
Mandible Terminology
The word ‘mandible’ is derived from the Greek word ‘mandere’ which means to masticate or chew. The Latin word ‘mandibula’ means lower jaw.
Mandible Peculiarities
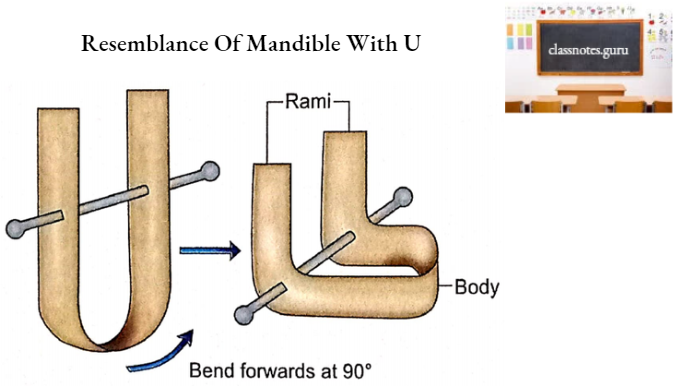
- It is a ‘U’ shaped bone.
- It is also called the ‘lower facial skeleton’.
- The mandible is the largest and strongest bone of the face.
- It forms the skeleton of the lower jaw.
Mandible Features And Attachments
The mandible has a body and two rami.
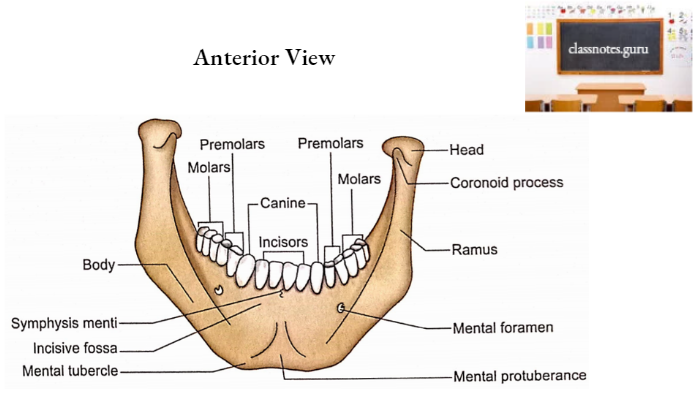
Mandible Body
It is shaped like a horseshoe and has 2 surfaces (external and internal) and 2 borders (upper and lower).
1. Surfaces
- External Surface
- It has the following features:
- Symphysis menti
- It is a faint ridge on the upper part of the midline indicating the fusion of two halves of the mandible.
- Mental protuberance
- It is a triangular area in the lower part of the midline. The upper angle of the triangle marks the lower end of symphysismenti.
- Mental tubercles
- The lower angles of the triangular mental protuberance are marked by tubercles called mental tubercles.
- Note: Remember that mental protuberance is characteristic of the human jaw.
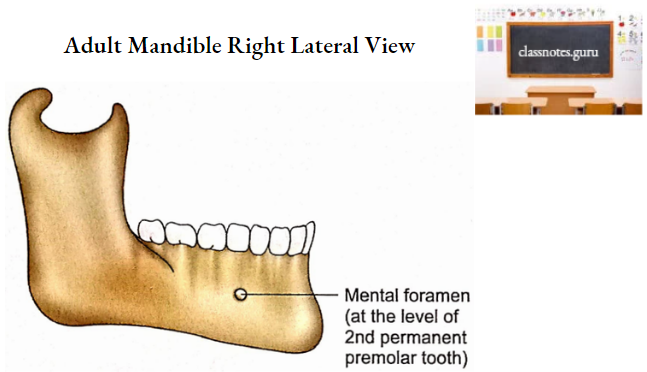
- Mental foramen
- It is located below the 2nd premolar or junction between two premolar teeth. Mental nerves and vessels pass through it.
