Class 2 div.2 deep bite
Appliances Used:
Retainers: Passive appliances that help in maintaining and stabilizing the position of teeth long enough to permit readaptation of supporting structures
Types of Retainers:
Removable Retainers
Removed and reinserted at patient’s will
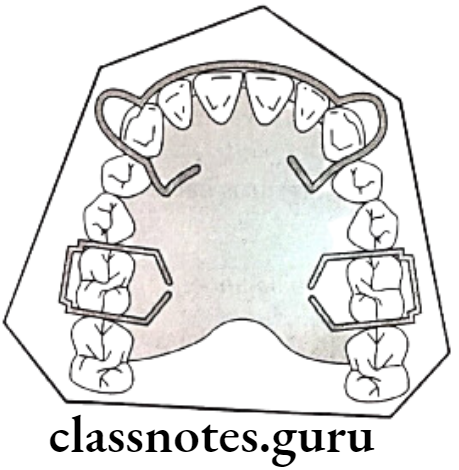
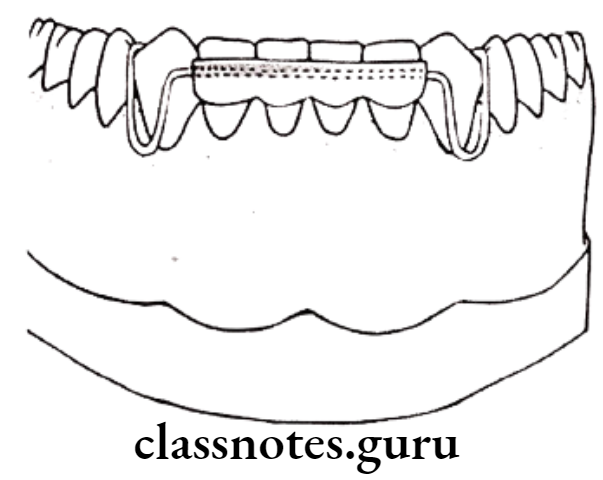
- Hawely’s Appliance – By Charles Hawley
- Consists of – short labial bow, Adam’s clasps on molars
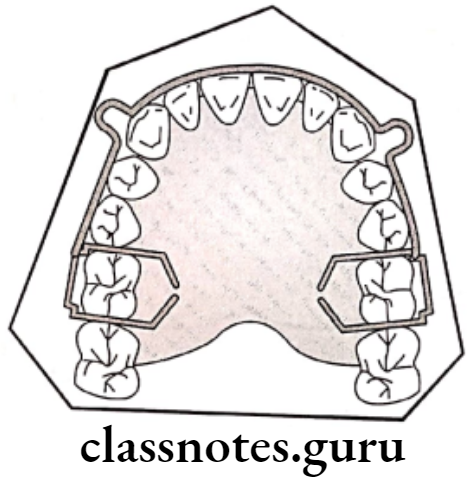
Modifications of Hawely’s appliance:
- Long labial bow – for space closure distal to the canine
- Fitted labial bow – Excellent retention
- Soldered labial bow
- Anterior bite plane – for deep bite
Advantages of Hawley’s appliance:
- Simple and easy to fabricate
- Comfortable to patient
- Acceptable
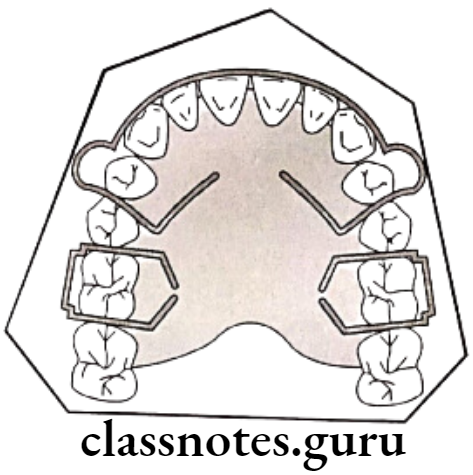
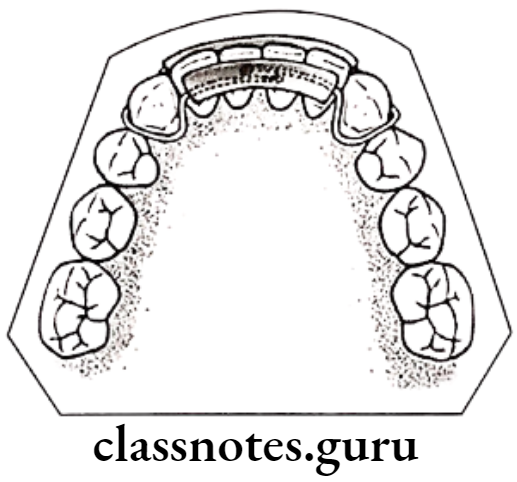
Begg retainer – By P.R. Begg
Consists Of Begg retainer:
- Labial wire till last erupted molar, curves around it
- Spans palate – Acrylic portion
Advantage of Begg retainer: Eliminate risk of spacing between canine and premolar
Clip on retainer:
- Labial wire covering incisors and canine then wrapped around same teeth lingually
Wrap around retainer:
- Wire wrapped around all erupted teeth labially as well as lingually
Keeping tooth position – By H.D. Kesling
- Thermoplastic rubber covering the clinical crown of upper and lower teeth
- This leads to difficulty in speech and TMJ problems
Invisible retainers: Covers clinical crowns and part of the gingiva on a transparent thermoplastic sheet
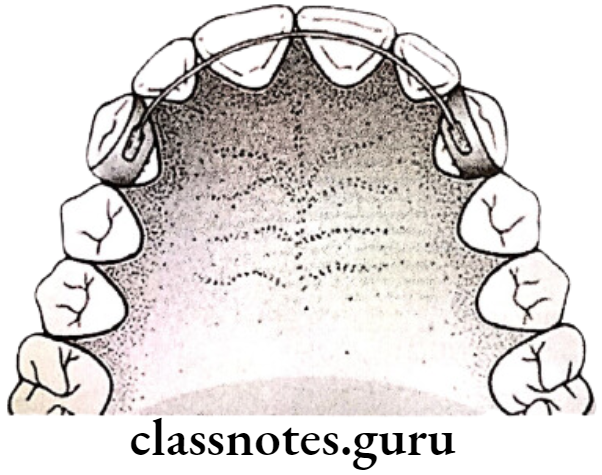
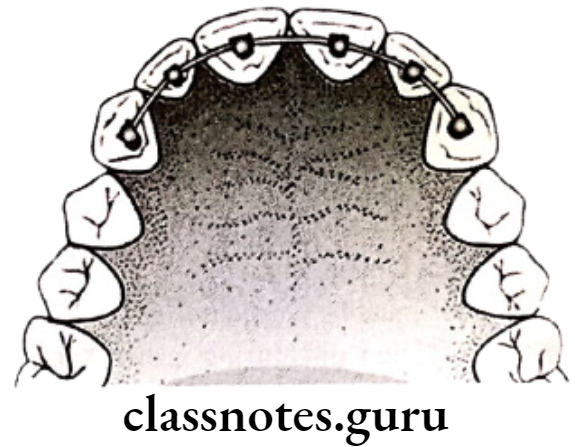
Fixed retainers
- Fixed appliance itself
- Banded canine-to-canine retainer
- Thicker wire over lingual surface soldered on canine bands
- Bonded lingual retainers
- Stainless steel/Etglioy wire is etched and bonded lingually over interiors
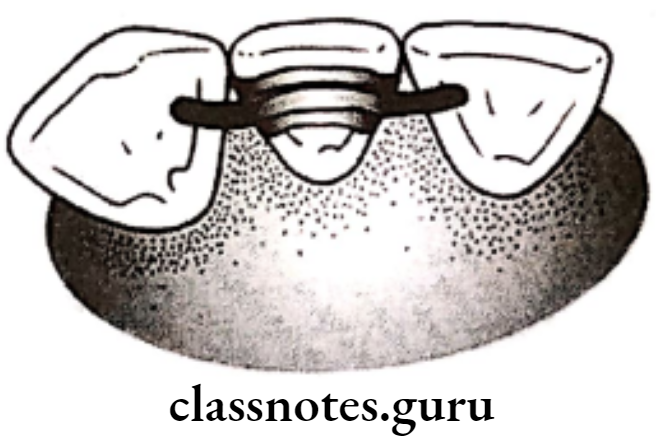
- Band and spur
- For rotation
- The moved tooth is bands and spur are soldered over it.
Retention And Relapse Short Questions And Answers
Question 1. Define retention.
Answer.
By Moyers
