Oral Medicine Tumours Important Notes
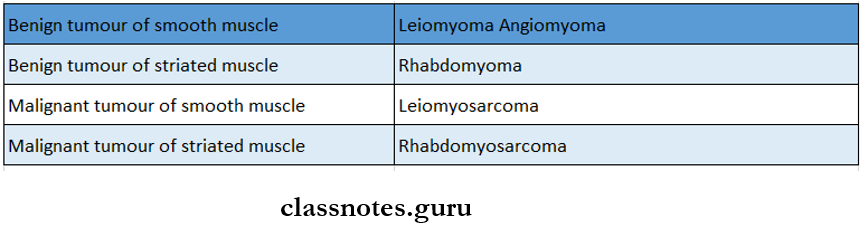
1. Tumours Of Muscles
2. Features Of Epithelial Dysplasia
- Increased abnormal mitosis
- Individual cell keratinization
- Epithelial pearls in the spinous layer
- Alterations in nuclear cytoplasm ratio
- Loss of polarity and disorientation of cells
- Hyperchromatism
- Large nucleoli
- Poikilokarynosis
- Basilar hyperplasia
3. Burkitt’s Lymphoma
- It is a B cell neoplasm
- Commonly affects children between 214 years of age
- Macrophages are found uniformly throughout the tumour producing the starring sky effect
Read And Learn More: Oral Medicine Question and Answers
4. Basal Cell Carcinoma
- Involves the exposed surfaces of skin mostly the middle third of the face
- Does not tend metastasize
- UV light is the main etiological agent
- Men are commonly affected
5. Histological Features Of Squamous Cell Carcinoma
- Enlarged nuclei
- Increased nuclear/ cytoplasmic ratio
- Hyperchromatic nuclei
- Dyskeratosis
- Increased mitotic activity
6. Teratoma
- It is made up of some different types of tissue which are not native to the area
- Occurs in various parts of the body
- Made up of various epithelial appendages such as hair, sweat glands, sebaceous glands, and salivary glands
- Teeth are usually normal
- Inflammatory gingivitis may be seen
7. Syndromes Associated With Haemangioma
- RenduoslerWeber syndrome
- SturgeWeber syndrome
- KasabachMerritt syndrome
8. Odontogenic Tumors And Their Common Sites
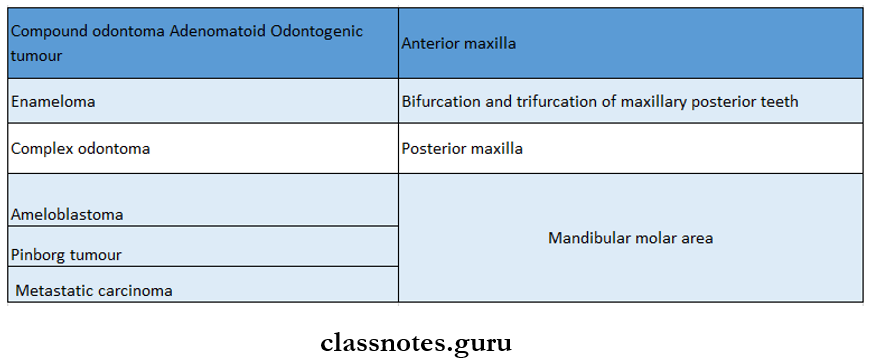
9. Odontoma
- It has two types
- Resembles normal tooth
- Affects anterior maxilla
- Complex odontoma
- Has no morphological similarity
- Affects posterior maxilla
10. Sunray Appearance Is seen in
- Osteogenic sarcoma
- Central hemangioma
- Ewing’s sarcoma
11. Onion Peel Appearance in
- Ewing’s sarcoma
- Garre’s osteomyelitis
- Caffey’s disease
12. Russell’s body is seen in
- Multiple myeloma
- Periapical granuloma
Oral Medicine Tumours Long Essays
Question 1. Give differences between benign and malignant tumors. Describe clinical features and radio¬graphic features of squamous cell carcinoma
Answer:
Differences between benign and malignant tumors
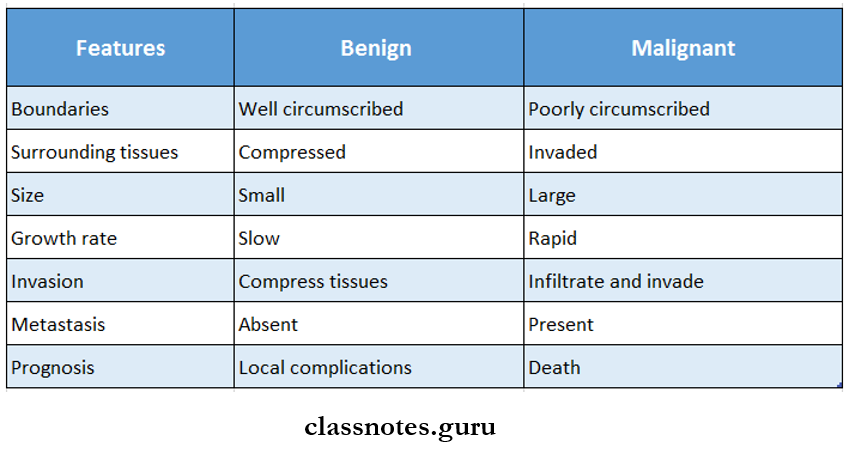
Benign and Malignant Tumors Clinical Features:
- Age and sex: It is common in older men
- Sites: sites involved in their order are
- Lower lip
- Lateral tongue
- The floor of the mouth
- Soft palate
- Gingiva
- Alveolar ridge
- Buccal mucosa
Benign and Malignant Tumors Presentation:
- Initially, it is an asymptomatic lesion
- It may resemble leukoplakia or erythroplakia
- It appears as a white or red nodule or fissure over the mucosa
- The advanced lesion appears as a rapidly enlarging exophytic growth or ulcer or tumor-like mass
- The ulcer has persistent induration around the periph¬ery with elevated and everted margins
- It may predispose to candidal infections
- It may be secondarily infected
- There is a presence of regional lymphadenopathy
