
Pediatric Restorative Dentistry Important Notes
1. Advantages of GIC
- Tooth-colored material
- Adherence to both enamel and dentin
- Fluoride release
2. Calcium hydroxide
- It was introduced by Herman for pulp capping
- It is very alkaline with pH 11-13 which ensures the inability of bacteria to thrive in its presence
- If placed too close to pulp, it will cause necrosis If adjacent pulp tissue and inflammation
- Dentin bridge formation occurs at the junction of the necrotic tissue and vital inflamed tissue
- When it is applied as liner the excess calcium ions present in the cement would be available to the pulp and would encourage remineralization with the pulp chamber
Read And Learn More: Pedodontics Short Essays Question And Answers
3. Modification in class 2 cavity preparation in primary teeth
- Due to the presence of broad contact areas, the gingival floor should be wide to place the margins in self-cleansing areas
- Due to cervical constriction, the gingival wall should not be too gingival
- The width of the isthmus should not exceed l/3rd of the intercuspal distance
- The gingival seat should not be beveled
- Avoid mesiobuccal pulp horn in case of small first molars
4. Esthetic preformed crowns
- Polycarbonate crowns
- Strip crowns
- Pedo jacket crowns
- Fuks crown
- New Millenium crown
- Nusmile crowns
- Cheng crown
- Dura crowns
- Pedo pearls
5. Rubber dam
- It was developed by Barnum
- A latex rubber dam is available in 5 *5 or 6 6 size
- Non-latex rubber dam is available in 6 * 6 size
Pediatric Restorative Dentistry Long Essays
Question 1. Classify stainless steel crowns, and mention their indications. Give a stepwise description of resto¬ration with it.
(or)
Mention uses, advantages, disadvantages, and preparation for stainless steel crown for tooth 85.
Answer:
Stainless steel crown Classification
1. Based on composition:
- Stainless steel crown:
- These alloys are made up of authentic steel with the composition
- 17-19% chromium
- 9-13% nickel
- 0.08-0.12% carbon
- These alloys are made up of authentic steel with the composition
- Nickel-base crown:
- Contains
- 76% nickel
- 15.5% chromium
- 8% iron
- 0.04% carbon
- 0.35% manganese
- Tin-base crowns:
- 96% tin
- 4% silver
- Aluminum base crown:
- Contains
- 1.2%-manganese
- 10% magnesium
- 0.7% iron
- 3% silicon
- 0.25% copper
2. Based on morphology:
- Untrimmed/ uncontoured crowns
- The sides are straight and longer
- Pretrimmed crowns
- The sides are straight but shorter
- Precontoured crowns
- Crowns are more rounded in the gingival margin
Stainless steel crown Uses/ Indications:
- Teeth with extensive caries
- Presence of developmental defects of teeth
- Teeth with hypoplastic defects
- Restoring teeth after pulpal therapy
- As a preventive restoration
- It is used as an abutment
- As temporary restoration of a fractured tooth
- In the presence of parafunctional habits
- Malocclusion – Single tooth cross bite
- For replacement of prematurely lost anterior
Stainless steel crown Advantages:
- Good life span
- Good retention and resistance
- Acceptable
- Cost-effective
Stainless steel crown Disadvantages:
- It may lead to
- Ledge formation in interproximal region
- Tilting of crown
- Poor marginal adaptation
Stainless steel crown Preparation:
- Occlusal reduction is done up to 1.5-2 mm
- Proximal walls are made converging occlusal
- Next, buccal and lingual surfaces are made at least 0.5 mm
- Buccal and lingual surfaces converge occlusal
- Rounding of line and point angles Even the occlusal third of buccal and lingual surfaces are made rounded seating of crown > Initially seat the lingual portion by applying gentle pressure in a buccal direction
- Examine the gingival margins of the crown
- Contour the crown along the tooth anatomy
- Finishing and polishing of the crown is done
- Finally, cementation with zinc phosphate, zinc polycarboxylate or GIC is done
- Excess cement is removed using Explorer and knotted dental floss
Pediatric Restorative Dentistry Short Essays
Question 1. Tooth preparation for stainless steel crown.