- Incisive fossa
- It is a shallow fossa below the incisor teeth. Mentalis and orbicularis oris originate from this fossa.
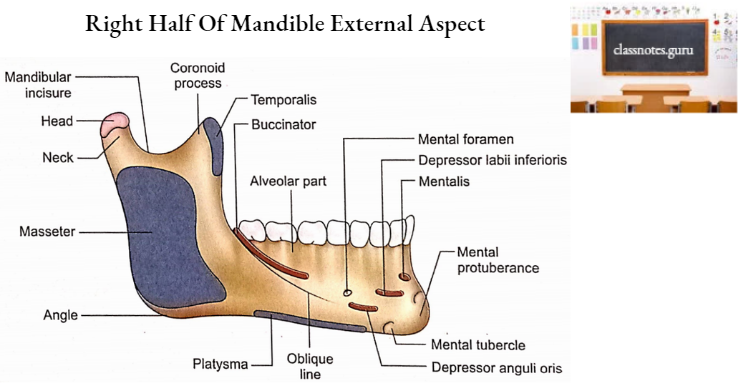
- Oblique line
- It is a continuation of the anterior border of the ramus on the external surface of the body. It is a faint ridge. It runs downwards and forwards to reach the mental tubercle. The following muscles are attached to it from anterior to posterior:
- Depressor labii inferioris.
- Depressor anguli oris.
- Buccinator (below the molar teeth).
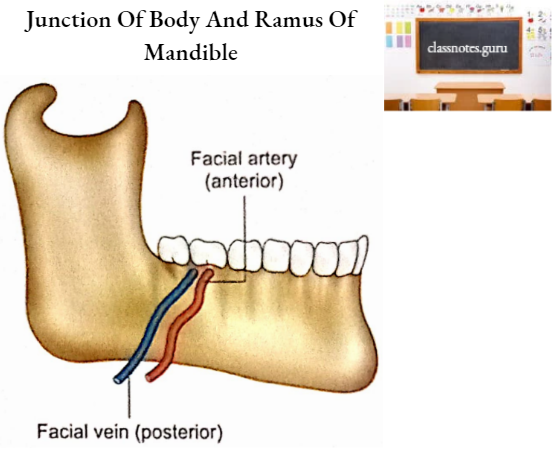
- Note: Junction of body and ramus is marked by the courses of facial artery and facial vein.
- It is a continuation of the anterior border of the ramus on the external surface of the body. It is a faint ridge. It runs downwards and forwards to reach the mental tubercle. The following muscles are attached to it from anterior to posterior:
- Symphysis menti
- Internal Surface
It has the following features:
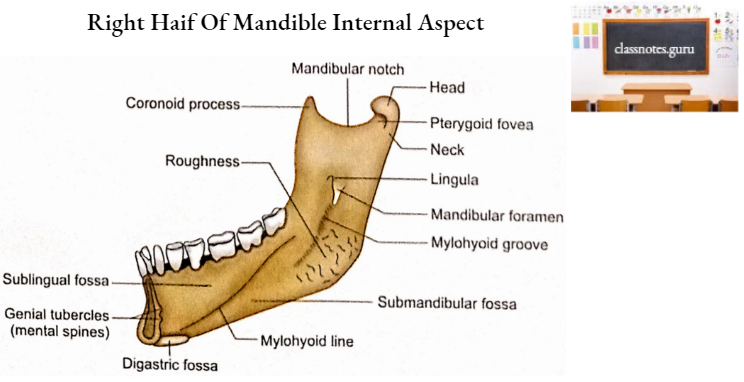
- Mylohyoid line
- It is an oblique ridge. It extends downwards and forwards from behind the 3rd molar tooth (1 cm below the alveolar border) to the midline near the lower border between digastric fossae. Mylohyoid muscle is attached to it.
- Submandibular fossa
- It is present below the posterior part of the mylohyoid line. It lodges the following structures:
- Submandibular salivary gland.
