
Common Specific Tumours Important Notes
1. Basal cell carcinoma
- It is locally invasive
- It rarely metastasize
- It is a slow growing tumour of middle age
- It occurs exclusively on hairy skin
- Common site: above the line of the tragus of the ear to the corner of the mouth
2. Squamous cell carcinoma
- It may arise from any parts of the skin and mucous membrane lined by squamous epithelium
- Predisposing factors are
- Solar keratosis
- Chronic ulcers
- Draining sinus
- Osteomyelitis
- Chewing betel nuts
- Tobacco
- Radiation
3. Teratoma: They are complex tumours composed of tissues derived from more than one of the three germ layers – endoderm, mesoderm and ectoderm
4. Hamartoma: It is a mass of disorganised but mature cells indigenous to the particular site
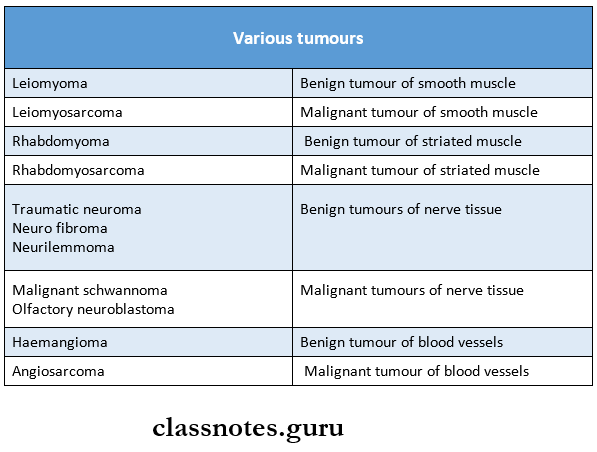
5. Various tumours:
Common Specific Tumours Short Essays
Question 1. Teratoma
Answer:
- Teratomas are complex tumours composed of tissues derived from more than one of the three germ cell layers
- They are commonly seen in the gonads of males and females
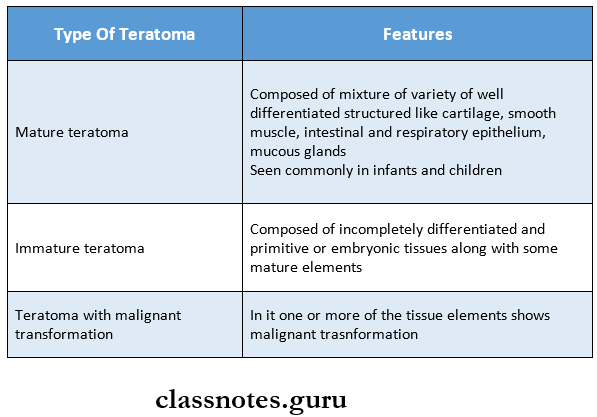
Teratoma Types:
- They are classified into three types
- Mature teratoma
- Immature teratoma
- Teratoma with malignant proliferation
Read And Learn More: Pathology Question And Answers
Teratoma Morphology:
- Gross appearance
- They appear as large, grey-white masses
- It enlarges the involved testis
- Cut surface:
- Shows grey-white solid areas, cystic and honey-combed areas
- Foci of cartilage and bone are also seen
- Microscopic features:
Question 2. Basal cell carcinoma
Answer:
- Also called as rodent ulcer. Most common tumour.
- If is a locally invasive, slow-growing tumour of middle-aged individuals which rarely metastasizes.
Basal cell carcinoma Etiology:
- Prolonged exposure to strong sunlight
- UV rays
- Arsenic is used in skin ointments.
- Dysregulation of the PTCH pathway
- Inherited effects of PTCH gene causing BCC, gorlin syndrome.
Basal cell carcinoma Clinical features:
- The majority of lesions occur on the face, usually abore a line joining lobe of the ear and the angle of the mouth.
