
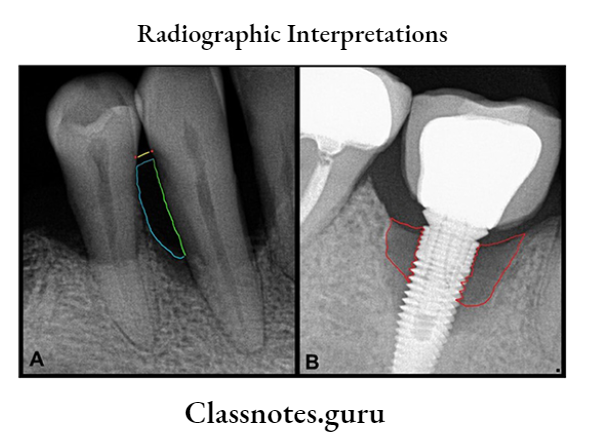
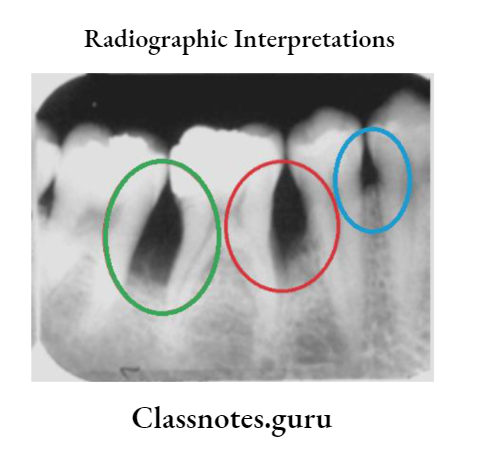
Radiographic Interpretations
Important Notes
- Some of the radiographic appearances in various pathology
- Central giant cell granuloma:
- It is a reactive process, but not a neoplasm.
- Soap bubble or honeycomb appearance
- A characteristic feature is that the septa are perpendicular to the periphery of the lesion and notching is seen corresponding to the outline where the septa arise.
- Central hemangioma:
- Soap bubble appearance
- Swelling of jaws, and gingival bleeding through the sulcus are seen.
- “Pumping action” is a characteristic clinical feature. If the tooth in the region of the tumor is pushed into the tumor, it will rebound back to the original.
- Aneurysmal bone cyst:
- H/O of trauma, the cyst is a reactive process secondary to trauma
- Honeycomb and soap bubble appearance
- Frank’s blood on aspiration
- Pseudocyst
- Multinucleated giant cells are seen histologically
- Cherubism:
- Seen at 2 – 6 years of age with familiar history
- When the maxilla is involved, the skin over it is stretched with the pulling of skin below the eyes. The sclera is visible giving an “angelic look” or “eyes towards heaven”.
- Multiple unerupted teeth are seen which appear to be floating in cyst-like spaces.
- Lesions arising from clinically missing or radiologically missing teeth:
- Eruption cyst
- Dentigerous cyst
- Gorlin cyst
- Unicystic or mural ameloblastoma
- Adenoamelobastoma
- Ameloblastic fibroma
- Variants of ameloblastoma
- Ameloblastic Odontoma
- Ameloblastic Odontofibroma
- Ameloblastic dentinoma
- Ameloblastic dentinofibroma
- Primordial cyst
- Teratoma
Radiographic interpretation in dentistry
Radiographic Interpretations Long Essays
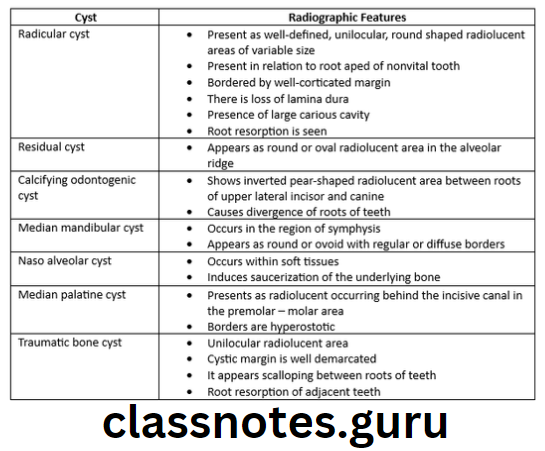
Question 1. Describe the radiographic appearance of different cysts of the maxilla and mandible.
