Vertebrae
Vertebrae General Considerations
- The vertebral column is made up of a number of irregular bones called vertebrae.
- The vertebral column forms the central axis of the body.
- There are 33 vertebrae.
- Vertebrae are named according to the regions they belong to.
- Following is the classification of vertebrae:
- Cervical vertebrae – 7
- Thoracic vertebrae – 12
- Lumbar vertebrae – 5
- Sacral vertebrae – 5 (these fuse to form a single sacrum)
- Coccygeal vertebrae – 4 (these fuse to form a single coccyx)
- Vertebrae are mobile or fixed.
- Mobile vertebrae are called true vertebrae while fixed vertebrae are called false vertebrae.
- Movable vertebrae are cervical, thoracic, and lumbar.
- Sacral and coccygeal vertebrae are immobile.
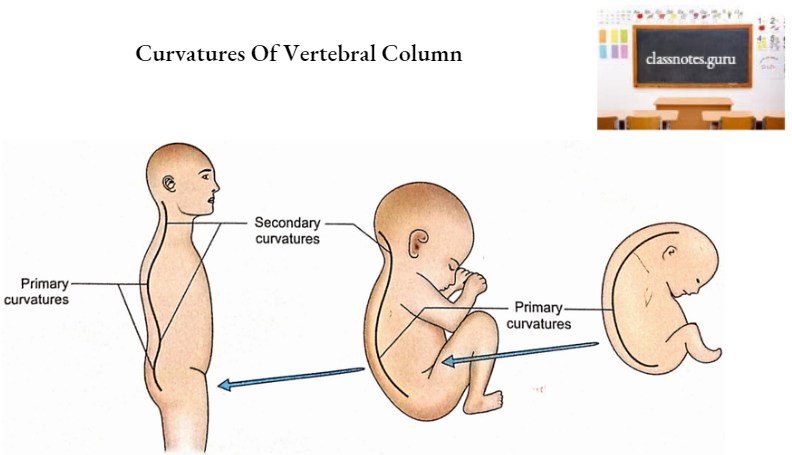
Curvatures Of Vertebral Column
1. Primary Curvatures
- During intrauterine life, the whole vertebral column is concave ventrally and convex dorsally. This is primary curvature.
- In adults, primary curvatures are retained only in thoracic and sacral regions.
- These are mainly due to the shape of vertebrae.
2. Secondary Curvatures
- Secondary curvatures are convex forwards.
- These develop after birth.
- These develop due to posture.
- These are mainly due to the shape of intervertebral discs.
- Secondary curvatures are observed in cervical and lumbar regions.
- Cervical curvature appears around 6 – 9 months when the child starts holding his head by himself.
- Lumbar curvature appears at about 12 – 18 months when the child starts walking.
Movements Of Vertebral Column
The vertebral column shows the following movements:
- Flexion: Forward bending.
- Extension: Backward bending.
- Lateral flexion: Side bending.
- Rotation: Twisting of the trunk.
- Circumduction: Combination of all the above movements.
Features Of A Typical Vertebra
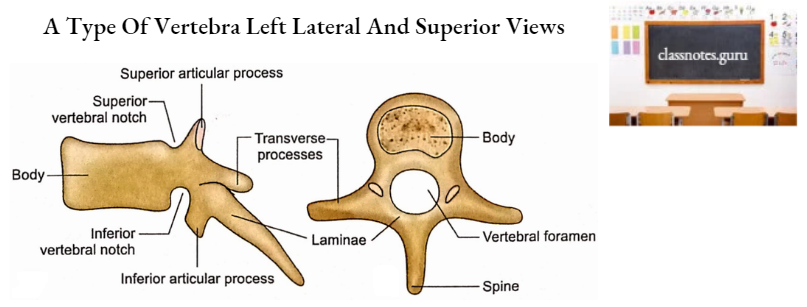
A typical vertebra is made up of 2 parts, the body and the vertebral arch.
1. Body
- It is the ventral part of a vertebra.
- It is cylindrical in shape.
- It has four surfaces, anterior, posterior, superior, and inferior.
- The anterior surface is convex from side to side and concave from above downwards.
- The posterior surface is slightly concave from side to side but flat from above downwards. It has a number of foramina for the exit of basivertebral veins. It forms the anterior boundary of the vertebral foramen.
- The upper and lower surfaces are rough for the intervertebral discs.
2. Vertebral Arch
It consists of a pair of pedicles, a pair of laminae, and seven processes (one spinous, four articular, and two transverse).
