CBSE Class 11 Chemistry Notes For Chapter 4 Chemical Bonding And Molecular Structure Theory Of Valency Kossel-Lewis Theory
Earlier the term ‘valency’ was defined as the combining capacity of an element. In order words, an element can combine with another element.
Theories of valency were a direct consequence of the development of the atomic structure. w. Kossel and G.N. Lewis were the pioneers in this field, who provided logical explanations of valency, based on the internees of noble gases, which was later known as the noctule. The rule was later modified by Langmuir based on the following-
One or more than one electron(s) of the valence shell i.e., the outermost shell (both penultimate and ultimate shell in some cases) of an atom participates in the chemical reaction. Hence they are responsible for the valency of the atom. These electrons are called valence electrons.
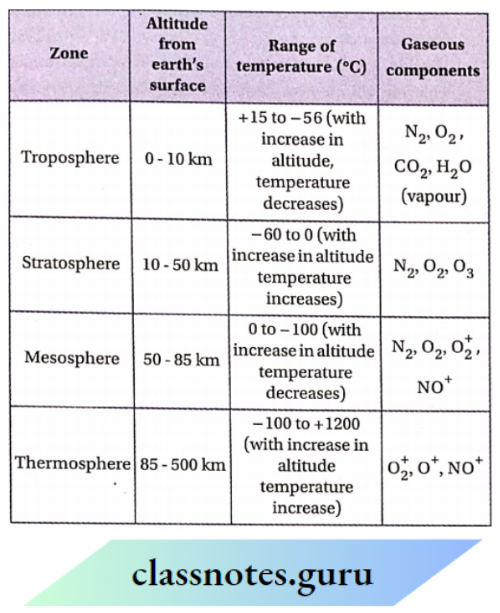
Helium (2He), Neon (10Ne), Argon (18Ar), Krypton (36Kr), Xenon (54Xe), and Radon (86Rn) — these noble gaseous elements possess very high ionization potential but very low electron affinity.
They do not undergo any reaction under normal conditions. Thus they are called inert gases and are placed in the zero group ofthe periodic table which means they are zero-valent. The electronic configuration of He is 1s² and the general electronic configuration of other inert gases is ns²np6. Thus, the total no. of electrons in the outermost shell of the inert gases (other than Helium) is 8. As the noble gas elements are reluctant towards chemical bond formation, this type of electronic configuration is assumed to be stable.

Octet And Duplet Rule
The study of noble gases showed that they are chemically inert, as they have very stable electronic configurations. Kossel and Lewis stated that the stability of noble gases is due to the presence of eight electrons in their valence shell (called octet)
or two electrons (called duplet) as in the case of helium. Most of the two electrons (called duplet) as in the case of helium.
Most of the elements take part in chemical reactions or bond formation to complete their respective octet or duplet.
- Octet rule: Atoms of various elements (except H, Li and Be) combine either by transfer of valence electron(s) from one atom to another (gain or loss) or by sharing of valence electrons so that they have eight electrons (an octet) in their outermost (valence) shells.
- Duplet rules: the element’s dose to helium (H, Li, Be) in the periodic table to attain the stable electronic configuration of He (Is²) by gaining, losing, or sharing electrons in their valence shells.
Chemical Bonding Class 11 Notes
Significance and Limitations of Octet Rule:
Significance of Octet Rule:
The reason behind the formation of covalent or ionic bonds by the atoms of different elements can be explained by the octet rule.
Limitations of Octet Rule: A few limitations of octet rule are as follows—
- The central atom of some molecules, despite having more or less than 8 electrons in the valence shell is quite stable.
- There are some molecules whose outermost shell contains an odd number of electrons. For example— NO, NO2, etc.
- Though the octet rule is based on the inertness of the noble gases, some noble gases form compounds with oxygen and fluorine This rule cannot predict the shape of molecules.
- The comparative stability of the molecules cannot be predicted from this rule.
Lewis symbols
- All the electrons present in an atom are not involved during chemical combination. It was proposed that the inner shell electrons are well protected and generally do not take part in chemical combinations.
- It is mainly the outer shell electrons that take part in chemical combinations. Hence, these are also called valence shell electrons.
- G. N. Lewis introduced simple notations to represent the valence electrons in an atom. The outer shell electrons are shown as dots surrounding the symbol of an atom.
- These notations showing the symbol of an atom surrounded by an appropriate number of dots are known as Lewis symbols or electron dot symbols.
Lewis symbols ignore the inner shell electrons. For example, the Lewis symbols for the elements of the second period are—

Significance of Lewis symbols:
- The number of dots present in the Lewis symbol of an atom gives the number of electrons present in the outermost (valence) shell of that atom. This number is useful for the calculation of the common valency of an element.
- The common valency of an element is either equal to the number of dots in the Lewis symbol (when these are < 4) or % 8 – the number of dots (when these are > 4).
- For example, the common valencies of Li, Be, B, and C are equal to the number of electrons present in their valence shell i.e., 1, 2, 3, and 4 respectively, while those of N O, F, and Ne are 8 minus number of dots, i.e., 3, 2, 1 and 0 respectively.
- When the monovalent, divalent, trivalent, etc., metal atoms are converted to unipositive, dipositive, tripositive, etc., ions, no electrons are present in their outermost shell.
On the other hand, when the monovalent, divalent, trivalent, etc., non-metal atoms are converted to negative, negative, try negative, etc., ions, the outermost shell of each of them contains 8 electrons. Lewis symbols of some cations and anions are given below.

Chemical bonding
Chemical bonding Definition:
The force of attraction between the atoms participating in a chemical reaction, to attain the stable electronic configuration of the nearest noble gas by gaining, losing, or sharing electrons in their valence shells, is called chemical bonding.
Atoms acquire the stable inert gas configuration in the following ways
By complete transfer of one or more electrons from one atom to another:
This process leads to the formation of a chemical bond termed an electrovalent bond or ionic bond.
By sharing of electrons: This occurs in two ways.
- When two combining atoms contribute an equal number of electrons for sharing, the bond formed is called a covalent bond. The shared electron pair(s) remains common to both the atoms.
- When the shared pair of electrons is donated by one of the two atoms involved in the formation of a bond, then the bond.
Types of chemical bonds: Chemical bonds are of 3 types
- Electrovalent or ionic bond
- Covalent bond and
- Coordinate or dative bond.
Class 11 Chemistry Chapter 4 Notes
Electrovalency And Electrovalent Bond
An ionic or electrovalent bond is formed by the complete transfer of one or more electrons from the valence shell of an electropositive (metal) atom to that of an electronegative (nonmetal) atom so that both atoms can achieve the stable electronic configuration of the nearest noble gas.
In this process, the metal atom and non-metal atom result in the formation of a cation and an anion respectively. These two oppositely charged species combine through the electrostatic force of attraction to form an ionic crystal (electrovalent compound.
Elecrovalency:
To achieve the stable electronic configuration, some atoms give up one or more valence electrons completely to form stable cations while some other atoms gain these electrons to form stable anions and ultimately these two types of oppositely charged species combine through electrostatic forces of attraction to form compounds. The capacity of the elements for such a chemical combination Is known as electrovalency.
Ionic Or Electrovalent Bond:
The coulomblc or electrostatic force of attraction which holds the oppositely charged Ions of combining atoms formed by the complete transfer of one or more electrons from the electropositive to the electronegative atom is called an ionic or electrovalent bond.
Ionic Or Electrovalent Compound:
- Compounds Containing inoinc or electrovalent bonds are called electrovalent compounds.
- In the formation of an electrovalent compound, the number of electrons (s) lost or gained by an atom of any participating element gives the measure of its electrovalency.
- For example, in the compound sodium chloride (NaCl), the electrovalent of sodium = 1 and the electrovalency of chlorine = 1. In magnesium chloride (MgCl2), each Mgatom loses two electrons and each Cl-atom gains one electron, so the electrovalency of magnesium and chlorine are 2 and 1 respectively.
Examples of ionic compound formation: The formation of some ionic compounds is discussed below—
Formation of sodium chloride (NaCl):
The electronic configuration of sodium (11Na) atom: Is22s22p63s1 and that of chlorine (17C1) atom: ls22s22p63s23p5. Na has only one electron in its valence shell.
- Being an electropositive element, sodium tends to lose electrons.
- So, it loses its valence electron to acquire the configuration of the nearest noble gas, Ne (ls22s22p6). On the other hand, Cl– atom has seven electrons in its valence shell. Being an electronegative element, chlorine tends to gain electrons.
- So, it can acquire the stable electronic configuration of the nearest noble gas. Ar (ls22s22p63s23p6) by gaining one electron.
- Therefore, when a Na-atom combines with a Cl–atom, the former transfers its valence electron to the latter resulting in the formation of sodium ion, Na+, and chloride ion, Cl– respectively.
- These two ions may be considered as two charged spherical particles.
- The charge is distributed throughout the surface of these spheres, and the field of the electrostatic attraction is distributed in all directions.
- Hence, even after the formation of the ion-pair Na+Cl–, these ions can attract oppositely charged ions towards themselves, the Columbia attractive forces of these two oppositely charged ions are not satisfied.
- Because of this, a large number of Na+Cl– ion pairs attract each other to form an aggregate and consequently, the energy of the system decreases.
This process is completed when a stable crystal of NaCl having a suitable shape and size is obtained. Since the formation of crystal lattice is a thermodynamically favorable process, therefore, the formation of ionic compounds like NaCl is a result of the formation of a three-dimensional crystal lattice.