- Pathological fractures of jawbones may sometimes occur
- Maxillary lesions may lead to nasal bleeding and pressure sensation over the eyeball
- Involvement of the inferior alveolar nerve leads to parties these of lower teeth and lip
Benign and Malignant Tumors – Radiographic Features:
- The involved bone exhibits large, irregular, and ill-defined borders in radiolucent areas
- It gives a typical moth-eaten appearance
- There is the destruction of interdental bone
- It causes exfoliation or displacement of regional teeth
Oral Medicine Tumours Short Answers
Question 1. Odontomes.
Answer:
Odontomes
Common hamartomatous odontogenic lesions with limited growth potential
Odontomes Types:
1. Comple Odontoma:
- Consists of a mass of haphazardly arranged enamel, dentin, and cementum
2. Compound odontoma:
- Consists of collections of numerous small, discrete, tooth-like structures
Odontomes Clinical Features:
- Age: Children and young adults
- Sex: Both
- Site: Compound in the maxilla
- Complex mandible
Odontomes Presentation:
- Small asymptomatic lesion
- Expansion of cortical plates
- Displacement of teeth
- Impacted or retained deciduous teeth
- Pain, inflammation
- Ulceration
- Fistula formation
Odontomes Radiographic Features:
- Compound A bag of teeth appearance
- Complex sunburst appearance
Odontomes Treatment:
Question 2. Keratoacanthoma.
Answer:
Keratoacanthoma
- Keratoacanthoma is a benign endophytic epithelial tissue neoplasm, which commonly occurs in the sun-exposed skin of the face and it usually appears as a circumscribed keratin-filled crater
Keratoacanthoma Features:
- It appears as a small, well-circumscribed, elevated, and crater-like lesion with a central depression
- It initiates as a small lump or bud-like growth on the sun-exposed skin surface of the face
- It grows rapidly and achieves its maximum size over about 48 weeks
- It reveals a well-circumscribed, elevated nodule that has a sharply delineated, rolled margin and a central keratotic core
- It is often painful
- It may have associated lymphadenopathy
Keratoacanthoma Treatment:
- Surgical excision of the lesion is done
Question 3. Papilloma
Answer:
Papilloma
- Papilloma is a common benign neoplasm of the oral cavity arising from epithelial tissue
- It is characterized by exophytic growth with a typical cauliflower-like appearance
Papilloma Clinical Features:
- Age third, fourth, and fifth decade of life
- Sex both sexes are equally affected
- Site involved
- Tongue
- Lips
- Buccal mucosa
- Gingiva
- Hard and soft palate
- Present as slow-growing, exophytic, soft, pedunculated, painless, nodular growth with a cauliflower-like appearance
- Have numerous fingerlike projections over the surface
- It appears as ovoid swelling with a corrugated surface
- Size a few mm to 1 cm in diameter
- The base of the lesion may be pedunculated or sessile
- The color white in color
- Surface highly keratinized
- Superficial ulceration and secondary infection occur
- Rarely papilloma grows inward
Question 4. Osteosarcoma.