- Facial artery.
- Submandibular lymph nodes.
- It is present below the posterior part of the mylohyoid line. It lodges the following structures:
- Sublingual fossa
- It is an area above the anterior part of mylohyoid line. It lodges the sublingual salivary gland.
- Genial tubercles
- These are irregular elevations on either side of the midline just above the anterior ends of mylohyoid lines. Upper genial tubercle. provides attachment to the genioglossus muscle while the lower genial tubercle gives origin to the geniohyoid muscle.
- Note: Genial tubercles are for genial muscles, since the tongue is higher as compared to the hyoid bone, the upper tubercle is for genioglossus and the lower is for geniohyoid.
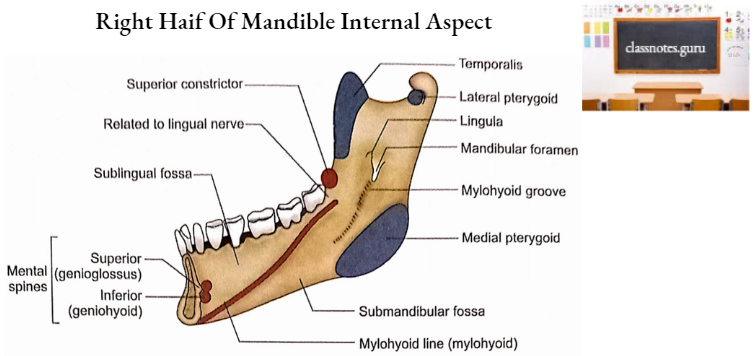
- Attachment of superior constrictor of pharynx
- The superior constrictor originates from the area above the posterior end of mylohyoid line.
- Attachment of pterygomandibular raphe
- This raphe is attached to the inner surface of the body in continuation with the origin of the superior constrictor just behind the 3rd molar tooth.
- Relation of lingual nerve
- The lingual nerve is related to the mandible between the origin of the superior constrictor and the posterior end of the mylohyoid line.
- Mylohyoid line
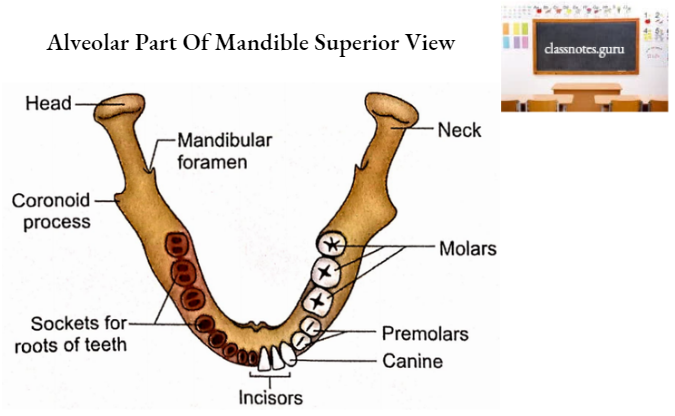
2. Borders
- Upper Border
- It is also called the alveolar part of the mandible.
- It is hollowed out by sixteen sockets for the roots of permanent teeth.
- The sockets vary in size and depth.
- The sockets may be single or subdivided by septa according to the teeth which they contain.
- Lower Border
- It is also called the base of the mandible.
- The digastric fossa is a depression at its anterior (mesial) end on each side of the
midline. It receives attachment of the anterior belly of the digastric. - The Investing layer of deep cervical fascia is attached to the whole length of the base.
- Platysma is inserted into the lower border near the outer surface.
Mandible Ramus
The Ramus of the mandible has 2 surfaces (lateral and medial), 4 borders (upper, lower, anterior and posterior) and two processes (coronoid and condylar).
1. Surfaces
- Lateral Surface
- A small posterosuperior area is related to the parotid gland.
- The remaining major area provides attachment to the masseter.
- Note: Remember, the house of the Prime Minister is located in the lateral area. P stands for Parotid and M stands for Masseter.