Formation of calcium oxide (CaO):

Formation of magnesium nitride (Mg3N2):

Formation of aluminium oxide(Al2O3):

Electrovalent or ionic bond and periodic table
The tendency of an element to form a cation or an anion depends on its position in the periodic table.
- The elements of group-1(1A), the alkali metals, and group-2(2A), the alkaline earth metals, belonging to s-block are highly electropositive and have very low ionization enthalpy because of larger atomic size.
- Therefore, to achieve the octet, these elements can easily form monovalent or divalent cations by losing one or two valence electrons respectively.
- On the other hand, the elements of groups 15 (5A), 16(6A), and 17(7A) belonging to the p-block are highly electronegative and possess higher values of electron gain enthalpy (electron affinity] owing to smaller atomic size.
- Therefore, to achieve the octet, these elements can easily accept 3, 2, or 1 electron respectively to form the corresponding anions.
- Hence, the metals of groups 1(1A) and 2(2A) react chemically with the non-metals (nitrogen, oxygen, halogen, etc.) of groups- 15(5A), 16(6A),and17(7A) to form ionic compounds.
- Note that nitrides, halides, oxides, sulfides, hydrides, and carbides of alkali metals (Na, K, Rb, Cs) and alkaline earth CaO metals (Mg, Ca, Sr, Ba) are generally ionic compounds.
Chemical Bonding And Molecular Structure Class 11
Factors favoring the formation of ionic compounds
- Number of valence electrons: The atom forming the cation should have 1, 2, or 3 valence electrons, whereas the atom forming the anion should have 5, 6, or 7 electrons in its outermost shell.
- The difference in electronegativity: There should be a large difference in electronegativities of the combining atoms. The greater the difference in electronegativities of the two atoms, the greater the ease of of ionic bond.
- Sizen of the ions: The formation of ionic bonds is favored by large cations and small anions.
- Ionization enthalpy and electron affinity: The lower the Ionisation enthalpy of the electropositive atom, the easier the formation of the cation. The higher the negative electron gain enthalpy of the electronegative atom, the easier the formation of the anion.
- The magnitude of charges: The higher the charge on the ions, the greater the force of attraction. Hence, the larger the amount of energy released, the greater the stability of the bond.
- Lattice enthalpy (or energy): The higher the value of of lattice enthalpy (electrostatic attraction between charged ions in a crystal), the greater the tire stability of the ionic bond and hence greater tire ease of formation of the compound.
Lattice Energy
The cations and anions combine to form three-dimensional solid substances known as ionic crystals. During the formation of a crystalline ionic compound, the ions of opposite charges come closer from an infinite distance and pack up three-dimensionally in a definite geometric pattern.
This process involves the liberation of energy because the attractive force between the ions of opposite charges tends to decrease the energy of the system. The energy thus liberated is called lattice energy or lattice enthalpy. Generally, it is denoted by U.
Lattice Energy Definition
Lattice enthalpy or lattice energy may be defined as the amount of energy evolved when one gram-formula mass of an ionic compound is formed by the close packing of the oppositely charged gaseous ions.
M+ (g) + X–(g) → M+ X–(s) + U (lattice energy)
The higher the value of lattice enthalpy, the greater the stability of the ionic compound. It has been observed that
⇒ \(U \propto \frac{\text { Product of ionic charges }}{\text { Distance between cation and anion }}\)
Thus, lattice enthalpy depends on the following factors:
- Charges on ions: The higher the charge on the ions, the greater the forces of attraction, and consequently, a larger amount ofenergy is released. Thus, the lattice enthalpy is high.
- Charges on ions Example: The lattice enthalpy of CaO (3452.7 kJ–mol-1 ) is greater than that of NaF(902.9 kJ–mol-1). This is because the charges on the two ions in CaO (+2 and -2) are greater than those on the two ions in NaF (+1 and -1).
- Size of the ions: The smaller the size of ions, the lesser the internuclear distance. Thus, the interionic attraction is greater resulting in higher lattice enthalpy.
- Size of the ions Example: The lattice enthalpy of KF (802.6 kJ.mol-1) is higher than that of KI (635.4 kJ.mol-1). This is because the ionic radius of the F– ion (1.36 Å) is less than that of the r ion (2.16 Å).
Similarly, the lattice energy of NaCl is greater than that of KCl. However, lattice energy is more dependent on the charge of an ion rather than its size.
Hence, the order of lattice energy is—
- LiF > NaF > KF > RbF > CsF
- LiF > LiCl > LiBr >Li
Born-lande equation:
Lattice energy (U) cannot be determined directly. However, its theoretical value can be calculated using the equation given below
⇒ \(U=-\frac{A e^2 Z_{+} Z_{-} N}{r}\left(1-\frac{1}{n}\right)\)
Where
A = Madelung constant
N=Avogadro’s number
n = a constant called Bom exponent (depends on the repulsive force arising from interionic penetration and is generally taken to be 9),
e = charge of an electron, Z+ and Z ¯ are the charges on the cation and the anion respectively
r = interionic distance (minimum distance between the centers of oppositely charged ions in the lattice).
Calculation of lattice enthalpy from the Born-Haber cycle:
The lattice enthalpy of an ionic compound cannot be measured directly by experiment. It can be measured indirectly from the Born-Haber Cycle. In 1919, Max Bom and Fritz Haber proposed a method based on Hess’s law for calculating lattice enthalpy by relating it with other thermochemical data.
It can be illustrated as follows:
Calculation of lattice enthalpy of NaCl:
The ionic compound, NaCl(s) may be formed from its constituent elements by two different paths. It may be formed by the combination of its constituent elements directly i.e., from sodium and chlorine. This is an exothermic process. The heat evolved at 25°C and 1 atm pressure is called standard enthalpy of formation \(\left(\Delta \boldsymbol{H}_f^{\mathbf{0}}\right)\).
⇒ \(\mathrm{Na}(s)+\frac{1}{2} \mathrm{Cl}_2(s) \rightarrow \mathrm{NaCl}(s) ; \Delta \mathrm{H}_f^0=-411.2 \mathrm{~kJ} \mathrm{~mol}^{-1}\)
The formation of 1 mol of NnCl(s) may also be considered indirectly through the following steps: O Sublimation of solid Nu to gaseous Na:
The energy needed to break down the metal lattice of sodium is called sublimation energy (S) or enthalpy of sublimation \(\left(\Delta H_s^0\right)\)
⇒ \(\mathrm{Na}(s) \rightarrow \mathrm{Na}(\mathrm{g}) ; \Delta H_s^0=+108.4 \mathrm{~kJ} \cdot \mathrm{mol}^{-1}\)
Formation of gaseous Na+ ion:
The energy required in this process is called the ionization energy (I) or ionization enthalpy \(\left(\Delta H_i^0\right)\)
⇒ \(\mathrm{Na}(\mathrm{g}) \rightarrow \mathrm{Na}^{+}(\mathrm{g})+e^{-} ; I=+495.6 \mathrm{~kJ} \cdot \mathrm{mol}^{-1}\)
Dissociation of Cl2 molecule into Gl-atoms:
The dissociation energy (D) or enthalpy of dissociation \(\left(\Delta H_d^0\right)\) is the amount of energy needed to convert 1 mol of Cl2 molecules into 2mol of Cl– atoms. To produce 1 mol of Cl-atoms, half dissociation energy is required.
⇒ \(\frac{1}{2} \mathrm{Cl}_2(\mathrm{~g}) \rightarrow \mathrm{Cl}(\mathrm{g}) ; \frac{1}{2} \Delta H_d^0=+121 \mathrm{~kJ} \cdot \mathrm{mol}^{-1}\)
Formation of Cl- ions:
It is an exothermic process. The energy evolved is called electron-gain enthalpy (JE).
⇒ \(\mathrm{Cl}(\mathrm{g})+e \rightarrow \mathrm{Cl}^{-}(\mathrm{g}) ; E=-348.6 \mathrm{~kJ} \cdot \mathrm{mol}^{-1}\)
Formation of NaCl(s) from Na+(g) and Cl–(g):
It is an exothermic process that results in the liberation of energy known as lattice energy lattice enthalpy (U).