Answer:
Osteosarcoma
- Osteosarcoma is a highly malignant primary neoplasm arising from the bone
Osteosarcoma Types:
1. According To The Location Of The Lesion
- Medullary osteosarcoma
- Periosteal osteosarcoma
- Parosteal osteosarcoma
- Soft tissue osteosarcoma
2. According To Radiological Characteristic
- Osteoblastic type of osteosarcoma
- Osteolytic type of osteosarcoma
- Mixed type
3. According To Tumor Histology
- Osteoblastic type of osteosarcoma
- Chondroblastic type of osteosarcoma
- Fibroblastic type of osteosarcoma
- Telangiectatic type of osteosarcoma
Osteosarcoma Clinical Features:
- Age- 10-20 years of age
- Sex- common in males
- Site involved
- Long bone
- Maxilla alveolar ridge, antrum, palate
- Mandible Symphysis, angle, ramus
- Temporomandibular joint
- Tongue
- Lip
- Presents as fast enlarging, firm, painful swelling of the jaw
- Expansion and distortion of cortical plates
- Restricted jaw movements
- Displacement and loosening of teeth
- Paraesthesia of lower lip and chin regions
- Paraesthesia of infraorbital nerve
- Epistaxis
- Nasal obstruction
- Redness and inflamed overlying skin and mucosa
- Ulceration, hemorrhage, pathological fracture
Question 5. Radiographic features of osteosarcoma.
Answer:
Radiographic Features Of Osteosarcoma
- Widening of PDL space is seen
- There are 3 radiographical types
- Osteolytic
- Margins are ill-defined
- Gives moth-eaten appearance
- Mandibular lesions may destroy the cortex of neuromuscular bundles
- Maxillary sinus involvement destroys bone
- Lamina Dura is destroyed
- Mixed
- New bone is laid down with not well-defined margins
- There are areas of destruction as well as bone formation
- This gives a honeycomb appearance
- Osteoblastic
- Mixed lesions have ragged, ill-defined borders
- The sclerotic portion shows vertical obliteration of the trabecular pattern giving a granular appearance
- If the tumor invades the periosteum, many thin irregu¬lar spicules of new bone are directed outwards and perpendicular to the surface of the lesion producing sun ray appearance
- Sometimes two triangular radiopacities project from the cortex and mark the lateral extremities of the lesion referred to as Codman’s triangle
- The subperiosteal bone may be laid down in layers giving an onion-peel appearance
- There is a distortion of the alveolar ridge
Question 6. Brachytherapy.
Answer:
Brachytherapy
- It is a type of radiation therapy used to treat cancers
- In it, the radioactive source is kept close to the patient’s body and directed to the surface of the tumor
Brachytherapy Types:
- Mold Treatment
- The radiation source is placed into the plastic mold on the patient’s skin or mucous membrane to treat su¬perficial tumors
- Interstitial Therapy
- Involves the insertion of a radioactive source into the tumor
- Intracavitary Therapy
- In this, the radiation source is placed into the body cavity to irradiate the surrounding tissues
Question 7. Oncovirus,
Answer:
Oncovirus
- Oncovirus are associated with neoplasms
- Based on nucleic acid content, oncovirus is divided into 2 groups:
- DNA virus
- RNA virus
1. DNA Virus
- They have direct access to the host cell nucleus and are incorporated into the genome of the host cell’s DNA
- Classified Into 5 Groups:
- Papova virus: responsible for skin warts and invasive cervical cancer
- Herpes virus: Epstein Burr virus causes Burkitt’s lymphoma, Human herpes virus
- causing Kaposi’s sarcoma
- Adenovirus: causes respiratory tract infections and pharyngitis
- Poxvirus: causes molluscum contagiosum
- Hepadna virus : Hepatitis B virus
Oral Medicine Tumours Viva Voce
- Cementifying fibroma is a tumor of mesodermal origin
- Floating teeth are found in Langerhans cell granulomatosis
- The majority of tongue carcinoma occurs in the anterior two-thirds of the tongue
- Burkitt’s lymphoma is caused by Epstein Burr virus
- Multiple myeloma is a malignant neoplasm of plasma cells
- Metastasis mainly involves submaxillary and cervical lymph nodes
- A common route for metastasis of oral cancer is lymphatics
- A common site of metastatic in the oral cavity is a mandibular molar area
- In cylindroma, basal cells are arranged in the honeycomb or Swiss cheese pattern
- Ameloblastoma is an ectodermal tumor of Odontogenic origin
- Verocay bodies are seen in neurilemmoma
- Reed Sternberg cells are seen in Hodgkin’s lymphoma
- Lisegang rings are seen in the Pindborg tumor