- Medial Surface
- Mandibular Foramen And Canal: The mandibular foramen is located a little above the centre of the medial surface. It leads into the mandibular canal which curves downwards and forwards into the body, to open on the external surface at the mental foramen. Inferior alveolar nerve and vessels enter the mandibular canal through the mandibular foramen.
- Lingula: It is a tongue-shaped projection near the anterior margin of the mandibular foramen. The sphenomandibular ligament is attached to the lingula.
- Mylohyoid Groove: It begins at the lower end of the mandibular foramen behind the lingula and continues downwards and forwards to reach the inner surface of the body. Mylohyoid nerve and vessels occupy the mylohyoid groove.
- The medial surface of the ramus between the mylohyoid groove and the angle of the mandible is marked by ridges. This area is meant for the attachment of the medial pterygoid.
- The area in front of the mylohyoid groove is related part (head) and a lower part (neck) to the lingual nerve.
2. Borders
- Upper Border
- It is thin.
- It forms a mandibular notch or incisure.
- Masseteric nerves and vessels cross the mandibular notch.
- Lower Border
- It is a backward continuation of the base of the mandible.
- It meets with the posterior border of the ramus to form the angle of the mandible.
- Anterior Border
- It is continuous above with the coronoid process and below with the alveolar border of the body.
- Temporalis muscle is inserted on this border and adjoining medial surface.
- Posterior Border
- It is continuous above with the condylar process.
- It meets with the lower border to form the angle of the mandible.
- It is related to the parotid gland.
3. Processes
- Coronoid Process
- It is a triangular upward projection from the anterosuperior part of the ramus.
- Its anterior border is continuous with the anterior border of the ramus and its posterior border bounds the mandibular notch.
- The Temporalis muscle gets inserted on the medial surface, apex and margins of the coronoid process.
- Condylar process
- It is an upward projection from the posterosuperior part of the ramus. It consists of an upper part (head) and a lower part (neck).
- Head
- It is side to side side-expanded part of the condylar process.
- It articulates with the temporal bone to form a temporomandibular joint.
- Neck
- It is a constricted part below the head.
- It provides attachment to the capsule in its upper part.
- The lateral ligament of the temporomandibular joint is attached to its lateral part.
- The pterygoid fovea is a depression in its anterior aspect. The lateral pterygoid muscle is inserted on the pterygoid fovea.
- Medially the neck is related to auriculo- temporal nerve above and the maxillary artery below.
Mandible Ossification
- Mandible is intramembranous as well as endochondral in origin.
- The membrane involved is the mesenchymal sheath on the lateral aspect of both Meckel’s cartilages. A centre appears on each side of this sheath during the 7th week of intrauterine life.
- Cartilages contributing to the mandible are as follows:
- Anterior ends of Meckel’s cartilage
- These are invaded by bone from parent centres at the 10th week of intrauterine life.
- Coronoid cartilages
- These appear at the 10th week of intrauterine life and disappear before birth.
- Condylar cartilages
- These appear at the 10th week of intrauterine life and persist till the 3rd decade.
- Cartilaginous nodules
- One or two of these nodules appear on each side of the symphysismenti at about the 10th week of intrauterine life. These ossify to form mental ossicles at about the 7th month of intrauterine life and fuse with the body at the age of one year.
- Anterior ends of Meckel’s cartilage
- Parts of the mandible which are derived from cartilage are:
- The incisive part below the incisor teeth.
- Coronoid and condylar processes.
- Part of ramus above the mandibular foramen.
- Note: Remember that the names of all the parts of the mandible which ossify from cartilage start with C, i.e. coronoid process, condylar process, cranial part of ramus and chin part of body related to cutting or incisor teeth.
- At birth, the mandible consists of two halves connected at symphysis menti. Bony union starts from below upwards during 1st year of age and is completed at the end of 3rd year.