According to Hess’s law:
⇒ \(\Delta H_f^0=\Delta H_s^0+I+\frac{1}{2} \Delta H_d^0+E+U\)
∴ U =-411.2 -108.4 -495.6 -121 -(-348.6)
= -787.6 kl-mol-1
Thus, the lattice enthalpy of NaCl(s) has a large negative value. This indicates that the compound is highly stable.
Importance of lattice enthalpy:
- A negative value of lattice enthalpy indicates that the formation of a crystalline ionic compound from its constituent ions is an exothermic process, i.e., an ionic crystal is more stable compared to its constituent ions.
- The magnitude of lattice enthalpy gives an Idea about the forces and the stability of the ionic compound. The higher the negative value of lattice enthalpy greater the stability of the ionic compound.
- A higher value of lattice enthalpy indicates that the ionic crystal is hard, has a high melting point, and is less soluble in water.
CBSE cLass 11 Chemistry Chapter 4 Notes
The order of lattice enthalpy of some ionic compounds:
- LiX > NaX > KX > RbX > CsX
- MgO > CaO > SrO > BaO
- MgCO2 > CaCO3 > SrCO3 > BaCO3
- Mg(OH)2> Ca(OH)2 > Sr(OH)2 > Ba(OH)2
Most of the ionic compounds are formed by reaction between cations (of metals) and anions (of non-metals). However, ammonium ion (NH), a cation obtained from two non-metallic elements is a very common exception.
Variable electrovalency and exceptions to the octet rule
Several metals like Ga, In, Tl, Sn, Pb, Bi, etc. (belonging to groups 13, 14, and 15 of-block) and Cr, Mn, Fe, Cu, etc. (belonging to d-block) exhibit variable electrovalency by losing different numbers of electrons. The reasons for exhibiting several electrovalency are
- Unstable electronic configurations of the ions and
- Inert pair effect. Some exceptions to the octet rule are also observed in the case of these metals.
Variable valency of heavy p-block elements:
Some heavier p -p-block elements having the valence shell electronic configuration: ns2npl-6 exhibit variable electrovalency.
- However, their primary valency is equal to the number of electrons present in the ultimate and penultimate shells.
- Why is it so? The electronic configuration of these elements has revealed that both d and f-electrons are present in the valence shell of these elements.
- Due to the poor screening effect of the d and orbitals, the s-electrons of the outermost shell are held tightly to the nucleus.
- As a result, a pair of electrons present in the ns orbital are reluctant to take part in the reaction. This is called the inert pair effect. Due to the inert pair effect, heavier p-block elements show variable valency.
Example:
- Lead (Pb) shows a +2 oxidation state predominantly due to the inert pair effect.
- Pb: [Xe]4f145d106s26p2. The two 6p¯ electrons are easily lost to attain the +2 oxidation state.
- However, due to the very poor shielding effect of the 4f and 5d -electrons, the pair of 6s¯ electrons get closer to the nucleus and hence, are more tightly bound by the nuclear force.
- A large amount of energy must be expended to unpair the electron pair in the 6s -orbital and hence, they tend to exist as an inert pair.
Hence, the common oxidation state of Pb in most of its compounds is +2. It is only in the presence of highly electronegative elements like fluorine and oxygen that the pair of electrons in the 6s¯ orbital can be unpaired and one of the electrons is promoted to the 6p¯ orbital giving rise to the +4 oxidation state of Pb.
Hence, only two compounds of Pb in the +4 oxidation state are known, viz., lead tetrafluoride (PbF4) and lead dioxide (PbO2).
Variable valency of d-block (transition) elements:
- The general electronic configuration of d-block elements is (n-1)d1-10-10ns1-2
- Here, apart from the s-electrons of the 1st shell, one or more d-electron(s) of (n-1)th shell contribute to the valency and hence to the oxidation state of the elements.
- Hence, the d-block elements exhibit variable valency.
Examples:
- The electrovalency of iron (Fe) may be 2 or 3. The electronic configuration of Fe ls22s22p63s23p63d64s2. It forms a Fe2+ ion by the loss of two electrons from the 4s orbital. Soin ferrous compounds, the electrovalency of Fe is +2. Fe2+ ion has a less stable d6 configuration.
- Therefore, it loses one electron more to form Fe3+ ion thereby attaining a relatively more stable configuration. So, the electrovalency of Fe in ferric compounds is 3.
- In the outermost shells of Fe2+ and Fe3+ ions, there are 14 and 13 electrons respectively. Thus, the octet rule is violated in both cases. The electrovalency of copper (Cu) can either be 1 or 2, i.e., it may either form Cu+ or Cu2+ ions.
- The electronic configuration of Cu is ls22s22p63s23p63d104s1. A single Cu-atom loses one 4s -electron and gets converted into a Cu+ ion. So in cuprous compounds, the electrovalency of Cu is 1.
Chemical Bonding Notes For NEET
- The nuclear charge of Cu is not sufficient enough to hold 18 electrons of Cu+ ion present in the outermost shell and hence, to acquire greater stability, Cu+ ion loses one more electron from the 3d -orbital to form Cu2+ ion.
- So, the electrovalency of copper in cupric compounds is 2. In the outermost shells of Cu+ and Cu2+, there are 18 and 17 electrons respectively. Thus, the octet rule is violated in both cases.
Exceptions to the octet rule in some elements