- Common sites are the inner and outer canthus of the eye, the eyelids bridge of the nose and around nasolabial fold.
- Most common pattern is a nodule-ulcerative lesion a slow-growing small nodule that undergoes central with pearly, rolled margins.
- Tumour enlarges in size by burrowing and by destroying the tissues locally like a rodent and hence the name”rodent ulcer.
Basal cell carcinoma Microscopic examination: A most common pattern is solid basal cell carcinoma in which the dermis contains irregular masses of basaloid cells having the characteristic peripheral palisaded appearance of the nuclei.
Basal cell carcinoma Treatment:
- Tumours are usually treated with complete local excision.
- BCC responds well to radiation. Radiation is indicated in elderly patients with extensive lesions, does – 4000 – 6000 gy units.
Question 3. Microscopic picture of osteosarcoma
Answer:
- Microscopic examination of osteosarcoma shows following features
- Sarcoma cells
- The tumour cells are anaplastic mesenchymal stromal cells
- They show marked pleomorphism and polymorphism
- Cells may be spindles, round, oval, polygonal or bizarre tumour giant cells
- They show hyperchromatism and atypical mitosis
- Osteogenesis
- The anaplastic sarcoma cells form an osteoid matrix and bone directly
- It lies interspersed between the areas of tumour cells
- Sarcoma cells
Question 4. Microscopic picture of Osteoclastoma
Answer:
- Microscopic examination of osteoclastoma shows
- A large number of osteoclast-like giant cells which are regularly scattered throughout the stroma
- Giant cells may contain as many as 100 benign nuclei and are similar to normal osteoclast
- Stromal cells are mononuclear cells and are the tumour cells
- They are uniform, plump, spindle-shaped or round to oval in shape
- They may have varying degrees of atypia and mitosis
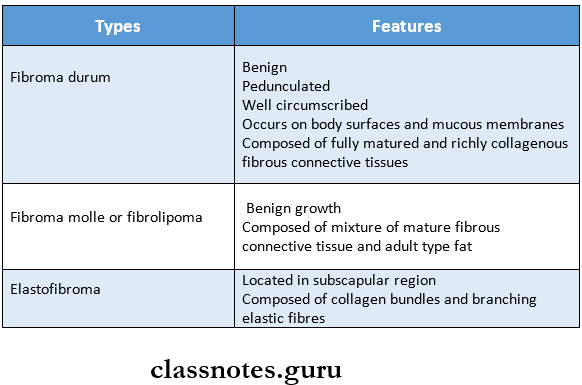
Question 5. Fibroma
Answer: Fibroma are uncommon tumours of soft tissues
Fibroma Types:
Based on microscopic appearance, fibroma are of three types
Common Specific Tumours Short Question And Answers
Question 1. Malignant melanoma
Answer: Malignant melanoma is a tumour arising from pigment-forming cells i.e., melanoblast which are desired from the neural crest.
Malignant Melanoma Etiology: Unknown but there is the role of excessive exposure of white skin sunlight.
Common site:
- Oral and anagenital mucosa,
- Oesophagus,
- Conjuctiva,
- Orbit,
- Leptomeninges.
Malignant melanoma Clinical features:
- Flat/slightly elevated nerves which has variegated pigmentation, and irregular borders and have undergone secondary changes of ulceration, bleeding and increase in size.
- Depending upon the clinical course and prognosis, cutaneous malignant melanomas are of 4 types.
- Lentigo maligna melanoma
- Superficial spreading melanoma
- Acral lentiginous melanoma
- Nodular melanoma.
- Malignant melanoma Spread: Metastatic spread in very common via lymphatics.
- Malignant melanoma Treatment: Surgery – main modality.
Palliative and supportive – other modalities.
Question 2. Carcinoma in situ
Answer: When the cytological features of malignancy are present but the malignant cells are confined to epithelium without invasion across the basement membrane, it is called as carcinoma in situ/intra epithelial neoplasia.