Age Changes In Mandible
Some of the differentiating features in different age groups are as follows:
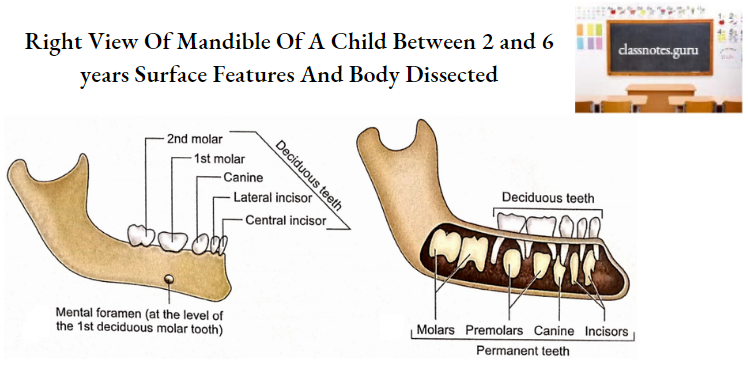
1. Children
- The body of the mandible is more like a shell having sockets for both deciduous and permanent teeth.
- The angle of the mandible measures about 140°.
- The coronoid process is above the level of the condylar process.
- The mandibular canal and mental foramen are close to the lower border of the body.
2. Adult
- The alveolar and subalveolar parts of the body are of equal depths.
- The angle of the mandible measures about 110°.
- The condylar process projects above the level of the coronoid process.
- The mandibular canal runs parallel to the mylohyoid line.
- The mental foramen is situated midway between the upper and lower borders of the body.
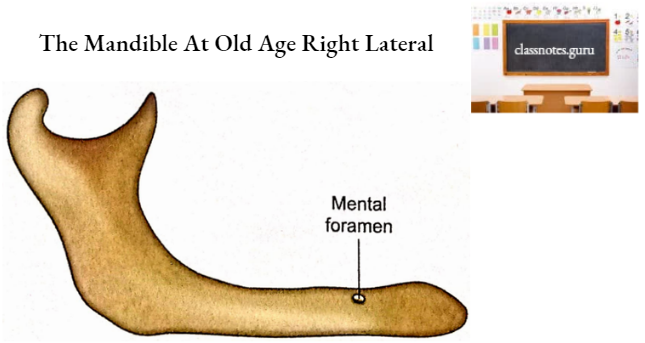
3. Old age
- Loss of teeth is a usual feature.
- The alveolar part is absorbed.
- The angle of the mandible measures about 140°
- The neck of the mandible is bent backwards making the level of the coronoid process higher than the condylar process.
- The mandibular canal and mental foramen are close to the upper border of the body.
Mandible Applied Anatomy
1. The mandible occupies a prominent and exposed position in the facial skeleton and, therefore, forms a common site of violent injuries.
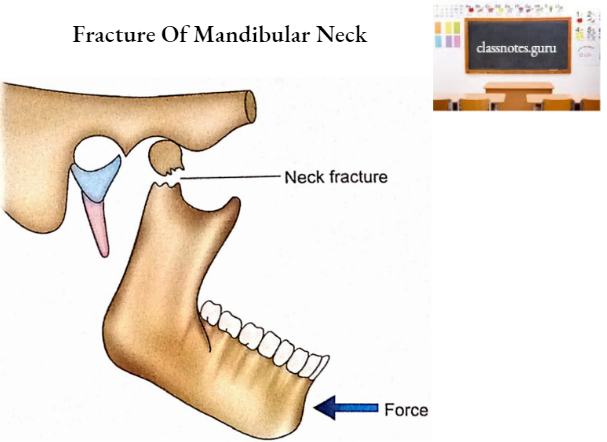
2. The slender neck of the mandible is liable to fracture as a result of violence received at the mental prominence.
3. The alveolar process is weaker than the rest of the mandible and, therefore, an independent alveolar fracture may occur.