- Maintaining newly moved teeth in position, long enough to aid in stabilizing their correction
Question 2. Define relapse.
Answer.
- It is the loss of any correction achieved by orthodontic treatment
Question 3. Causes of relapse.
Answer.
- Periodontal ligament traction
- Due to orthodontic tooth movement, PDL and gingival fibres are stretched
- They readapt to the newly moved teeth
- Different fibres require different periods for it
- Principle fibres – 4 weeks
- Gingival fibres – 40 weeks
- If not provided sufficient time, leads to relapse
Growth-related changes:
- Due to the continuation of abnormal growth pattern
Bone adaptation:
- Normal, bony trabeculae are arranged perpendicular to the long axis of teeth
- During orthodontic treatment, arranged parallel to the long axis of teeth
- After treatment returns to the original position
Muscular forces:
- Abnormal muscle balance
Failure to eliminate the original cause:
- The cause should be properly diagnosed and a treatment plan must be done accordingly
Role of the third molar:
- Eruption time – 18-21 years i.e. usually after completion of orthodontic treatment
- Procedures pressure
- Results in crowding recurrence
Role of occlusion:
- Failure to eliminate habits like bruxism
- Failure to achieve centric occlusion
Question 4. Conditions where retention is not required/Natural retention.
Answer.
- Anterior crossbite
- Serial extraction
- Highly placed canines
- Posterior crossbite
Question 5. Permanent retention.
Answer.
- Midline diastema
- Rotation
- Class 2 div.2 deep bites
- Abnormal musculature
- Left palate patients
Retention And Relapse Viva Voce
- According to Alex Lundstorm, the apical base is the key to retention
- According to Grieves and Tweed, mandibular incisors are a key factor in retention
- Full-time retention after comprehensive orthodontic therapy is needed for 4-5 months
- Upper anterior crossbite correction with no adequate overbite requires retention of 3-6 months
- Opening of premolar space is a drawback of standard Hawley retainer
- Prevention of wedging effect on extraction site by Hawley retainer can be attempted by long labial bow
- Relapse is the loss of any correction achieved by orthodontic treatment