
Hemodynamic Derangements Due To Deranged Volume Important Notes
1. Hyperaemia
- Increased volume of blood from arterial and arteriolar dilatation is called hyperemia
- It is seen in
- Inflammation
- Blushing
- Menopausal flush
- Muscular exercise
- High-grade fever
- The affected organ is pink or red
2. Caissons disease
- It is a form of gas embolism
- It is produced when an individual decompresses suddenly either from high atmospheric pressure to normal level or from normal pressure to low atmospheric pressure
3. Lines of Zahn
- It consists of alternate layers of aggregated platelets within fibrin meshwork and red cells
- Lines of Zahn are distinct in arterial thrombi
4. In hypovolemic shock, kidneys conserve body fluids by
- Reducing GFR
- Releasing aldosterone and ADH – aldosterone increases renal retention of sodium and water
Hemodynamic Derangements Due To Deranged Volume Long Essays
Question 1. Define shock. Discuss classification, pathogenesis, and pathology of shock.
(or)
Discuss Etiology, pathogenesis, and pathology of shock.
Answer:
Shock: Shock is a life-threatening clinical syndrome of cardiovascular collapse characterized by:
- An acute reduction of effective circulating blood volume [Hypotension) and
- Inadequate perfusion of cells and tissues [Hypoperfusion).
Types Of shock:
Classification and etiology of shock:
1. Hypovolaemic Shock
- Acute hemorrhage
- Dehydration from vomiting, diarrhoea
- Burns
- Excessive use of diuretics
- Acute pancreatitis
2. Cardiogenic Shock
- Deficient emptying example
- Myocardial infarction
- Cardiomyopathies
- Rupture of the heart, ventricle or papillary muscle
- Cardiac arrhythmias
- Deficient filling example
- Cardiac tamponade from haemopericardium
- Obstruction to the outflow example
- Pulmonary embolism
- Ball valve thrombus
- Tension pneumothorax
- Dissecting aortic aneurysm
Read And Learn More: Pathology Question And Answers
3. Septic Shock
- Gram-negative septicemia (endotoxic shock) example Infection with E. coli, Proteus, Klebsiella, Pseudomonas and Bacteroides
- Gram-positive septicemia (exotoxic shock) example Infection with streptococci, pneumococci
4. Other Types
- Traumatic shock
- Severe injuries
- Surgery with marked blood loss
- Obstetrical trauma
- Neurogenic shock
- High cervical spinal cord injury
- Accidental high spinal anesthesia
- Severe head injury
- Hypoadrenal Shock
- Administration of high doses of glucocorticoids
- Secondary adrenal insufficiency (example in tubercu¬losis, metastatic disease, bilateral adrenal hemorrhage, idiopathic adrenal atrophy)
Pathology of Shock:
- Shock is characterized by multi-system failure.
- The morphogenic changes in shock are due to hypoxia resulting in degeneration and necrosis in various or¬gans.
- Predominant morphologic complications in shock are as follows:
1. Hypoxic Encephalopathy:
- An altered state of consciousness may be produced by cerebral ischemia in compensated shock.
- In prolonged shock and cardiac arrest, the brain suffers from severe ischaemic damage with loss of cortical functions, coma, and a vegetative state.
- Dead and dying nerve cells are replaced by gliosis.
2. Heart in shock:
- The heart is more vulnerable to the effects of hypoxia than any other organ.
- 2 important morphogenic changes in the heart are Hemorrhages and necrosis – There may be small/large ischaemic areas of infarcts, particularly located in the subepicardial and subendocardial regions.
- Zonal lesions- these are opaque transverse con-traction bands in the myocytes near the intercalated disc.
3. Shock lung:
- Due to dual blood supply lungs are not affected by hypovolaemic shock but are affected by septic shock. The lungs become heavy and wet.
- Microscopically, changes of adult respiratory distress syndrome (ARDS) are seen. Briefly, the changes include congestion, interstitial and alveolar edema, lymphocyte infiltration, fibrin, and platelet thrombi in the microvasculature.
4. Shock kidney:
- Irreversible renal injury is one of the most important complications of shock.
- Acute tubular necrosis occurs in which there are tubular lesions.
- The end result is generally anuria and death.
5. Adrenal changes in shock:
- Adrenals show stress syndrome which includes the release of aldosterone, glucocorticoid, and catecholamines like adrenaline.
- In severe shock, adrenal high can occur.
6. Haemorrhagic Gastroenteropahty:
The hypoperfusion of the alimentary tract in conditions such as shock and cardiac failure may result in mucosal and mural infarction called hemorrhagic gastro- teropathy.
7. Liver in shock:
Due to hypoxia vasodepressor ma¬terial is released which causes vasodilation, focal necrosis, fatty liver, and impaired liver functions grossly, faint nutmeg appearance is seen.