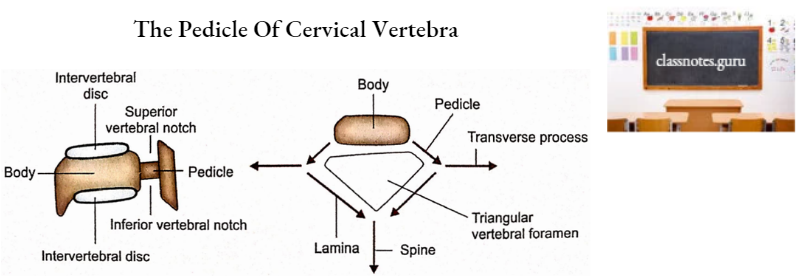
- Pedicles
- These are pairs of short thick processes that project backward from the body.
- Between the adjacent pedicles are intervertebral foramina.
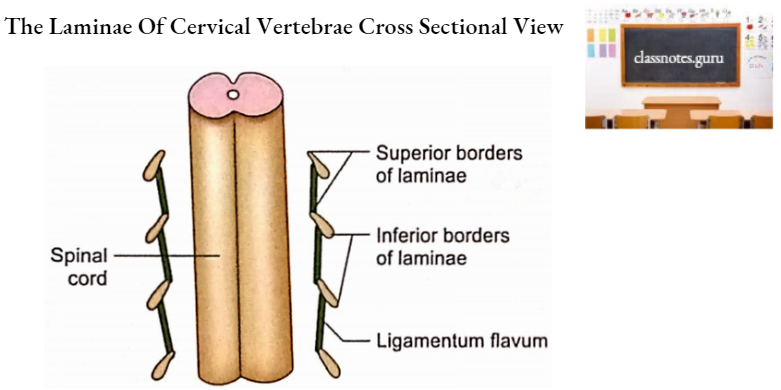
- Laminae
- These are bony plates extending backward and medially from the posterior end of the pedicles.
- Posteriorly they fuse to form a spine in the midline.
- The body, pedicles, and laminae together enclose the foramen of the vertebra called the vertebral foramen.
- Transverse Process
- It projects laterally on each side from the junction of the pedicle and lamina.
- Articular Processes
- There are two on each side and four in total.
- These are superior and inferior articular processes projecting upwards and downwards respectively from the junction of the pedicle and lamina.
- Spinous Process (Spine)
- It projects backward in the midline from the meeting point of the laminae.
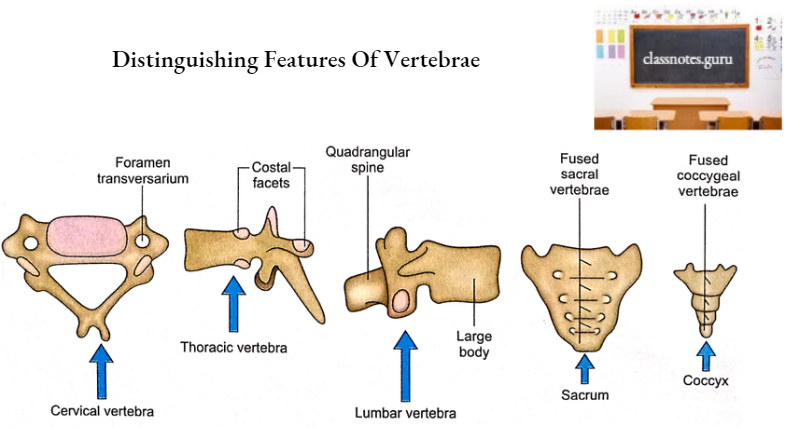
Distinguishing Features
- The cervical vertebra is characterized by the presence of a foramen in each transverse process. This foramen is named as foramen transversarium.
- The thoracic vertebra is recognized by the presence of costal facets on the sides of the body.
- The Lumbar vertebra is larger in size and lacks both foramen transversarium as well as costal facets.
- There is no isolated sacral vertebra. Five sacral vertebrae fuse to form a single piece of triangular and curved sacrum.
- Similarly, there is no isolated coccygeal vertebra. Four coccygeal vertebrae fuse to form a single piece of coccyx. The coccyx is relatively much smaller in size than the sacrum.
Regional Vertebrae Cervical Vertebrae
These are classified as typical and atypical. 3rd to 6th cervical vertebrae are typical. 1st, 2nd and 7th cervical vertebrae are atypical.