Shapes of ionic compounds
For the maximum stability of ionic compounds, cations, and anions form crystals by arranging themselves in regular and definite geometrical patterns so that the coulom forces of repulsion among the ions of similar charge, as well as electron-electron repulsion among the extranuclear electrons, are minimum.
- The shape of the crystals depends on the charges of the ions, their packing arrangements, and the ratio of the cation to anion radius.
- It can be shown by simple geometrical calculation that if the radius ratio is greater than 0.414 but less than 0.732, each cation is surrounded by the six nearest anionic neighbors. Such an array gives rise to the octahedral crystal ofthe compound.
So, during the formation of a NaCl crystal, each Na+ ion is surrounded by six neighboring Cl–ions, and each such Cl– ton is similarly surrounded by six neighboring Na+ ions, each ion lies at the center of an octahedron and the oppositely charged ions reside at tire corners of that octahedron. This type of arrangement is called 6-6 coordination.

Coordination number:
- In an ionic crystal, the number of oppositely charged adjacent ions that are equidistant from a particular ion (in 3D close packing) is called the coordination number (C.N.) of that ion.
- Positive and negative ions both have the same coordination number when there are equal numbers of both types of ions present (NaCl), but the coordination numbers for positive and negative ions are different when there are different numbers of oppositely charged ions (CaCl2).
Example:
When the radius ratio (r+/r-) is less than 0.414, the coordination number is less than 6, but when the radius ratio (r+/r-) is more than 0.732, the coordination number is more than 6. In cesium chloride (CsCl), rCs+/rcr = L69A/1.81 Å = 0.933.
- So in a CsCl crystal, each Cs+ ion is surrounded by eight Cl- ions, and each Cl- ion is similarly surrounded by eight Cs+ ions. In this case, the coordination number of both the Cs+ and Cl- ions is 8. On the other hand, in zinc sulfide (ZnS) crystal, rZni+/rS2- = 0.74A/1.84Å = 0.40.
- In the ZnS crystal, each Zn Ion is surrounded by four S2- ions, and each S2- lon is surrounded by four Zn2+ ions. So, the coordination number of both ions is 4.
- In the formation of ternary ionic compounds [such as calcium fluoride crystal (CaF2) to maintain electrical neutrality, the coordination number of calcium ions (Ca2+) becomes twice the coordination number of fluoride ions (F–).
- In CaF, crystal, each Ca2+ ion is surrounded by eight F– ions while each F– ion is surrounded by four Ca2+ ions.
Role of cation and anion in the formation of stable crystal:
The definite position of the anions surrounding a cation in a stable octahedral crystal is shown. Two anions, aligned vertically above and below the central cation have not been shown.
- In this case, the radius ratio (r+/r_) is in the range: of 0.414 – 0.732. If the size of the cation is small, then the value of (r+/r-) will be diminished and in this condition, the anions in contact will repel each other.
- But the cation, not being in contact with tire anions, will not attract them. Consequently, a stable octahedral crystal will not be formed. Instead, the ionic compound assumes a tetrahedral structure with coordination number 4 by disposing of its ions suitably, so that it gains stability.
- Stated differently, if the cation is much smaller in size than the anion, four anions are sufficient to surround the central cation—six anions are not required. When the cationic size is very large, the value of (r +/r-) increases.
- In such a case, the anions touch the cation but do not touch each other. So, a stable octahedral structure will not be formed. Hence, more anions should surround the central cation so that they touch each other to give rise to
A stable cubic structure with coordination number 8.

Radius ratio (r+/r–),C.Nand crystalstructure

The given rules relating radius ratio with crystal structure apply only to those ionic compounds in which the cation and the anion bear the same charge (electrovalency).
For example, in NaCl, the electrovalency of both Na+ and Cl– is 1, and in ZnS, the electrovalency of both Zn2+ and S2- is 2, etc. The radius ratio rule (mentioned above) is not applicable for those ionic compounds in which the electrovalencies of cations and anions are not equal.
Note that a conglomeration of countless cations and anions leads to the formation of crystals of an ionic compound. Hence, there is no existence of a separate molecule and the entire crystal exists as a giant molecule.
Properties and characteristics of ionic compounds
- Physical state: In ionic compounds, there is no existence of separate molecular entities. Oppositely charged ions arrange themselves three-dimensionally, forming a crystal of definite geometrical shape. The compounds are solids at ordinary temperature and pressure.
- Melting and boiling points: In ionic compounds, the oppositely charged ions are held together, tightly by strong electrostatic forces of attraction, and hence a huge amount of energy is required to overcome these forces, i.e., to break the compact and hard crystal lattice. As a result, the melting and boiling points of ionic compounds are generally very high.
- Directional nature: Electrostatic force in an ionic compound extends in all directions. Hence, ionic bonds are non-directional.
- Isomerism: Due to the non-directional nature of ionic bonds, ionic compounds do not exhibit isomerism.
- Electrical conductivity: Ionic compounds do not conduct electricity in the solid state because oppositely charged. Ions are held together strongly with a coulomb force of attraction extending in all directions.
NCERT cLass 11 Chemistry Chapter 4
- But in the molten state or solution in a suitable solvent (like water), the ions being free from the crystal lattice, conduct electricity.
- Solubility: Ionic compounds generally dissolve in polar solvents i.e., solvents possessing high dielectric constant, (e.g., water), and insoluble in non-polar solvents (e.g., carbon disulfide, carbon tetrachloride, benzene, etc.).
- Isomorphism: Isoelectronicionic compounds generally exhibit the property of isomorphism (both of the ions have similar electronic configurations).
Two pairs of isomorphous compounds are—
Sodium Fluoride (Naf) and magnesium oxide (MgO):
Potassium sulfide (K2S) and calcium chloride (CaCl2)
Example:
⇒ [Na+(2, 8) F–2, 8)], [Mg2+(2, 8) O2-(2, 8)]; [K+(2, 8, 8) S2+(2, 8, 8)], [Ca2+(2, 8, 8) Cl–(2, 8, 8)]
Ionic reaction and its rate:
In an aqueous solution, electrovalent compounds exist as ions. In any solution, the chemical reaction of ionic compounds is the chemical reaction of the constituent ions of that compound. As a result, a chemical reaction between ionic compounds in solution is very fast.
For example: On addition of an aqueous solution of AgNO3 to an aqueous solution of NaCl,
A white precipitate of AgCl is formed immediately:
⇒ \(\mathrm{Na}^{+} \mathrm{Cl}^{-}+\mathrm{Ag}^{+} \mathrm{NO}_3^{-} \rightarrow \mathrm{AgCl} \downarrow+\mathrm{Na}^{+} \mathrm{NO}_3^{-}\)
Solvation of ions and solvation energy or enthalpy
Ionic compounds dissolve in polar solvents (for example water).
- Such solvent molecules strongly attract the ions present in the crystal lattice of solid ionic compounds and detach them from the crystal.
- When any ionic compound dissolves in a polar solvent, the negative pole of the solvent molecule attracts the cation that forms the crystal while its positive pole attracts the anion.
- As a result, the electrostatic force of attraction between the cations and anions decreases.
- If the magnitude of this attractive force of the polar solvent molecules exceeds the lattice energy of the solute, the ions present in the crystal get detached from the crystal lattice and are dispersed in the solvent.
Ions present in the solvent, being surrounded by a suitable number of solvent molecules (i.e., being solvated) are stabilized.
- For example, at the time of dissolution of NaCl in water, each Na+ and Cl– ion being surrounded by six water molecules, becomes solvated to form stable hydrated ions. This process is known as solvation.
- The amount of energy released when one mole (one gram formula mass) of an ionic crystal is solvated in a solvent, is known as the solvation.