Answer.
Cysts Of Jaws:
- Odontogenic cysts:
- Radicular cyst
- Dentigerous cyst
- Residual cyst
- Odontogenic keratocyst
- Calcifying odontogenic cyst
- Primordial cyst
- Globulomaxillary cyst
- Median mandibular cyst
- Non – Odontogenic Cysts:
- Incisive canal cyst
- Nasoalveolar cyst
- Median palatine cyst
- Traumatic bone cyst
- Aneurysmal bone cyst
Read And Learn More: Oral Radiology Question and Answers
Question 2. Describe the radiographic appearance of different stages of osteomyelitis of the jaw
Answer.
Osteomyelitis:
Early Acute:
- No radiographic changes are absorbed
Established Suppurative:
- The density of the involved bone is decreased
- Loss of sharpness of trabeculae
- Outline becomes blurred
- Gradually solitary or multiple radiolucent areas may be seen on the radiograph representing enlarged trabeculae spaces
- Saucer saucer-shaped area of destruction with irregular margins with teeth and some supporting bone is seen
- Inflammatory exudates may lift the periosteum, which is seen as a thin radiopaque line adjacent to and almost parallel or slightly convex to the surface
- There is a loss of continuity of lamina dura
Chronic Type:
- Multiple radiolucencies of variable size with irregular outlines and poorly defined borders are seen
- The bone gradually develops a moth-eaten appearance, as radiolucent areas enlarge and are separated by islands of normal bone
- Segments of the necrotic bone become detached and calcified and are called sequestra
- Sequestra are more dense and better defined due to sclerosis
- It often stimulates the formation of periosteal new bone which is seen as a single radiopaque or a series of radiopaque lines parallel to the surface of the critical bone gradually the radiolucent strip that separates the new bone from the outer cortical bone may be filled with sclerotic bone
- Roots may undergo resorption
- Lamina dura becomes less apparent
- The Fistula tract may appear as a radiolucent band
Interpretation of dental radiographs
Radiographic Interpretations Short Essays
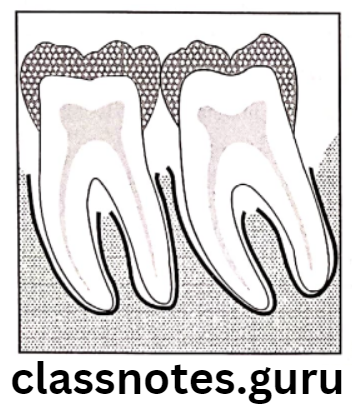
Question 1. Radiographic features of periodontal disease
Answer.
Early Or Mild Periodontitis:
- It is represented as an area of localized erosion of the alveolar bone crest
- In the anterior region, it is seen as the blunting of the alveolar crests
- In the posterior region, there may be a loss in the sharp angle between the lamina dura and the alveolar crest
- There is a loss of the cortical margins
- It appears rounded off with irregular diffuse margins
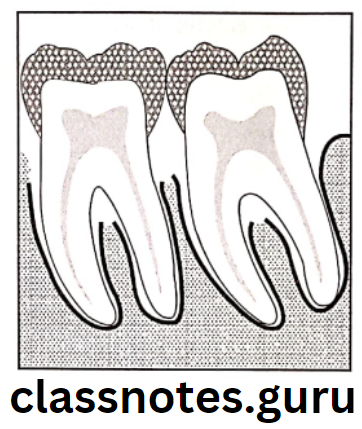
Moderate Periodontitis:
- The Buccal and lingual cortical plates are resorb
- There may be bone defects of bone between both plates
- It is seen as generalized horizontal bone erosion or localized angular defect
Horizontal Bone Loss:
- There is a loss of height of the alveolar bone with the crest still horizontal or parallel to the occlusal plane
Vertical Osseous Defect:
- These are localized lesions
- They appear as an oblique angulation of the alveolar bone in the area of the involved teeth
Types:
- Interproximal craters
- Proximal intrabony defect
- Two walled defects
- Interproximal hemisepta
- Inconsistent bony margins
Radiograph reading and diagnosis
Surrounding Internal Bone Changes:
- Peripheral bone may appear radiolucent due to loss of density and number of trabeculae
- The sclerotic bone appears as a dense amorphous radiopaque mass
Advance Or Severe Periodontitis:
- Extensive bone loss
- Excessive mobility
- Extensive osseous defects
Furcation Involvement:
- Bone resorption extending down the side of the multirooted tooth
- The thickening of the periodontal ligament space at the apex of the inter radicular bone crest
- The radiolucent image is sharply outlined between the roots
- The cortical plates appear more irregular
Aggressive Periodontitis:
Types:
- Localized juvenile periodontitis
- Associated with attachment loss
- Vertical bone loss with maxillary teeth (incisors & / molars)
- There are arch or saucer-shaped defects with strong arch symmetry
- Generalized juvenile periodontitis
- It may involve a variable number of teeth
- A Rapid bone loss which may be of the vertical angular or horizontal pattern is seen
- Progressing periodontitis
Tooth Mobility:
- In the case of the single tooth, it may develop an hourglass-shaped
- In multirooted teeth, widening of periodontal space is seen
Question 2. Radiographic features of dental caries
Answer.