1. Typical Cervical Vertebra
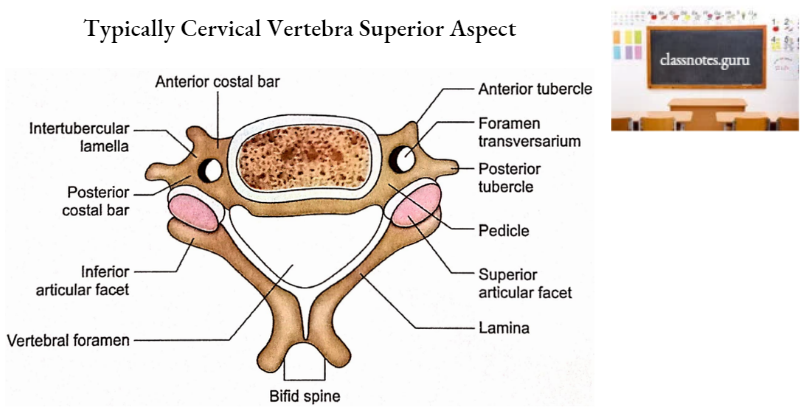
It has a body and a vertebral arch. These enclose a vertebral foramen.
- Body
- It is the smallest among all vertebrae.
- It is narrower anteroposteriorly.
- It has 4 surfaces; superior, inferior, anterior, and posterior.
- Its superior surface is concave from side to side with an upward projecting lip on either side. This surface is mainly related to the intervertebral disc.
- The inferior surface is convex from side to side. The anterior border of the inferior surface projects downwards to hide the intervertebral disc. The inferior surface, like the superior surface, is also related to the intervertebral disc.
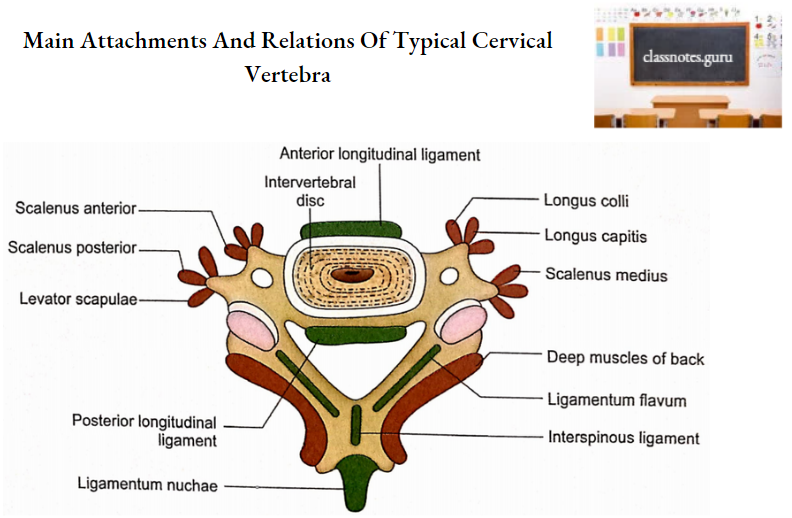
- The anterior surface provides attachments to an anterior longitudinal ligament in the middle and longus colli muscle on either side of it.
- The posterior surface has a number of foramina for basivertebral veins. Its superior and inferior margins provide attachments to the posterior longitudinal ligament.
- Vertebral Foramen
- It is triangular in shape.
- It is bigger than the body.
- Vertebral Arch
- It is comprised of pedicles, laminae, the superior and inferior articular processes, the transverse processes, and the spine.
- Pedicles
- These are directed backward and laterally. It is this direction which is responsible for the triangular shape of the vertebral foramen.
- Above and below the pedicles are superior and inferior vertebral notches respectively. These notches are equal in size.
- Laminae
- These are long and narrow.
- The superior border is thinner than the inferior border.
- Ligamentum flavum is attached to its superior border and the lower part of its anterior surface.
- Articular Processes
- Superior and inferior articular processes are located on each side, above and below the junction of the pedicle and lamina.
- Superior articular process faces upwards and backward.
- The inferior articular process is directed downwards and forwards.
- The superior articular process of a vertebra articulates with the inferior articular process of the vertebra above.
- Articular processes lie in one line forming an articular pillar.
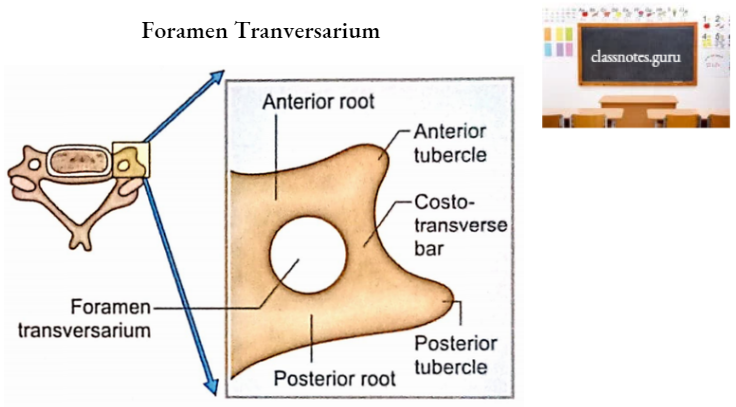
- Transverse process
- It has a foramen called foramen transversarium, which forms a characteristic feature of the cervical vertebra.