Energy evolved in the dissolution of ionic compounds:
The solvation energy is die driving force that brings about die total collapse of the structural framework work of the crystal.
- Higher the dielectric constant the capacity of the solvent to weaken the forces of attraction) and dipole moment of the solvent, the higher the die magnitude of die solvation energy.
- Moreover, solvation energy also depends on the sizes ofthe cations and anions. ΔH solution = ΔH solvation lattice where ΔHsolution = energy evolved in the dissolution of the ionic compound, ΔH solvation = solvation enthalpy, and ΔHlattice enthalpy of the ionic compound.
- If the solvation energy exceeds the lattice energy, then that ionic compound is soluble in that solvent but if It is much less, then the ionic compound is insoluble in that solvent.
Example: CaF2 is insoluble in water while CaCl2 is appreciably soluble. This implies that the lattice energy of CaF2 is more than the solvation energy of its constituent ions, but the lattice energy of CaCl2 is less than the solvation energy of its constituent ions.
- It is to be noted that ionic compounds do not dissolve in non-polar solvents (turpentine oil, gasoline, etc.) because solvation of ions by the non-polar solvent is not possible.
- For most of the ionic compounds, ΔH° is +ve, i.e., the dissolution process is endothermic. Hence, the solution solubility of most of the salts in water increases with the temperature rise.
Covalency And Covalent Bond
Formation of ionic bonds is not possible when the atoms of similar or almost similar electronegativities combine. This is because the electron affinity of both atoms is of the same or approximately the same order.
- Therefore, the electron transfer theory’ (as discussed in the case of ionic bond formation) cannot explain the bonding in molecules such as H2, O2, N2, Cl2, etc.
- To explain the bonding in such molecules, G. N. Lewis (1916) proposed an electronic model, according to which, the chemical bond in a non-ionic compound is covalent.
- He suggested that when both the atoms taking part in a chemical combination are short of electrons than the stable electronic configuration of the nearest noble gas, they can share their electrons to complete their octets (duplet in the case of H).
- This type of bond, formed by mutual sharing of electrons, is called a covalent bond.
- During the formation of a covalent bond, the two combining atoms contribute an equal number of electrons for sharing. The shared electrons are common to both atoms and are responsible for holding the two atoms together.
Since such a combination of atoms does not involve the transfer of electrons from one atom to another, the bonded atoms remain electrically neutral.
Covalency:
To achieve the electronic configuration of the nearest noble gas, an equal number of electron(s) from the outermost shells of two combining atoms remaining in the ground state or excited state, form one or more electron pairs that are evenly shared by the two atoms. The capacity of the elements for this type of chemical combination is called covalency.
Covalent bond:
The force Of attraction that binds atoms of the same or different elements by the mutual sharing of electrons is called a covalent bond. The atoms involved in covalent bond formation contribute an equal number of electrons for sharing. The shared electron pair(s) are common to both atoms.
Covalent Molecules:
- The molecules that consist of atoms held together by covalent bonds are called covalent molecules.
- The number of valence electrons shared by an atom of an element to form covalent bonds is called the covalency of that element.
- Therefore, the covalency of an element in a covalent molecule is, in fact, equal to the number of covalent bonds formed by its atom with other atoms of the same or different element.
For example: In a carbon dioxide molecule (0=C=0), the covalency of carbon is 4 and that of oxygen is 2.
Driving force behind covalent bond formation:
Any covalent bond is formed by the combination of two electrons of opposite spin.
The driving forces behind the formation of a covalent bond are the electromagnetic force of attraction developed in the pairing of two electrons of opposite spin and the attainment of stability by forming an inert electron core.
Types of covalent molecules
- Homonuclear covalent molecule: The molecules formed when atoms of the same element are joined together by covalent bonds are called homonuclear covalent molecules, for Example; H2, O2, N2, Cl2, etc.
- Heteronuclear covalent molecule: The molecules formed when atoms of different elements are joined together by covalent bonds are called heteronuclear covalent molecules, for Example; NH3, H2O, HC1, CH4, etc.
Types of covalent bonds
- Single bond: The bond formed by the sharing of one electron pair between two atoms is known as a single bond and is represented by ( — ).
- Double bond: The bond formed by sharing two electron pairs between two atoms is known as a double bond and is represented by (=).
- Triple bond: The bond formed by the sharing of three electron pairs between two atoms is known as a triple bond and is represented by (=).
Examples: There exists a single bond between the two hydrogen atoms in a hydrogen molecule (H —H), a double bond between the two oxygen atoms in an oxygen molecule (0=0), and a triple bond between the two nitrogen atoms in a nitrogen molecule (N=N).
Lewis dot structure
The structure of a covalent compound expressed by writing Lewis symbols ofthe participating atoms using one pair of dots between each pair of atoms for each covalent bond where a dot represents an electron is called Lewis dot structure.
Electrons are normally represented by dot or cross (x) signs. Lewis dot structures of fluorine and hydrogen chloride are shown here.

Valence electrons that do not participate in covalent bond formation are simply written as pairs of dots surrounding the symbol of the concerned atom.
Chemical Bonding And Molecular Structure Notes
The steps involved in writing Lewis dot structure are as follows:
- The total number of valence electrons ofthe atoms present in a particular molecule, Orion should be calculated.
- If the species is a cation, the number of electrons equal to the units of +ve charge should be subtracted from the total, and if the species is an anion, the number of electrons equal to the units of -ve charge should be added to the total. This gives the total number of electrons to be distributed.
- The skeletal structure is written by placing the least electronegative atom in the center (except hydrogen) and more negative atoms in the terminal positions. Note that the monovalent atoms like H and F always occupy the terminal positions.
- One shared electron pair should be placed between every pair of atoms to represent a single bond between them. The remaining pairs of electrons are used either for multiple bonding or to show them as lone pairs, keeping in mind that the octet of every atom (except) is completed.
- Remember that oxygen atoms do not bond to each other except in cases of O2, O3, peroxides, and superoxides.
Example: Lewis dot structure of HCN molecule:
- Total number of valence electrons of the atoms in HCN molecule =I (for H-atom) +4 (for C-atom) +5 (for Natom)=10.
- The skeletal structure of the molecule is HCN.
- One shared pair of electrons is placed between H and C and one shared pair is placed between C and N. The remaining electrons are treated as two lone pairs on N and one lone pair on C. H:C: N:O
- Since the octets of C and N are incomplete, multiple bonds are required between them.
- To complete their octets, a triple bond (i.e., two more shared pairs of electrons) should be placed between them. Thus, the Lewis dot structure of the hydrogen cyanide molecule is:

Lewis dot structure of some molecule or ions


Example of covalent bond formation:
Formation of a chlorine molecule (Cl2): Two Cl-atom combine to form a Cl2 molecule. Electronic configuration of a Cl -atom (Z = 17) 1s22s22p63s23p5 i.e., 2, 8, 7
- Thus, each Cl -atom has seven electrons In Its valence shell and needs one more electron to attain a stable electronic configuration of Ar (2, 8, 8), i.e., to achieve the octet.
- During combination, both the Cl -atoms contribute one electron each to form a common shared pair. In this way, both of them complete their octets.
- As a result, a covalent bond Is formed between the two chlorine atoms to produce a chlorine molecule. The completed octets are generally represented by enclosing the dots around the symbol of the element by a circle or ellipse.
The electron pair (s) shared by the bonding atoms is known as the shared pair or bond pair and the electron pair not involved In sharing is known as the unshared pair or lone pair.