8. Other organs: Other organs such as lymph nodes, spleen, and pancreas may also show foci of necrosis in shock.
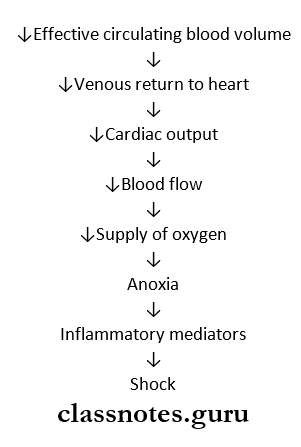
Pathogenesis: There are 2 basic features in the pathogenesis of shock.
1. Reduced effective circulating volume: It may result in either.
- By actual loss of blood volume as in hypovolemic shock or.
- By decreased cardiac output without actual loss of blood as in cardiogenic and septic shock.
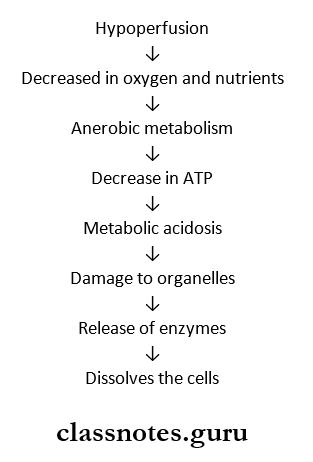
2. Tissue Anoxia:
- Following the reduction in effective cir¬culating blood volume, there is decreased venous return and hence Tsedcardic output.
- This leads to reduced 02 supply, hence tissue anoxia which sets in cellular injury.
3. Release of inflammatory mediators: In response to cellular injury, inmate immunity of the body gets ac¬tivated and there is the release of inflammatory media¬tors but eventually these agents themselves become the cause of cell injury.
Pathogenesis
Question 3. What are the factors leading to irreversible shock?
Answer:
Factors Leading To Irreversible Shock:
1. Progressive Vasodilatation
- Anoxia damages the capillary and venular wall
- Arterioles do not respond to vasoconstrictors
- This results in Vasodilatation and peripheral pool¬ing of blood
2. Increased vascular permeability
- Tissue damage occurs due to anoxia
- This releases inflammatory mediators
- Results in increased vascular permeability
3. Myocardial depressant factor
- Release of Myocardial depressant factor causes
- Fall in blood pressure
- Persistent reduced blood flow to myocardium a Coronal insufficiency
- Myocardial ischemia
4. Worsening pulmonary hypoperfusion Causes respiratory distress
5. Anoxic damage to the heart, kidney, and brain
- Due to anaerobic glycolysis, tissue anoxia causes
- Severe metabolic acidosis
- Release of inflammatory mediators
- Ischaemic cell death
6. Hypercoagulability
- Tissue damage activates the coagulation pathway which causes
- Release of clot-promoting factor, thromboplastin
- Release of platelet aggregator
- ADP
- Slowing of bloodstream
- Vascular thrombosis
Hemodynamic Derangements Due To Deranged Volume Short Essays
Question 1. Irreversible shock
Answer:
When the shock is so severe and no recovery takes place in spite of compensatory mechanism, therapy, and control of the etiologic agent which caused the shock, it is called decompensated/irreversible shock.
Irreversible shock Pathogenesis:
- Progressive vasodilation
- ↑Vascular permeability
- Myocardial depressant factor (MDF]
- Pulmonary hypoperfusion
- Anoxic damage
- Hyper coagulability
Irreversible shock Complications:
- Brain – hypoxic encephalopathy
- Heart – focal myocardial necrosis
- Lungs – ARDS
- Kidney – ATN
- GI – Haemorrhagic gastro enteropathy
- Liver – necrosis
- Blood-DIC.
- Adrenals – necrosis
Question 3. Chronic venous congestion of the liver.
Answer:
Liver Etiology:
- It is seen in
- Right heart failure
- Occlusion of inferior vena cava and hepatic vein
Liver Macroscopic Appearance:
- Enlarged liver
- The tensed capsule is present
Liver Cut Surface:
- Shows a nutmeg liver appearance
- It shows the red and yellow mottled appearance
- The red part corresponds to the congested center of lob¬ules
- The yellow part corresponds to the fatty peripheral zone
Microscopic Appearance:
- Centrilobular zone
- Shows severe hypoxia
- Distended central veins and adjacent sinusoids
- Degeneration of hepatocytes
- Hemorrhagic necrosis
- Fibrosis and regeneration of hepatocytes in long-standing cases
- Peripheral zone
- Less effected
- Fatty change in hepatocytes is seen
Question 4. Septic shock.