- The vertebral artery, vertebral vein, and sympathetic nerves pass through the foramen transversarium (vertebral artery passes through upper 6 foramina only).
- The foramen transversarium is bounded anteriorly and posteriorly by anterior and posterior roots respectively.
- The lateral ends of the anterior and posterior roots are connected by the costotransverse bar or intertubercular lamella.
- Junctions of anterior and posterior roots with costotransverse bars are marked by anterior and posterior tubercles respectively.
- The enlarged anterior tubercle of the sixth cervical vertebra is called the carotid tubercle. This is related to the common carotid artery.
- Anterior tubercles give origins to scalenus anterior, longus capitis and longus colli muscles.
- Posterior tubercles provide attachments to levator scapulae, scalenus medius, scalenus posterior, and some deep muscles of the back.
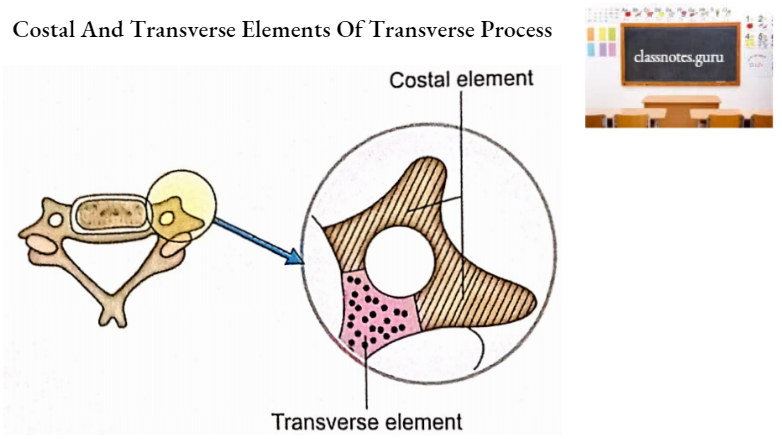
- The anterior root, anterior tubercle, costotransverse bar, posterior tubercle, and adjoining (lateral part of) posterior root represent the costal element while the medial part of the posterior root represents the transverse element of the developing vertebra.
- Spine
- It is small and bifid.
- Ligamentum nuchae is attached to the spinous notch.
- Interspinous ligaments are attached to their superior and inferior borders.
- Sides provide attachments to deep muscles of the back.
2. Atypical Vervical Vertebrae
First Cervical Vertebra Terminology
It is also named an atlas because it supports the skull. According to Greek mythology, Atlas is the God who supported the earth on his shoulders.
Distinguishing Features
- It is ring-shaped with narrow anterior and posterior arches.
- It has nobody.
- It has no spine.
- It has a large lateral mass on either side.
- The two transverse processes are widest apart relative to other cervical vertebrae.
Normal Anatomical Position
- Two arches lie in the same horizontal plane.
- The anterior arch is smaller than the posterior arch.
- Superior articular facets on lateral masses are elongated.
Features And Attachments
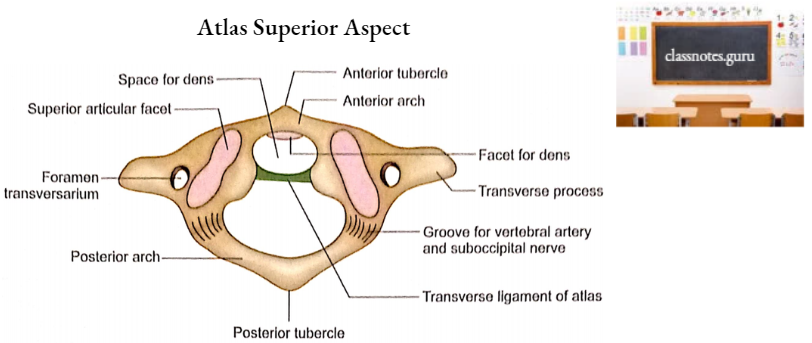
Atlas has an anterior arch, a posterior arch, and two lateral masses.
- Anterior Arch
- It is smaller than the posterior arch.
- It connects the two lateral masses.