Answer:
- Tooth preparation mainly involves 3 steps
1. Occlusal preparation:
- Bur is used to reducing the occlusal surface by 1.5-2 mm following the cuspal outline
- Cusp are reduced preserving as much tooth structure as possible
- It is done prior to proximal reduction
2. Proximal reduction:
- Wooden wedges are used in the interproximal embrasures to reduce the risk of damage to adjacent teeth
- Bur is swept buccolingually across the proximal surface
3. Roundening of line angles:
- All line angles created are rounded by moving the bur at the angle of 45 degrees
Crown Selection
- Crown is selected by
- Adequate mesiodistal diameter
- Light resistance to seating
- Proper occlusal height
Crown Seating
- The selected crown should be placed on the lingual side and rotated to the buccal side
- The crown should fit loosely with 2-3 mm of excess on the gingival side
Adapting The Crown
- Pliers are used to contouring the gingival edges to tighten the fit of the crown
- Poorly adapted crowns will serve as a collection area for bacteria and can cause recurrent caries
Finishing
- After adaptation, the crown margin should be trimmed using green stone in a counterclockwise direction at 45 degrees angle
Question 2. Class 2 Cavity Preparation for primary 2nd molar.
Answer:
1. Occlusal Form:
- Extend the cavity margins to include all carious lesions
- Cavity margins should be such that it can be easily assessed and include self cleansable area
- Initial pulpal depth is maintained as 0.5 mm into the dentin
2. Proximal Reduction:
- Proximal ditch cut is given
- Provide 0.2-0.3 mm proximal clearance
- The depth of the axial wall is maintained to 0.5 mm in dentin
- The gingival seat is not beveled
Resistance Form – Features:
- Flat pulpal floor
- Box-shaped cavity
- Rounded internal line angles
- 90o cavosurface angle
- Width of cavity not more than l/3rd of intercuspal distance
- Adequate bulk of the restorative material
- The reverse curve is provided
Retention Form:
- Converging occlusal walls
- Preservation of uninvolved marginal ridge
- Dovetail provided over the uninvolved marginal ridge
- An inverse taper of 5 degrees is given
Convenience Form:
- It is the form of cavity that facilitates access for instrumentation, condensation, adaptation, and finishing
- Removal of any remaining defects
- Removal of infected dentin
Finishing Of The External Walls:
- Pulp protection:
- In the case of a deep cavity, the pulp is protected with the help of bases
- Final Step:
- Cleaning and inspecting the cavity preparation
Question 3. Baume’s Classification.
Answer:
- It is for the classification of dental caries
- It consists of
1. Pit and Fissure lesions:
- Pit and Fissures are the depression prevented over the occlusal surfaces of posterior teeth
- If they are narrow, they can be self cleansable
- But, however, widened pit and fissures are more prone to caries
- Such pit and fissure can be prevented by pit and fis¬sure sealants
2. Smooth Surface Caries:
- These involve the proximal surfaces of posterior teeth
- These are common in deciduous teeth due to the presence of open contacts
- Open contacts results in food lodgement
- The stagnant of food in these areas leads to demin¬eralization of the calcified tooth structure
- This further leads to the development of caries
Question 4. Matrices.
Answer:
Matricing is the procedure of creating a temporary wall opposite to the axial wall
Matrices Objectives:
- Creates good proximal contour
- Good adaptation of restoration is provided
- Improves the accessibility
- Holds the material while it is setting
- Avoid contamination of restoration
- To some extent, it displaces gingiva
Matrices Types:
1. For class 1 cavity:
- Double-banded Tofflemire
2. For class 2 cavity:
- Single banded Tofflemire
- Ivory No. 1
- Ivory No. 8
- Automatic
- S-shaped matrix band
- T-shaped matrix band
3. For class 3 cavity:
- Transparent celluloid strips
4. For class 4 cavity:
- Celluloid strips
- Crown form matrices
5. For class 5 cavity:
- Window matrix
Question 5. Atraumatic Restorative Treatment.
Answer:
- It is a procedure that involves conservative tooth preparation and restoration it by using only hand instruments
Atraumatic Restorative Method:
- Remove the carious lesion with the help of spoon exca¬vator
- With the help of a hatchet remove the unsupported enamel
- Clean the cavity
- Isolate the cavity
- Condition the cavity by placing a drop of GIC liquid with the help of wet cotton
- Wiped out and rinse the cavity immediately to remove the excess of polyacrylic acid
- Now, dry the cavity
- Manipulate Glass ionomer cement
- Place the cement as a thick mix, into the cavity, con-dense it with finger pressure
- Apply a layer a varnish over it to protect it against con¬tamination
- Atraumatic Restorative
Atraumatic Restorative Advantages:
- Conservative
- No need of complicated procedures
- Minimize the risk of iatrogenic errors
Question 6. Polycarbonate Crowns.