Answer:
Septic shock Etiology:
- Severe bacterial infection – more commonly Gram-negative
- Septicemia
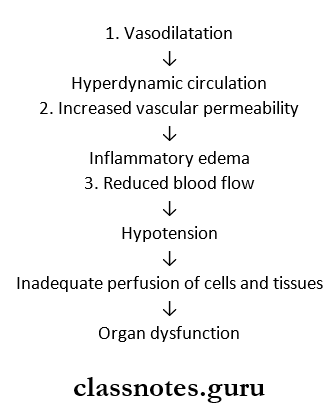
Septic shock Pathogenesis:
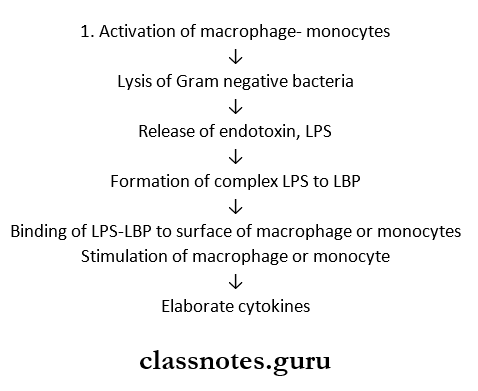
Septic shock Result:
- Produces more neutrophils which liberate free radical causing vascular injury
- Promotes NO synthase for vasodilatation and hypoten¬sion
2. Activation of other inflammatory response
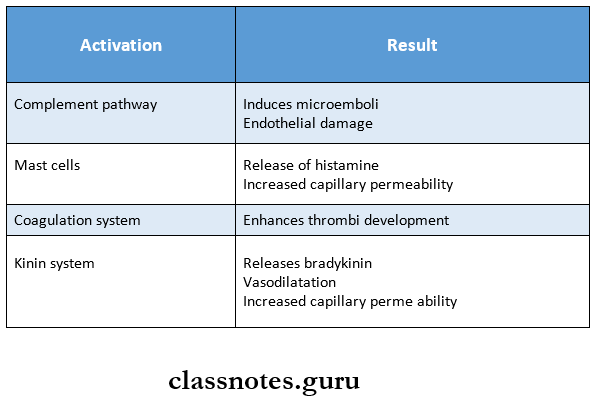
Activation of other inflammatory response Results
Hemodynamic Derangements Due To Deranged Volume Short Question And Answers
Question 1. Stages of shock
Answer:
Deterioration of the circulation in shock is a progressive phenomenon and can be divided into the following 3 stages.
1. Initial nonprogressive stage: During this stage reflex compensatory mechanisms are activated and perfusion of vital organs is maintained.
2. Progressive stage: This stage is characterized by tissue hypoperfusion and the onset of worsening circula¬tory and metabolic imbalances.
3. Irreversible stage: It sets in after the body has in¬curred cellular and tissue injury so severe that even if the hemodynamic defects are corrected, survival is not possible
Question 2.Anaphylactic shock
Answer:
Anaphylactic shock Definition:
- Anaphylaxis is a state of rapidly developing immune response to an antigen to which the individual is previously sensitized.
- Anaphylactic shock develops due to vasodilation and peripheral pooling of blood.
Anaphylactic shock Pathogenesis:
- IgE antibodies sanitize basophils of peripheral blood/most cells of tissue leading to the release of anaphy¬lactic mediators like histamine, serotonin, VIP, and chemotactic factors of anaphylaxis.
- The effects produced are increased vascular permeability, smooth muscle contraction, and early vasoconstriction followed by vasodilation and shock.
- Increased vascular permeability and vasodilation lead to peripheral pooling and blood. This results in a reduction of effective circulating volume and shock.
- Example: Systemic anaphylaxis due to administration of antisera drugs like penicillin.
Clinical features of systemic anaphylaxis include itching, erythema, contraction of respiratory bronchioles, pulmonary edema, shock, and death.
Question 3. Mechanism of shock in burns
Answer:
- Reduction in blood volume due to fluid loss in burns in¬duces hypovolemic shock.
- The major effects of hypovolemic shock are due to de¬creased cardiac output and low intracardiac pressure.
- Accordingly, clinical features are increased heart rate (Tachycardia), low blood pressure (hypotension), low urinary output, and alteration in mental state (agitated to confused to lethargic).
Question 4. End result in a shock
Answer:
- Acute respiratory distress syndrome
- Disseminated intravascular coagulation
- Acute renal failure
- Multiple organ dysfunction syndrome
- Stupor
- Coma
- Death
Question 5. Nutmeg liver.
Answer:
- It is seen in the cut surface of chronic congestion of the liver
- It shows the red and yellow mottled appearance
- The red part corresponds to the congested center of lobules
- The yellow part corresponds to the fatty peripheral zone
Question 6. Neurogenic shock.
Answer:
Neurogenic shock Pathophysiology:
Neurogenic shock Damage to Organs:
- Increase in myocardial contractibility
- ARDS
- Increase in blood pressure
- Toxaemia
- Bacteraemia
- Renal failure
- Upper GI bleeding
Neurogenic shock Management:
- Administration of oxygen
- Vasoactive drugs – Phenoxybenzamine
- Inotropic agents – Dopamine
- Corticosteroids – Prednisolonel5 mg/kg
- Mechanical ventilation
- Fluid replacement