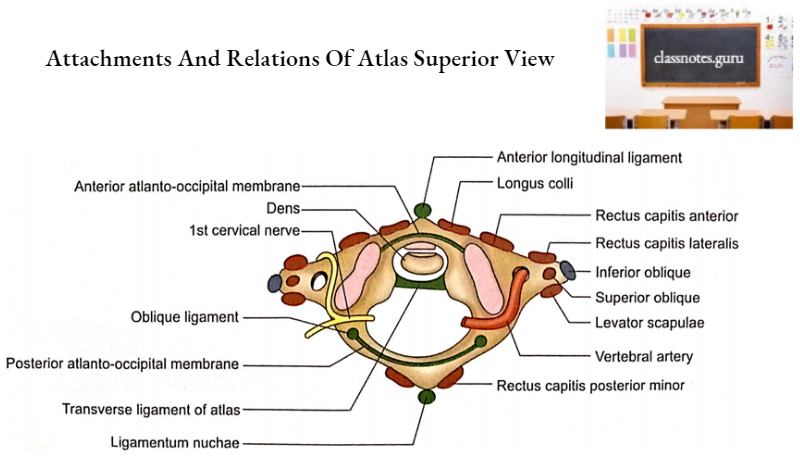
- The anterior tubercle is present on its anterior aspect in the midline. The midline part of the upper end of the anterior longitudinal ligament is attached to it.
- Its anterior surface on each side of the anterior tubercle provides attachment to longus colli muscle.
- An oval facet is present on its posterior surface in the midline for articulation with dens of the 2nd cervical vertebra to form the atlantoaxial joint.
- The anterior atlantooccipital membrane is attached to the upper border of the anterior arch.
- The lateral part of the upper end of the anterior longitudinal ligament is attached to the lower border of the anterior arch.
- Posterior Arch
- It is longer than the anterior arch.
- The midline posterior tubercle on its posterior surface represents the spine.
- The Ligamentum nuchae is attached to the posterior tubercle.
- On each side of the posterior tubercle is attached the rectus capitis posterior minor.
- The vertebral artery (3rd part) and first cervical nerve lie in the shallow groove on the superior surface of the posterior arch just behind the lateral mass.
- The posterior atlanto-occipital membrane is attached to the superior border behind the grooves.
- Ligamentum flavum is attached to its lower border on each side of the midline.
- Lateral Masses
- Each lateral mass has two articular facets (superior and inferior), two surfaces (anterior and medial), and a transverse process.
- The superior articular facet is concave and elongated. It articulates with the occipital condyle from the atlanto-occipital joint.
- Note: Remember, we say ‘No’ at the atlantoaxial joint, i.e. move the head from side to side while we say ‘Yes’ at the atlantooccipital joint, i.e. perform nodding movement of the head.
- The inferior articular facet is flat and circular. It articulates with an axis.
- The medial surface has a tubercle for the transverse ligament of the atlas.
- The anterior surface gives origin to the rectus capitis anterior.
- The transverse process is long and strong. It has foramen transversarium which transmits vertebral artery, vertebral vein, and sympathetic nerve.
- Rectus capitis lateralis, levator scapulae, and superior oblique muscles are attached to its superior aspect around the foramen transversarium.
- The inferior oblique muscle is attached to its inferior surface. The anterior aspect of the transverse process is related to the ventral ramus of 1st cervical nerve and accessory nerve.
Second Cervical Vertebra
Terminology
It is also called an axis because the atlas carrying the skull rotates on it.
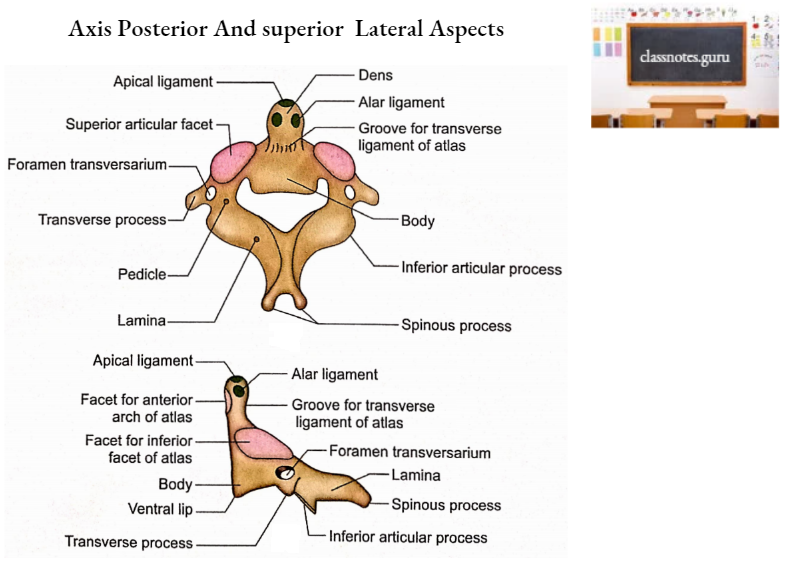
Peculiarities
- It is the strongest of the cervical vertebrae.