Answer:
- These are temporary crowns which can be given as fixed prostheses to deciduous anterior teeth
Polycarbonate Crowns Contraindications:
- Severe bruxism
- Deep bite
- Excessive abrasion
Polycarbonate Crowns Advantage:
- Easy and quick
- Can be easily adjusted
Polycarbonate Crowns Technique:
- Select the crown according to the dimension of the tooth
- Proceed with the tooth preparation
- Facial and lingual reduction – 0.5-1 mm
- Proximal reduction – 0.5-1 mm
- Incisal reduction – 1-2 mm
- Examine the preparation
- Check for the adaptation of crown
- Trim and Finish the margins of the crown
- Finally, the cementation of the crown is carried out
Question 7. Glass Ionomer Cement (GIC).
Answer:
Glass Ionomer Cement Advantages:
- Chemical bonding
- Esthetic
- Fluoride releasing property
Glass Ionomer Cement Disadvantages:
- Susceptible to erosion
- Less wear resistance
- Brittle in nature
Glass Ionomer Cement Classification:
- Type 1 – Luting
- Type 2 – Restorative
- Type 2-1 – Restorative esthetic
- Type 2-2 – Restorative reinforced
- Type 3 – Lining or base
Glass Ionomer Cement Composition:
- Powder:
- Silica
- Alumina
- Aluminum fluoride
- Calcium fluoride
- Aluminum phosphate
- Sodium fluoride
- Liquid:
- Polyacrylic acid
- Tartaric acid
- Water
Glass Ionomer Cement Uses:
- Asa sealant
- As liners and bases
- For luting of brackets
- Restorative material
- As temporary restoration
- As core build-up
- For atraumative restorative treatment
Glass Ionomer Cement Properties:
- Compressive strength – 150 MPa
- Tensile strength – 6.6 MPa
- Hardness – 49 kHN
- Fracture toughness
- Solubility – 0.4%
- Adhesion – Chemical bonding
- Esthetic
- Bio-compatible
- Fluoride release
Glass Ionomer Cement Setting time:
- Type 1 – 4.5 min
- Type 2 – 7 min
Powder Liquid Ration 1:5:1 OR 3:1:
- Modifications:
- Fiber reinforced GIC
- Metal reinforced GIC
- Cermet cement
- Resin modified GIC
Pediatric Restorative Dentistry Short Answers
Question 1. Rubber dam sheet
Answer:
- They are available in 5″ X 5″ or 6″ X 6″ sizes
- Available thicknesses are:
- Thin- 0.15 mm
- Medium- 0.20 mm
- Heavy- 0.25 mm
- Extra heavy 0.30 mm
- Special heavy – 0.35 mm
- It is available in green, blue, black, pink, and burgundy colours and mint, banana, and strawberry flavors
- The rubber dam sheet has a darker side and a shiny side
- The shiny side should always be towards the tissue so that the dam can pass easily over them with minimal irritation
- The dull side should be towards the occlusal aspect so that it does not reflect the light from it
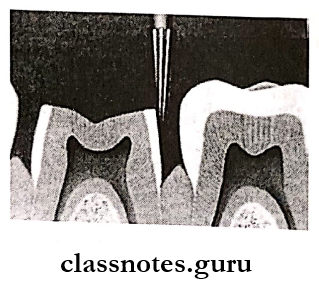
Question 2. Tunnel cavity preparation.
Answer:
- Tunnel cavity preparation is a modification of class 2
Tunnel cavity Indications:
- Small cavities
- Cavities that are placed 2-2.5 mm below the marginal ridge
Tunnel cavity AIMS:
- Access via occlusal aspect
- To preserve the strength of the marginal ridge
- To prevent the formation of a proximal cavity
Tunnel Cavity Procedure:
- Caries is removed by using slow-speed round bur
- The proximal wall is not fractured if it is not involved
- The remaining caries is removed with a spoon excavator
- The cavity is restored using G1C
Question 3. Semi-permanent restorations.
Answer:
- Semi-permanent restoration are used to restore the lost tooth structure and stabilize it
- Polycarbonate and stainless steel crowns are used as semi-permanent restorations
1. Polycarbonate crowns:
- They are heat molded acrylic resins used to restore anterior teeth
- They do not resist strong abrasive forces, leading to occlusal fracture and de-bonding or dislodgement
2. Stainless steel crown:
- It is used in primary and young permanent teeth
- It was introduced by Humphrey in 1950
- It is more frequently used in deciduous dentition
Question 4. Rubber dam.