4. The tendency of the mandible to fracture with advancing age is due to resorption of the alveolar portion of bone when the teeth are lost.
5. The elongated root of the canine tooth reduces the bony substance and makes the mandible weaker at this site. The canine region is, therefore, the commonest site of fracture.
6. Thick periosteum over the mandible prevents gross displacement of fractured bones after fracture.
7. Impacted 3rd molar, mental foramen and missing teeth also contribute to the weakness in the mandible.
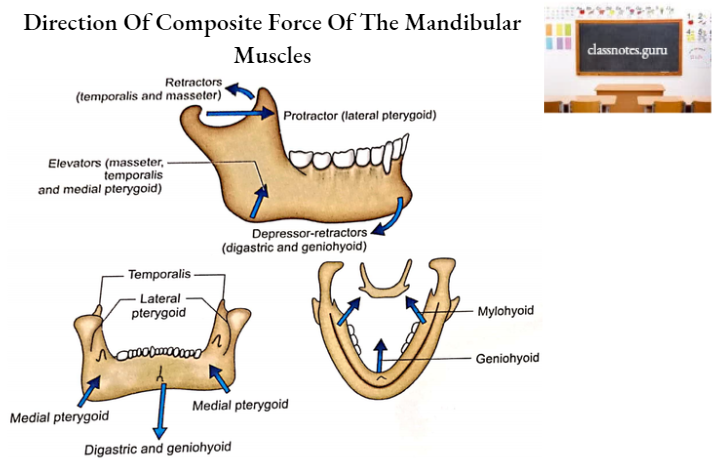
8. Strong muscles attached to the mandible play a very important role in the displacement of fractured segments of the mandible. Such muscles are divided into 3 groups.
- The depressor group
- It includes geniohyoid and digastric muscles. They cause posterior and inferior displacement of a fractured anterior mandibular segment.
- The elevator group
- The masseter, temporalis and medial pterygoid muscles belong to this group. Contraction of these muscles causes upward displacement of the fractured segment if the fracture occurs in the region of the angle.
- The protrusion group
- It includes lateral pterygoid muscle which causes forward displacement of the head in cases of fracture of the mandibular neck.
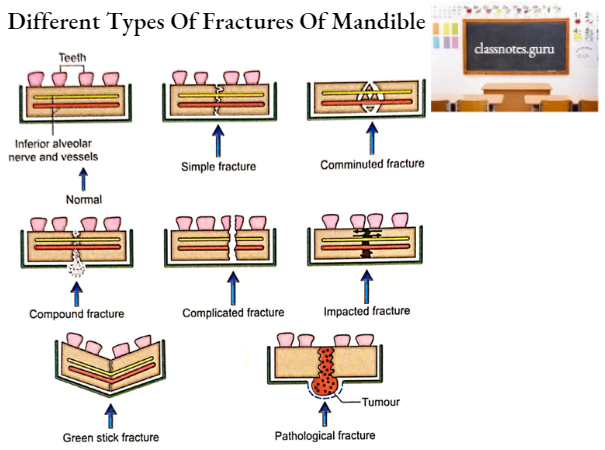
9. The following is the general classification of mandibular fractures:
- Simple
- Single fracture without exposure to exterior.
- Compound
- The fractured site is exposed to the exterior.
- Comminuted
- It is multiple fractures of the mandible at the same site. It may be both simple and compound.
- Complicated
- It is a fracture associated with injury of teeth, nerves or vessels.
- Impacted
- In this fracture, one fragment has been driven into the substance of another fragment.
- Greenstick
- In this fractured site bends without displacement.
- Pathological
- Fracture is due to underlying diseases like osteomyelitis or tumours.