Formation of oxygen molecule (O2):

Formation of nitrogen molecule (N2):

Formation of water molecule (H2O)

Formation of carbon dioxide molecule (CO2):

Formal Charge
A molecule Is neutral and its constituent atoms do not carry charges. In polyatomic ions, the net charge is possessed as a whole and not by individual atoms. In some cases, charges are assigned to individual atoms. These are called formal charges.
The formal charge of an atom in a polyatomic molecule or ion is defined as the difference between the number of valence electrons of that atom in an isolated atom and the number of electrons assigned to that atom in the Lewis structure. It can be expressed as follows.

If the atom has more electrons in the molecule Orion than in the free or isolated state, then the atom possesses a negative formal charge and if the atom has fewer electrons in the molecule or ion than in the free or isolated state, then the atom possesses a positive formal charge.
Calculation of Formal Charges Of some Molecules And Ions



Advantages of formal charge calculation:
- The main advantage of the calculation of formal charges is that It helps to select the most stable structure from many possible Lewis structures for a given molecule or Ion.
- Generally, the lowest energy structure (most stable) is the one with the lowest formal charges on the constituent atoms for a particular molecule or ion.
Chemical Bonding Class 11 Chemistry
Factors favoring the formation of covalent bonds
- Number of valence electrons:
- Formation of a covalent bond is favored when each of the combining atoms possesses 4, 5, 6, or 7 (except H) valence electrons.
- Such atoms can form 4, 3, 2, or 1 electron pair(s) with one or more atoms to achieve the octet by mutual sharing. So, elements of groups 14, 15, 16, and 17 form covalent bonds easily.
- High ionization enthalpy:
- The atoms having high ionization energy are unable to form electrovalent bonds. They form molecules through the formation of covalent bonds.
- This behavior is observed in the case of p-block elements.
- Comparable electron-gain enthalpies:
- The formation of a covalent bond is favored when the participating atoms have equal or nearly equal electron-gain enthalpies, they should have equal or nearly equal electron affinity.
- Comparable electronegativities:
- The two atoms involved in covalent bond formation should have equal or nearly equal values of electronegativity because in that case no transfer of electrons from one atom to another takes place and thus, the formation of a covalent bond is favored.
- High nuclear charge and small internuclear distance:
- During the formation of a covalent bond, the electron density is concentrated between the two nuclei of the combining atoms, which is responsible for holding the two nuclei together.
- The greater the nuclear charge and the smaller the internuclear distance, the greater the tendency for the formation of covalent bonds.
Characteristics of covalent compounds
- Physical state: Covalent compounds are composed of discrete molecules. The intermolecular forces of attraction between them are usually very weak. Hence, covalent compounds exist in a gaseous or liquid state. However, a few covalent compounds such as urea, sugar, glucose, etc. exist as solids because of stronger intermolecular forces.
- Melting and boiling points: The attractive force between the molecules of covalent compounds is usually weak and consequently, a lesser amount of energy is required to overcome these forces. As a result, covalent compounds possess low melting and boiling points compared to ionic compounds.
- Electrical conductivity: Covalent compounds do not possess negatively and positively charged ions so, they usually do not conduct electricity in the fused or dissolved state.
However, in some cases, the covalent compound dissolved in a polar solvent reacts with the solvent molecules to form ions and thus conduct electricity.
For example, being a covalent compound, hydrogen chloride is a non-conductor of electricity in the pure state but when dissolved in water, it reacts with water to form hydronium ions and chloride ions. Hence, an aqueous solution of hydrogen chloride (i.e., hydrochloric acid) is capable of conducting electricity.
⇒ \(\mathrm{HCl}+\mathrm{H}_2 \mathrm{O} \rightleftharpoons \mathrm{H}_3 \mathrm{O}^{+}+\mathrm{Cl}^{-}\)
Solubility:
- Covalent compounds are usually soluble in non-polar solvents but insoluble in polar solvents (in conformity with the principle, “like dissolves like”).
- For example, the covalent compound carbon tetrachloride does not dissolve in a polar solvent (like water) but it readily dissolves in the non-polar solvent, benzene. However, some covalent compounds such as alcohol, acetic acid, hydrogen chloride, glucose, etc. dissolve In a die polar solvent, water.
- This Is because they are themselves polar compounds and react with water or participate In the formation of hydrogen bonds with water molecules. For example, HC1 dissolves In water and forms H3O+ and Cl- Ions while glucose (C6H12O6) having five hydroxyl (-Oil) groups, dissolves In water by forming hydrogen bonds with water molecules.
Rate of chemical reaction:
- The reactions of covalent compounds Involve the breaking of strong covalent hond(s) present In their molecules.
- Since It requires sufficient energy and time, the chemical reactions of covalent compounds occur at a relatively slower rate. For example, the formation of ethanol from glucose by fermentation takes nearly 3 days.
⇒ \(\mathrm{C}_6 \mathrm{H}_{12} \mathrm{O}_6 \rightarrow{\text { Zymase }} 2 \mathrm{C}_2 \mathrm{H}_5 \mathrm{OH}+\mathrm{CO}_2\)
Directional characteristics of covalent bond:
- Since the atomic orbitals have definite spatial orientation and the covalent bonds are formed by overlapping of atomic orbitals, the bonds possess directional properties.
- For example, 4 covalent bonds of a sp³ -hybridized C-atom are directed toward the four corners of a tetrahedron and for days, the shape of the CH4 molecule is tetrahedral.
Isomerism:
- Since the covalent bonds are rigid and directional, the atoms involved in the formation of a covalent molecule may be oriented differently.
- Two or more structurally different compounds having different chemical and physical properties may be represented by a single molecular formula.
- Such compounds are called structural isomers, In other words, covalent compounds exhibit structural isomerism.
For example, both dimethyl ether and ethyl alcohol have the same molecular formula (C2H6O), but different structural formulas i.e., they are isomers.

For elements such as hydrogen and nitrogen, oxygen, and fluorine (elements of the second period of the periodic table), the number of unpaired electrons (s) in their valence shells gives a measure of their covalency. Therefore, the covalencies of H, N, O, and F are 1,3, 2, and 1 respectively.
⇒ \(\begin{gathered}
\mathrm{H}: 1 s^1 ; \mathrm{N}: 1 s^2 2 s^2 2 p_x^1 2 p_y^1 2 p_z^1 ; \mathrm{O}: 1 s^2 2 s^2 2 p_x^2 2 p_y^1 2 p_z^1 \text {; } \\
\mathrm{F}: 1 s^2 2 s^2 2 p_x^2 2 p_y^2 2 p_z^1
\end{gathered}\)
For elements such as Be, B, and C, their covalencies are not determined by the number of unpaired electrons(s) in their valence shells in the ground state.
In the excited state, out of two electrons in the 2s-orbital, one electron gets promoted to the 2p-orbital. Thus, there are 2, 3, and 4 unpaired electrons respectively in the valence shells of Be, B, and C. So, their covalencies are 2, 3, and 4 respectively.
- Elements belonging mainly to the 3rd, 4th, and 5th periods of the periodic table possess variable covalencies.
- These elements possess vacant orbitals in their valence shell and are capable of promoting one of the paired electrons of that shell to the vacant orbitals. The number of electrons to be promoted depends on the energy available for excitation.
- Thus, such an element exhibits more than one covalency depending on the availability of unpaired electrons. This is termed as variable covalency. For example— In PCl3 and PCl5, covalencies of P are 3 and 5 respectively;
- In H2S, SF4, and SF6, sulfur exhibits covalencies of 2, 4, and 6 respectively, and in IC1, IC13, IF5, and IF7 iodine has covalence of 1, 3, 5, and 7 respectively.