Answer:
- Used for isolation
Rubber dam Purpose:
- Retraction of soft tissue
- Improves efficiency of the treatment
- Improves properties of restorative material
- Provides clean and dry field
- Prevents contamination
Rubber dam Contraindication:
- Asthmatic patient
- Newly erupted teeth
- Patients with allergic to late
Rubber dam Components
- Rubber dam sheet
- Rubber dam frame
- Rubber dam punch
- Rubber dam forceps
- Dental floss
- Rubber dam napkin
- Clamps
Question 5. Saliva Ejectors.
Answer:
- Prevent pooling of saliva in the floor of the mouth
Saliva Ejectors Types:
- Metallic – Can be autoclaved
- Plastic – Disposable
Saliva Ejectors Advantages:
- Provides adequate dry field
- No dehydration of oral tissues
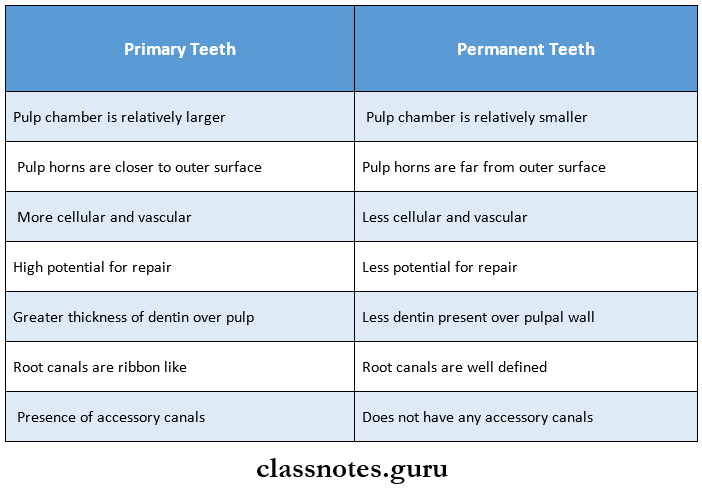
Question 6. Pulpal Differences between primary and permanent teeth.
Answer:
Question 7. Celluloid/Strip Crowns.
Answer:
- Esthetic crown
Strip Crowns Technique:
- Anaesthetise and isolate the tooth
- Selection of celluloid crown
- Tooth preparation
- Incisal reduction – 1.5-2 mm
- Proximal reduction – 0.5-1 mm
- Labial reduction – 1 mm
- Lingual reduction – 0.5 mm
- Rounding of line angles
- Trim the crown margin
- Place the ventholes
- Fill the crown with composite
- Etch and dry the tooth
- Apply bonding agent
- Seat the crown upto polymerization of the resin
- Strip the celluloid crown using the explorer
- Check for occlusion
- Finishing and polishing done
Question 8. Intermediate Restoration.
Answer:
Intermediate Restoration Features/Requirements:
- Nonirritant
- Esthetic
- Easy to apply and remove
- Maintain periodontal health
- Should have adequate strength
Intermediate Restoration Cement Used:
- Zinc oxide eugenol
- Zinc Phosphate
- Zinc polycarboxylate
- Glass ionomer
- Calcium hydroxide
Question 9. Reparative Dentin.
Answer:
- It is formed as a response to external stimuli
- It is irregular with cellular inclusions
- Has decreased permeability
- Formed by secondary odontoblasts that are differentiated from mesenchymal cells of the pulp
- Helps in the prevention of diffusion of noxious agents from the tubules
Question 10. Calcium Hydroxide.
Answer:
Calcium Hydroxide Use:
- Intracanal medicament
- Pulp capping agent
Calcium Hydroxide Effect:
- Bactericidal
- Stimulate secondary dentin formation
- Denature proteins
- Aids in the dissolution of necrotic pulp
- Increases alkalinity
- Destroys micro-organisms in inaccessible areas
Calcium Hydroxide Available Form:
- Powder and liquid
- Paste form
Question 11. Gamma 2 phase(γ2).
Answer:
- γ2 phase is SngHg
- It is the weakest phase
- Its hardness is 10% that of
- Least corrosion resistance
Pediatric Restorative Dentistry Viva Voce
- GIC was developed by Wilson and Kent
- Stainless steel crown was introduced by Humprey
- The finish line for the stainless steel crown is feather edge
- The crown should extend 1 mm below the gingival crest
- In the primary dentition, a rubber dam is routinely placed over c,d,e
- The universal clamp used for stabilizing the rubber dam during mixed dentition is 5.5 # 206