- It is easily identified by the presence of an odontoid process (dens) which is a strong tooth-like projection from the superior surface of the body.
Features And Attachments
- Body And Odontoid Process
- The apex of the odontoid process gives attachment to the apical ligament.
- On each side of the apex, the sloping gives attachment to the alar ligament.
- The anterior surface of the odontoid process possesses an oval facet for articulation with the anterior arch of the atlas.
- The posterior surface of the odontoid process is grooved to lodge the transverse ligament of the atlas.
- The inferior surface of the body is related to the intervertebral disc.
- The anterior surface of the body gives attachments to the anterior longitudinal ligament in the midline and longus colli muscle on each side.
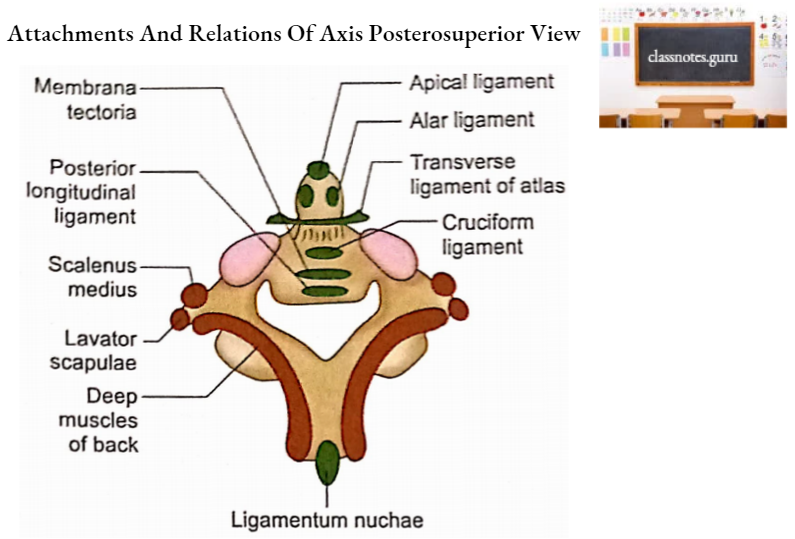
- The posterior surface of the body provides attachments to the following three structures from above downwards:
- The lower vertical limb of the cruciform ligament.
- Membrana tectoria.
- Posterior longitudinal ligament.
- The superior articular facet (for articulation with the inferior facet of the atlas) is situated lateral to the odontoid process, partly over the body and partly on the pedicle.
- Vertebral Arch
- The pedicle passes backward from the upper part of the body.
- The superior articular facet is large, flat, and circular. It is directed upwards and laterally.
- The inferior articular facet is situated posterior to the transverse process and is directed downwards and forwards.
- The spine is short, thick, and strong. Its tip is bifid and receives attachment of ligamentum nuchae.
- Ligamentum flavum is attached to the superior border and lower part of the anterior surface of the lamina on each side.
- The side of the spine provides attachment to rectus capitis posterior major.
- The external surface of the lamina is meant for the attachment of the inferior oblique in its upper part and the deep muscles of the back in its lower part.
- Transverse processes are very small. They represent the true posterior tubercles
only. - The tip of the transverse process receives attachments of the following 3 muscles from anterior to posterior:
- Scalenus medius
- Levator scapulae
- Deep muscles of the back
Seventh Cervical Vertebra
Terminology
It is also called vertebra prominent because it has a very long spine which may be palpated under the skin of the lower part of the back of the neck.
Peculiarities
- The spine is long, horizontal, and nonbifid.
- The transverse process is large with a prominent posterior tubercle.
- Foramen transversarium is smaller and sometimes may be absent.
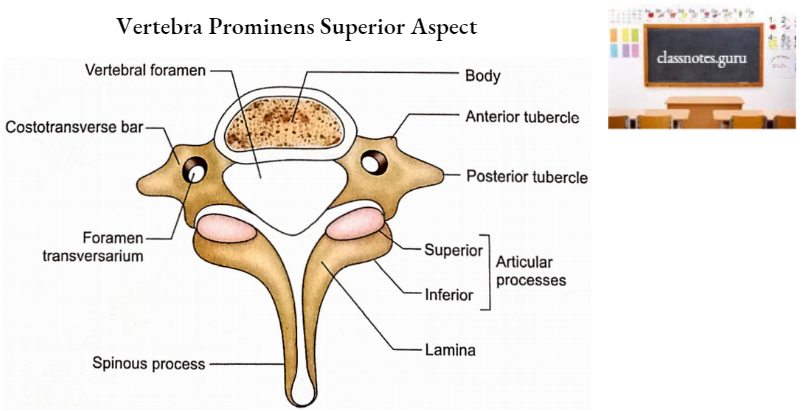
Important Attachments And Relations
- The spine provides attachments to ligamentum nuchae, trapezius, rhomboids minor, and deep muscles of the back.