Variable covalency of phosphorus: 3,5
1. Trlcovalency of P:
The outermost electronic configuration of phosphorus in its ground state:

In the ground state, phosphorus1 has only three unpaired valence electrons in 3px, 3py, and 3pz orbitals. So, the normal covalency of phosphorus is 3.
Example: In phosphorus trichloride (PCl3), phosphorus (sp³ hybridized) exhibits a covalency of 3.
2. Pentacovalency of P:
In the excited state, phosphorus possesses five unpaired electrons in its valence shell by promoting one of its 3s -electrons to the vacant 3dorbital. Thus, it exhibits a covalence of 5.

Example: In phosphorus pentachloride (PCl3), phosphorus (sp³d -hybridized) possesses a covalency of 5.
Variable covalency of sulphur: 2,4,6
1. Bicovalency of S:
The outermost electronic configuration of sulfur in its ground state.

In the ground state, sulfur has only 2 unpaired electrons in 3py and 3pz orbitals. Hence, the covalency of sulfur in the ground state is 2.
Example: In hydrogen sulfide (H2S), sulfur (sp³ hybridized) exhibits a covalency of 2.
2. Tetracovalency of S:
On excitation, one of the paired electrons in 3px -orbital is promoted to vacant 3d -orbital. This results in 4 unpaired electrons in its valence shell.

So, the covalency of sulfur in the first excited state is 4. Example: in sulfur tetrafluoride(SF4), sulfur (sp3 d hybridized) exhibits a covalency of 4.
3. Hexacovalency of S:
In the case of the second excitation, one of the 3s -electrons gets promoted to vacant 3d -orbital. This results in 6 unpaired electrons in its valence shell.

Hence, the covalency of S in the second excited state is 6.
Example: In sulfur hexafluoride (SF6), sulphur {sp³d² hybridised) exhibits a covalency of 6.
Variable covalency of iodine: 1,3, 5, 7
1. Monocovalency of I:
The outermost electronic configuration of iodine in its ground state.

One unpaired electron indicates the monovalency of I.
2. Tricovalency of I:
In its first excited state, one of the paired electrons from the 5p -orbital gets promoted to a vacant 5d -orbital. This leads to the presence of unpaired electrons in its valence shell.

Hence, the covalency of iodine in the first excited state is 3.
Example: In iodine trifluoride (IF3), iodine (sp²d -hybridized) exhibits a covalency of 3.
3. Pentacovalency of I:
In the second excited state, one of the paired electrons from 5px -orbital is promoted to vacant 5d -orbital. This results in the presence of 5 impaired electrons in the valence shell of the I-atom.

Example: In iodine pentafluoride (IF5), iodine (sp³d³ – hybridized) exhibits a covalency of 5.
4. Heptacovalency of I:
I-atom attains the third excited state by promoting one of the paired electrons from 5s -orbital to vacant 5d -orbital. This leads to the presence of 7 unpaired electrons in the valence shell of i-atoms.

Since the Iodine atom now possesses 7 unpaired electrons the covalency of iodinein in the third excited state is 7.
Example: In iodine heptafluoride (IF), iodine (sp³d³- hybridized) exhibits a covalency of7.
Molecular Structure Class 11 Notes
Maximum covalency:
Maximum covalency of an element is the maximum number of unpaired electrons that an atom of an element possesses after promoting electrons from s and the p -orbitals to d -orbitals, i.e., it is the maximum number of covalent bonds that an atom of an element can form. For example, the maximum covalencies of P, S, and I are 5, 6, and 7 respectively.
Limitations of the octet rule
The octet rule, although useful for understanding the structures of most organic compounds, fails in many cases and has several exceptions.
Some important exceptions to the rules are as follows:
Incomplete octet of the central atom:
- Elements of groups, 2, and 13 are not expected to form covalent compounds as they possess less than four electrons in their valence shell and cannot achieve an octet by sharing electrons.
- But, several covalent compounds of these elements are known to exist, which violates the octet rule such as LiCl, BeCl2, BF3, AlCl3, etc.
These compounds with an incomplete octet of the central atom are called hypovalent compounds or electron-deficient compounds.

Expansion of octet of the central atom:
The octet rule is also found to be violated in compounds like PCl5, SF6, and IF7 in which the central atoms possess more than eight electrons in their valence shells, i.e., they possess expanded octets.
These compounds with an expanded octet of the central atom are called hypervalent compounds.

Odd electron molecules:
There are some molecules and ions in which the atoms bonded to each other contain an odd no. of electrons (usually 3).
These bonds formed by three electrons are called odd electron bonds and the corresponding molecules are called odd electron molecules. Octet rule is not satisfied for all the atoms of such molecules. Some common examples are as follows:

Formation of compounds by noble gases:
Noble gases have filled octets and hence are not expected to form compounds.
- However, it has been found that some noble gases like xenon and krypton combine with oxygen and fluorine to form a large number of compounds such as XeF2, XeOF2, XeOF4, XeF6, KrF2, etc. In these compounds, Xe or Kr have expanded octets.
- This theory cannot explain the shapes of covalent molecules. It cannot explain the relative stability of the molecules in terms of energy.
The explanation for the deviations from the octet rule
Sidgwick’s concept of maximum covalency:
- According to Sidgwick, it is not always necessary for an atom of an element to achieve the octet combination.
- He postulated his views in the form of an empirical rule called the rule of maximum covalency. According to this rule, the maximum covalency of an element depends on its position in the periodic table.
- For example, the maximum covalency for H belonging to the first period is 2, the second period (Li to F) is 4, the third (Na to Cl) and fourth period (K to Br) is 6, and for elements of higher periods, it is 8. So, the formation of compounds like PCl5 and SF6 where P and S exhibit penta covalency and hexa covalency respectively, is not irrelevant. The modem electronic concept supports Sidgwick’s concept.
Explanation: In the formation of covalent bonds, atoms of the elements belonging to the second period use one orbital of 2s -subshell and three orbitals of 2p -subshell of L -shell {n = 2). Therefore, they can share a maximum of 8 electrons to form covalent bonds, i.e., their maximum covalency is 4.
The maximum covalency shown by the elements of the third period and that of the higher periods is more than 4. This is because their atoms can form compounds using s, p, and d -orbitals of their outermost shell [M(n = 3), N(n = 4), O(n = 5), etc], For exhibiting higher valency, one or more electrons are promoted from s and p -orbitals to vacant d -orbitals having slightly higher energy. So these elements, depending on the requirement of valency, can utilize 5, 6, 7, or 8 orbitals.
Sugden’s concept of single electron linkage or singlet linkage:
According to Sugden, the central atoms of molecules like PCl5, SF6, etc., attain octets by the formation of one or more one-electron bonds. To explain their structures, he proposed the formation of a new type of bonding called singlet linkage.