Dental Caries Types:
- Proximal Caries:
Types:
- Incipient proximal lesions:
- It appears as a classical triangle with its broad base at the tooth surface spreading along the enamel rods
- It appears as a notch, a dot, a band, or a thin line
- Moderate proximal lesion:
- These involve more than the outer half of the enamel
- It doesn’t extend upto DEJ
- Different appearances:
- Triangular in shape with the base at the surface of the tooth
- Diffuse radiolucent image
- Combination of the above
- Advanced proximal lesions:
- These depict lesions invading the DEJ
- It appears triangular and diffuse
- This is the spreading of the demineralization process
- Usually, the lesion does not spread beyond more than half the thickness of the dentine
- Incipient proximal lesions:
- Pit And Fissure Caries:
Types:
- Incipient Occlusal Lesions:
- These are not usually detected on the radiograph unless the lesion reaches the dentin
- The only change is seen as a grey shadow just below the DEJ
- Moderate Occlusal Lesions:
- It appears as a broad base thin radiolucent zone in the dentine with little or no change apparent in the enamel
- Occlusal caries in dentine appears as a band of increased opacity between the carious lesion and the pulp chamber
- Severe Occlusal Lesions:
- Depict large cavity in the crown
- Pulp exposure is looked for
- Incipient Occlusal Lesions:
- Buccal/Facial/Lingual/Cervical Caries:
- These occur in enamel pits and fissures
- They appear as small round radiolucencies and become elliptical or semilunar as the lesion enlarges they have sharp well-defined borders
- Surrounded by apparent radiolucency
- If the lesion extends up to the distal line angle it may appear as a proximal caries
- Root Surface Caries:
- It involves both cementum and dentin
- It is common in mandibular molars and premolars
- It appears as an “ill-defined saucer-like crater”
- When the periphery surface is small it appears “notched”
- Rampant Caries:
- Common in children with poor dietary habits and poor oral hygiene
- It is seen as an extensive inter-proximal caries involving almost the whole of the primary dentine
- Recurrent Caries:
- It develops at the margins of an existing restoration
- A lesion next to the restoration may be distinguished from the radiopaque image of the restoration
- Nursing Bottle Caries:
- The affected teeth are maxillary and Mandibular first permanent molars and the Mandibular canine
- Radiation Caries:
- Appears as dark radiolucent shadows at the necks of teeth
- It is more apparent in the mesial and distal aspects
Basics of radiographic interpretation
Question 3. Radiographic appearance of odontoma.
Answer.
Radiographic appearance of odontoma
- Appears as well-defined radiolucencies with well-corticated borders
- Surrounded by a thin radiolucent zone representing a capsule
- Compound – a bag of teeth appearance
- Appears as numerous, small miniature teeth or tooth-like structures projecting from a single focus
- Present between roots of erupted permanent teeth or above the crown of impacted teeth
- Complex – sunburst appearance
- Radiopaque mass within jawbone is present
- Compound – a bag of teeth appearance
Question 4. Radiographic appearance of fibrous dysplasia
Answer.