- The posterior tubercle of the transverse process receives attachments of the suprapleural membrane and scalenus minimus.
- Foramen transversarium transmits an accessory vertebral vein.
- Note: The vertebral artery occupies the foramina transversal of the upper 6 cervical vertebrae only
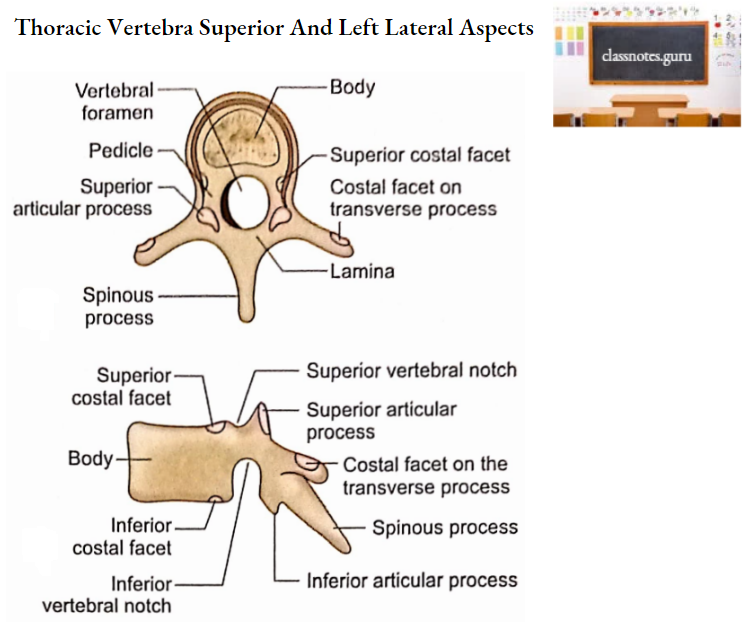
Thoracic Vertebrae
There are 12 thoracic vertebrae.
Peculiarities
- Articular facets are present by the side of the body and in front of transverse processes.
- The body is heart-shaped.
- Vertebral foramen is circular.
- The spinous process is long, pointed, and directed. downwards.
- The pedicle is attached to the upper part of the body making the inferior vertebral notch deeper.
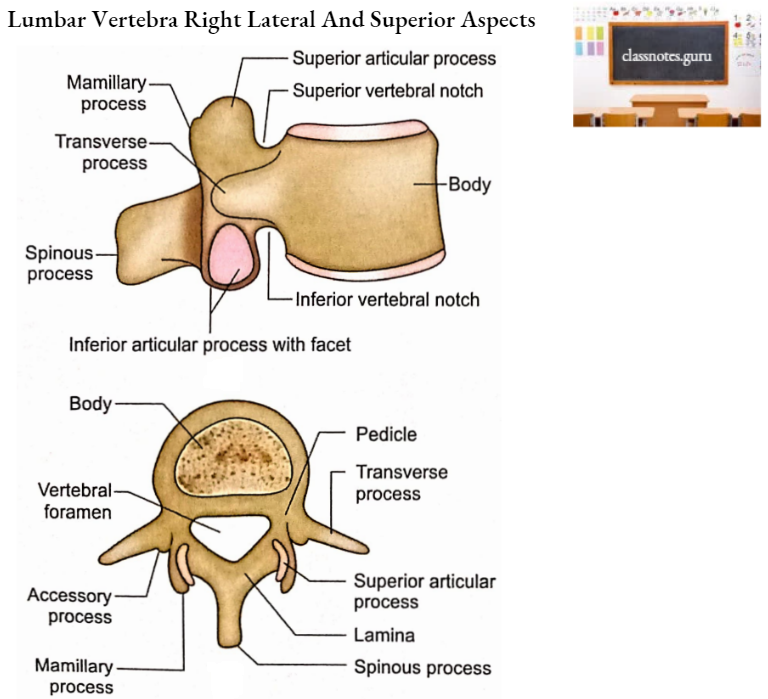
Lumbar Vertebrae
There are 5 lumbar vertebrae.
Peculiarities
- A lumbar vertebra has a massive body.
- Vertebral foramen is triangular.
- Spine is quadrangular.
- The superior articular facet is concave.
- The inferior articular facet is convex.
- The posterior part of the root of the transverse process has a rough elevation called the accessory process.