Common sites:
- Uterine cervix at the junction of ecto and endocervix
- Banen’s disease of the skin.
- Actinic/solar keratosis.
- Oral leukoplakia
- Interlobular and intraductal carcinoma of the breast.
- The area involved may be single and small/multifocal.
- It may return to normal/may develop into invasive cancer.
- In cervical cancer, there is sequential transformation from squamous metaplasia, to epithelial dysplasia, to carcinoma in situ and eventually in invasive cancer.
Question 3. Premalignant lesions
Answer:
Premalignant lesions Definition: Pre-malignant lesions is defined as morphologically altered tissue in which cancer is more likely to occur than its apparently normal counterparts
Premalignant lesions Examples:
- Leukoplakia
- Erythroplakia
- Mucosal changes associated with smoking habits
- Carcinoma in situ
- Bowen’s disease
- Actinic keratosis
Question 4. Sequestrum
Answer:
- Sequestrum is a fragment of dead tissue, usually bone, that has separated from healthy tissue as a result of injury or disease
- It is avascular
Sequestrum Types:
- Primary sequestrum
- A piece of dead bone that completely separates from sound bone during the process of necrosis
- Secondary sequestrum
- A piece of dead bone that is partially separated from sound bone during the process of necrosis but may be pushed back into position
Question 5. Osteoporosis
Answer: Osteoporosis is a common clinical syndrome involving multiple bones in which there is quantitative reduction of bone tissue mass
Osteoporosis Features:
- Common in elder people
- Increased risk of fractures occurs
- Causes pain and deformity
Osteoporosis Types:
- Primary osteoporosis
- Occurs without any underlying disease or medication
- Occurs due to the following factors
- Genetic factors
- Reduced physical activity
- Deficiency of sex hormones
- Combined deficiency of calcitonin and estrogen
- Secondary osteoporosis
- Occurs due to underlying diseases like
- Chronic anaemia
- Acromegaly
- Hepatic disease
- Hyperparathyroidism
- Occurs due to underlying diseases like
Question 6. Osteomyelitis
Answer:
Osteomyelitis Definition: An infection of bone that results in inflammation of bone involving the periosteum and haversian system is called osteomyelitis
Osteomyelitis Etiology:
- Odontogenic infections
- Traumatic injury
- Periostitis
- Hematogenous spread
Predisposing Factors:
- Conditions reducing host defences
- Diabetes
- Malnutrition
- Leukaemia
- Alcoholism
- Conditions compromising vascularity
- Radiation
- Paget’s disease
- Fibrous disease
- Malignancy
Question 7. Pyogenic Osteomyelitis
Answer:
- Pyogenic osteomyelitis is usually caused by bacterial infections
- It occurs most commonly in the long bones of infants and young children
Pyogenic Osteomyelitis Etiological Agents:
- Staphylococcus aureus
- E. coli
- Pseudomonas
- Klebsiella
- Anaerobes
Pyogenic Osteomyelitis Features:
- Painful and tender limb
- Fever
- Malaise
- Leucocytosis
- Draining sinus tract
Pyogenic Osteomyelitis Complications:
- Septicaemia
- Acute bacterial arthritis
- Pathologic fractures
- Development of squamous cell carcinoma
- Secondary amyloidosis
- Vertebral osteomyelitis
Question 8. Ewing’s sarcoma.
Answer: It is a malignant small round cell tumour
Ewing’s sarcoma Variants:
- Classic Ewing’s sarcoma
- Soft tissue Ewing’s sarcoma
- Primitive neuroectodermal tumour
Ewing’s Sarcoma Clinical Features:
- Age – Between 5-20 years
- Sex – Common in females
- Site-
- Shafts and metaphysis of long bones
- Flat bones such as the pelvis and scapula
- Presentation
- Pain, swelling, and tenderness of the affected area
- Fever
- Leucocytosis
- Elevated ESR