Radiographic appearance of fibrous dysplasia
- Initially, it produces unilocular or multilocular radiolucent areas in the bone
- Expansion and distortion of cortical plates occurs
- Displacement of teeth
- The egg-cell crackling of the cortex of the bone is present
- Later a classical ground glass or orange peel appearance of bone is seen
- The margin of the lesion blends with the surrounding normal bone
- Mandibular lesions cause bulging of the inferior borders
- Narrowing of periodontal ligament
- Thinning of lamina dura
- Maxillary lesions causes obliteration of maxillary sinus
Question 5. Radiographic appearance of hyperparathyroidism
Answer.
Radiographic appearance of hyperparathyroidism
- Radiodensity – Radiolucent lesion
- There may be a normal, granular, or ground-glass appearance
- Moth-eaten appearance with varying density
- Ostelitis fibrosa generalization – Localised bone destruction
- Brown tumor – represents ill-defined radiolucency
- Thinning of cortical tables
- Pepper pot skull
- Demineralization of the inferior border of the mandibular canal
- Thinning of outlines of the maxillary sinus
- Loss of lamina dura
Radiographic Interpretations Short Answers
Question 1. Radiographic features of ameloblastoma
Answer.
Radiographic features of ameloblastoma
- It develops in the Mandibular ramus region
- It may extend to the symphysis
- In the maxilla, it is more common in the third molar region and may extend into the maxillary sinus and nasal floor
- It has well defined corticated border which is curved and in small lesions, the border shape may be distinguishable from the cyst
- The internal structure varies:
- Unilocular cyst-like appearance with a hyperostotic border
- Area of bone destruction having smooth curved margins that are well defined, corticated, and situated within the cavity in an arrangement of coarse trabeculae
- The thickness of the trabeculae varies from delicate strands to 2 mm width
- In some large lesions, it is found that there is an almost complete loss of bony margins of the jaws
- Multilocular cyst-like appearance which shows multiple cystic cavities with thin septae
- The presence of cysts bunched together
Oral radiology interpretation questions
Question 2. Radiographic features of OKC
Answer.
Radiographic features of OKC
- The radiographic appearance of odontogenic keratocyst shows aggressive growth with undulating borders, cloudy interiors, and the presence of internal septa which may give a multilocular appearance
- The margins are hyperstatic
- The size may vary from 5 cm to more in diameter
- They are usually oval shape
- It may expand and perforate the lingual and Buccal cortical plates
- Causes expansion of them
- It causes downward displacement of the inferior alveolar canal and resorption of the lower cortical plate of the mandible
- As it enlarges it may produce deflection of the unerupted teeth
- Root resorption may be seen
OKC Types:
- Envelopment
- This embraces an adjacent unerupted teeth
- Replacement:
- This forms in the place of normal teeth
- Extraneous
- These are in the ascending ramus away from the teeth
- Collateral
- These are adjacent to the roots of teeth
Question 3. Radiographic features of osteogenic sarcoma
Answer.
Radiographic features of osteogenic sarcoma
- The mandible is more frequently involved
- Common sites are the body of the mandible and the alveolar ridge
- The bony lesion is radiolucent with poorly defined, ragged borders
- Widening of PDL space
- Unusual unilateral bone resorption
- Cemental resorption
- Widening of the mandibular canal
- Early in the course of the disease, it is usually located centrally in the jaws
- Sometimes, it appears as a radiolucency in the periapex or more toward the periphery of the ridge or cortical plates
- It may originate adjacent to or seemingly in the periodontal space
Question 4. Radiographic features of proximal caries
Answer.
Proximal Caries Types:
- Incipient proximal lesions:
- It appears as a classical triangle with its broad base at the tooth surface spreading along the enamel rods
- It appears as a notch, a dot, a band, or a thin line
- Moderate proximal lesion:
- These involve more than the outer half of the enamel
- It doesn’t extend up to DEJ
- Different appearances:
- Triangular in shape with the base at the surface of the tooth
- Diffuse radiolucent image
- Combination of the above
- Advanced proximal lesions:
- These depict lesions invading the DEJ
- It appears triangular and diffuse
- This is the spreading of the demineralization process
- Usually, the lesion does not spread beyond more than half the thickness of the dentine
Question 5. Radiographic features of periapical granuloma
Answer.
Radiographic features of periapical granuloma
- Periapical area is radiolucent with loss of lamina dura
- The radiolucency may be of variable size at the apex of the tooth, usually of a diameter less than 1.5cm
- The lesion may or may not have a well-defined border
- There is a loss of lamina dura and periapical bone which is called “Periapical rarifying osteitis”
- The involved tooth may show a deep restoration, extensive caries, fracture, or a narrow pulp canal with nonvital pulp
How to interpret dental X-rays
Question 6. Radiological appearance of periapical cemental dysplasia
Answer.