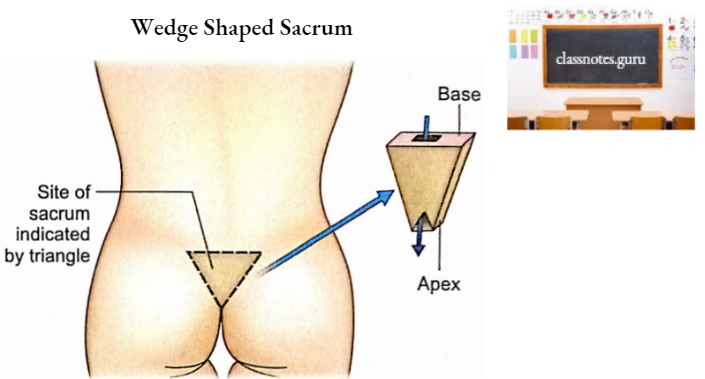
Sacrum
General Form
The sacrum is a wedge-shaped triangular bone. The base of the wedge is superior and forms the base of the sacrum. The edge of the wedge forms the inferior apex.
It has 4 surfaces, pelvic (anterior), dorsal (posterior), and 2 lateral. The canal of the sacrum is called the sacral canal.
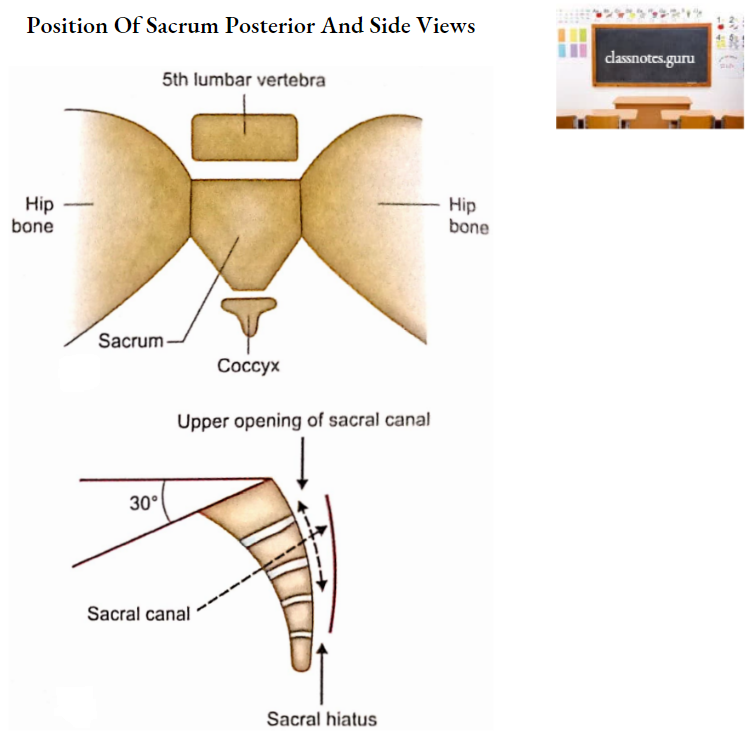
Anatomical Position
- The sacrum is a midline bone placed between hip bones (on each side), the 5th lumbar vertebra (superiorly), and the coccyx (inferiorly).
- The superior surface of the body of 1st sacral vertebra slopes forward at an angle of 30°.
- The anterior surface of the sacrum faces downwards and forwards.
- The upper end of the sacral canal is directed upwards.
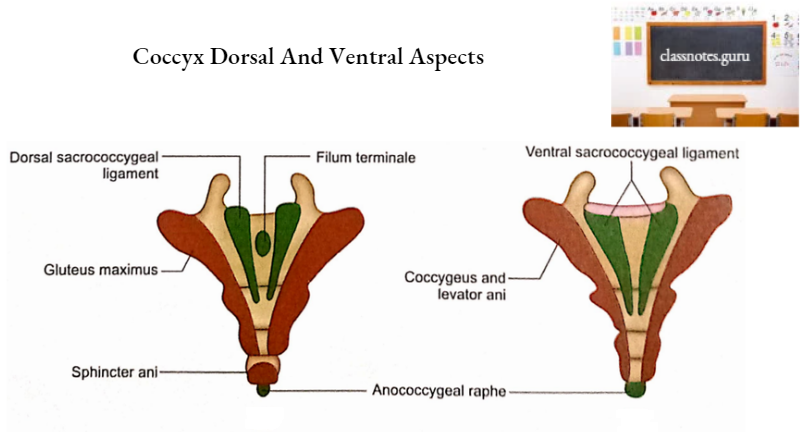
Coccyx
Normal Anatomical Position
Coccyx is directed downwards and forwards.
Features
A coccyx is formed by the fusion of four coccygeal vertebrae. It is triangular in shape. with the base upwards and apex downwards. It has two surfaces (pelvic and dorsal) and two lateral borders (right and left).