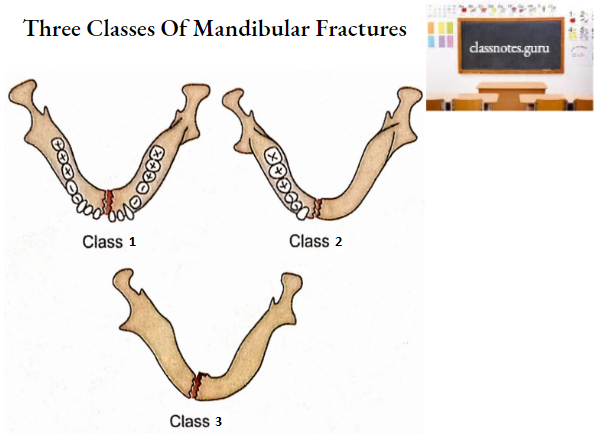
10. Clinical classification of mandibular fractures.
- Class 1
- Teeth are present on both sides of the fractured line.
- Class 2
- Teeth are present on one side of the fractured line.
- Class 3
- Fragments are edentulous (without teeth)
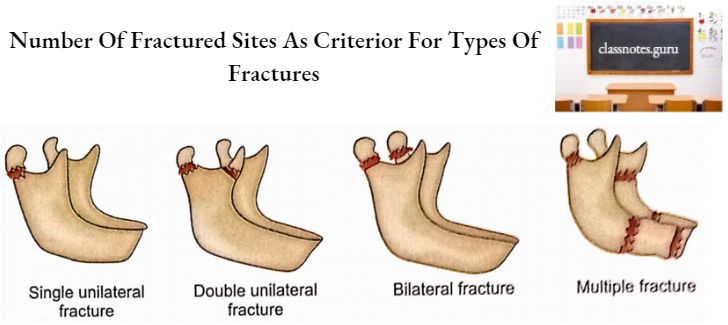
11. Depending upon the number of sites, mandibular fractures may be of the following types:
- Single unilateral
- Double unilateral
- Bilateral
- Multiple
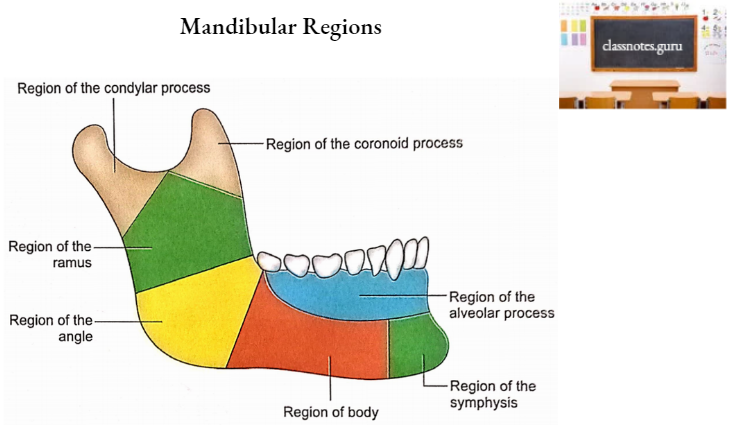
12. The mandible can be divided into the following regions to simplify the sites of lesions, for example. fractures:
- Condylar
- Coronoid
- Ramus
- Angle
- Alveolar.
- Body.
- Symphysis.
13. Tumours of the hard tissue of the lower jaw can originate in teeth (odontogenic tumours) or mandible (osteogenic tumours)
- Odontogenic Tumours
- These can be of the following two types:
- Odontoma
- Arising from teeth proper. Odontomas may be of the following three types according to their structures:
- Calcified odontoma
- It has dentine.
- Simple enamel pearl.
- It has enamel.
- Cementoma
- It has cementum.
- Calcified odontoma
- Ameloblastoma
- Arising from the embryonal (ameloblast) cells of developing teeth.
- Osteogenic Tumours
- The following are the common osteogenic tumours:
- Osteoma
- Fibro-osteoma
- Myxoma
- Chondroma
- Sarcoma
- Ewing’s tumour
- Multiple myeloma.
- Central giant cell tumour