Radiological appearance of periapical cemental dysplasia
The radiographic appearance of periapical dysplasia varies in different stages of the disease
- Osteolytic stage:
- The lesion presents as a small, well-defined, radiolucent area near the apex of the involved tooth
- Radiolucency is present in continuation with the periodontal ligament space
- Cementoblastic stage:
- The lesion appears as a radiolucent area containing multiple small radiopaque foci
- Mature stage:
- Present as well well-defined radiopaque mass at the root apex, being surrounded by a thin radiolucent zone
Question 7. Garre’s osteomyelitis
Answer.
Garre’s osteomyelitis
- Presents as a mottled radiolucent lesion with few radiopaque foci
- The cortex of bone exhibits many concentric or parallel opaque layers giving onion skin appearance
- It shows focal overgrowth of bone on the outer surface of the cortex
- Described as a duplication of the cortical layer of bone
- Few newly formed bony trabeculae are oriented perpendicular to onion skin layers
Question 8. Radiological appearance of fibrous dysplasia
Answer.
Radiological appearance of fibrous dysplasia
- Initially, it produces unilocular or multilocular radiolucent areas in the bone
- Expansion and distortion of cortical plates occurs
- Displacement of teeth
- The egg-cell crackling of the cortex of the bone is present
- Later a classical ground glass or orange peel appearance of bone is seen
- The margin of the lesion blends with the surrounding normal bone
- Mandibular lesions cause bulging of the inferior borders
- Narrowing of periodontal ligament
- Thinning of lamina dura
- Maxillary lesions causes obliteration of maxillary sinus
Question 9. Radiological appearance of Paget’s disease
Answer.
Radiological appearance of Paget’s disease
- Initially, there is the presence of radiolucent areas in the affected bone
- In the next stage, involved bone shows haphazardly arranged newly formed bone in radiolucent areas
- This produces the cotton wool appearance
- Radiopacity of lesions increases due to increased osteosclerosis
- Obliteration of maxillary sinus
- Hypercementosis of tooth
- Loss of lamina dura
- Obliteration of periodontal ligament space
- Root resorption
Question 10. Multilocular radiolucencies of jaws
Answer.
Multilocular radiolucencies of jaws
Multilocular radiolucencies of jaws are
- Odontogenic keratocyst
- Ameloblastic
- Central giant cell granuloma
- Cherubism
- Odontogenic myxoma
- Aneurysmal bone cyst
- Central hemangioma of bone
Question 11. Onion peel appearance
Answer.
Onion peel appearance
- It demonstrates multiple concentric parallel layers of new bone adjacent to the cortex
- The layers are thought to be the result of periods of variable growth
- It can be seen with
- Osteosarcoma
- Acute osteomyelitis
- Ewing sarcoma
- Langerhans cell histiocytosis
Question 12. Moth eaten appearance
Answer.
Moth eaten appearance
- It describes multiple small endosteal lucent lesions often with poorly defined margins
- Consists of multiple scattered holes that vary in size and arise separately
- These holes coalesce to form larger areas of bone destruction
- It is a bone marrow process
- It is seen in
- Multiple myeloma
- Primary bone lymphoma
- Ewing sarcoma
- Infection
- Eosinophilic granuloma
- Malignant fibrous histiocytoma
- Metastases
Radiographic diagnosis in oral pathology
Question 13. Sunburst appearance
Answer.
Sunburst appearance
- Sunburst appearance is a type of periosteal reaction giving the appearance of a sunburst secondary to an aggressive periostitis
- It occurs when the lesion grows too fast and the periosteum does not have enough time to lay down a new layer
- In such cases, the Sharpey’s fibers become stretched out perpendicular to the bone
- When these fibers ossify, they produce a pattern called a sunburst appearance
- It is frequently associated with osteosarcoma
Radiographic Interpretations Viva Voce
- A dentigerous cyst is associated with the crown of unerupted teeth
- The most common site for the occurrence of nasopalatine canal cyst is the maxillary central incisor
- AOT is commonly associated with an unerupted tooth