Example: In the PCl5 molecule, the P-atom with the help of its 5 valence electrons, forms 3 shared pairs or normal single covalent bonds with three Cl-atoms, and the remaining 2 electrons are used to bond with two Cl-atoms by singlet linkages.
Similarly, the S-atom in SFg molecule forms 2 normal single covalent bonds with two F-atoms using 2 of its 6 valence electrons and the remaining 4 electrons are used to form singlet linkages with four F-atoms.
Limitations of the concept of singlet linkage:
Singlet electron linkage is weaker than a normal covalent bond.
- Vapors of PCl5 dissociate into PCl5 and Cl2 at 300°C. This indicates that two P —Cl bonds in PClg are comparatively weaker than the remaining three P—Cl bonds.
- However, SFg is a very stable molecule and experimental results show that all the six S —F bonds are similar.
- Hence, it is not possible to distinguish between singlet electron linkage and normal covalent bond in the case of SF6. There are 5 valence electrons present in the outer shell of both nitrogen and phosphorus.
- However, nitrogen forms only trihalides (NX3, X = Cl, Br, I), while phosphorus forms both trihalides (PX3) and pentahalides (PX5). If singlet electron linkages exist, then nitrogen would also have formed pentahalides.
- Although the concept of singlet electron linkage explains the formation and properties of a few molecules, it fails in most of cases.
- There are 5 valence electrons present in the outer shell of both nitrogen and phosphorus. However, nitrogen forms only trihalides (NX3, X = Cl, Br, I), while phosphorus forms both trihalides (PX3) and pentahalides (PX3).
Chemistry Chapter 4 Class 11 – Chemical Bonding
- If singlet electron linkages exist, then nitrogen would also have formed pentahalides. Although the concept of singlet electron linkage explains the formation and properties of a few molecules, it fails in most of the cases octet occurs for them.
- Group 16 elements like S, Se, etc., belonging to third, and fourth, periods form covalent compounds in which the normal valency of the elements is 2 and higher valencies of the elements are 4 and 6.
- In normal valency, those elements have fulfilled octet. In higher valencies, octets occur. Group 17 elements like Cl, III, I (tie, belonging to third, fourth, fifth….. form covalent compounds In
Ionic distortion and development of covalent character In Ionic compounds:
- Fajan’s rule hikes several covalent compounds possessing ionic characters, many Ionic compounds are also found to carry a partial covalent nature.
- For example, Is an Ionic compound hut due to its significant covalent character, It Is more soluble in organic solvents water.
Development of covalent character in an ionic compound:
When two oppositely charged Ions approach each other, the cation attracts the electron cloud of the anion but repels Its nucleus.
- This results in distortion of (the electron cloud around the anion.
- This Is known as the polarisation of the anion.
- The power of the cation to polarise the anion Is called Its polarising power.
- The tendency of the anion to get polarised by the cation is called Its polarisability. Such polarisation results In the transportation of electron cloud towards the cation to produce an overlapping zone.
- Consequently, the Ionic character of the bond decreases and the covalent character increases. The following picture shows the gradual development of covalent character with an increase in polarisation.

It is to be noted that the reverse polarisation of the cationic charge cloud by the anion will indeed be very small, as the cation has a more compact charge cloud.
The polarising power of the cation is expressed by the term ‘ionic potential: It is the ratio of charge to radius of the corresponding cation and is expressed by the sign, (Phi). Thus,
⇒ \(\text { Ionlc potential, } \phi=\frac{\text { Charge of the cation }}{\text { Radlus of the cation }}\)
On moving front from left to right In a period, the charge of the cation Increases while Its radius decreases. This results In an Increase lu the value of phi.
⇒ \(\text { For example, } \phi\left(\mathrm{Na}^{+}\right)<\phi\left(\mathrm{Mg}^{2+}\right)<\phi\left(\mathrm{Al}^{3+}\right)<\phi\left(\mathrm{Si}^{4+}\right)\)
On the other hand, on moving down the group the cationic charge remains unaltered but the cationic radius increases. Consequently, the value of decreases. For example
⇒\(\phi\left(\mathrm{LI}^{+}\right)>\phi\left(\mathrm{Na}^{+}\right)>\phi\left(\mathrm{K}^{+}\right) ; \phi\left(\mathrm{Be}^{2+}\right)>\phi\left(\mathrm{Mg}^{2+}\right)>\left(\mathrm{Ca}^{2+}\right)\)
In the case of some metals with different oxidation states, the value of phi Increases with an Increase In oxidation number,
⇒ \(\text { For example, } \phi\left(\mathrm{Sn}^{2+}\right)<\phi\left(\mathrm{Sn}^{4+}\right) ; \phi\left(\mathrm{Fe}^{2+}\right)<\phi\left(\mathrm{Fe}^{3+}\right)\)
With an Increase In the value of <p, the polarising power of the cullon increases which ultimately Increases the covalent character of the Ionic compound.
Fajan’s rule:
The polarising power of the cation and the polarisability of the anion (i.e., the extent of polarization causing the development of covalent character in an ionic compound) are governed by certain rules known as Fajan’s rules.
According to these rules, the covalent character of an ionic compound depends on the following factors:
Size of the cation:
For the cations having the same charge, the value Φ increases with a decrease in the size of the cation. Hence, the deformation of the anion increases which in turn enhances covalency. From the table given below, it is observed that the melting point decreases (i.e., the covalent character of anhydrous chlorides of alkaline earth metals increases) with a decrease in the radii of the cations.

The melting point however decreases from NaCl to KCl to RbCl, due to successive decreases in in the lattice energy.

Size of the anion: In a large-sized anion:
- The outermost electrons are less tightly held by the nucleus and hence, would be more easily distorted by the cation.
- Thus, the larger the anion, the higher its polarisability and the greater the covalent character of the compound formed.
The following table shows that the melting points decrease (i.e., the covalent character of the anhydrous calcium halides increases) with the increase in the size of the anion.

The greater amount of charge on the cation or anion:
The ionic potential Φ of the cations increases with an increase in cationic charge and a decrease in cationic radii. Consequently, the resulting compound is found to possess a more covalent character. It becomes evident.

As the charge on an anion increases, valence electrons become more loosely held by the nucleus and therefore, it gets more easily deformed by the cation. Thus, the greater the charge on an anion, the higher its polarisability, and the greater the covalent character of the compound formed.
Chemical Bonding Class 11 Notes
Configuration of cation:
- Between the two cations having the same size and charge, the one with 18 electrons in the outermost shell (S2p6d10) i.e., with pseudo noble gas configuration, has greater polarising power than the other with 8 electrons in the outermost shell (S2p6), i.e., with noble gas configuration.
- This is because, in the case of cations having 18 valence electrons, there is a poor screening effect due to the presence of d electrons.
- Thus, a more effective nuclear charge polarises the anion to a greater extent causing the development of a more covalent character in the compound formed, the following table shows that the melting points of the anhydrous chlorides of coinage metals are less compared to those of the anhydrous chlorides of alkali metals with noble gas electronic configuration.
The chlorides of Cu, Ag, and Au, therefore, possess a greater covalent character.

The dielectric constant of the medium:
A polar medium possessing a high dielectric constant tends to weaken electrostatic forces of attraction existing between oppositely charged ions. As a result, ions remain separated in a polar medium and effective polarisation does not take place.
However, effective polarisation takes place in a nonpolar medium having a low dielectric constant. Hence, an ionic compound exhibits more covalent character in a non-polar medium than in an apolar medium.
Effect of polarisation on the properties of compounds
- Solubility: As polarisation increases, the covalent character as well as the tendency of ionic compounds to get dissolved in non-polar solvents increases.
- Solubility of silver halides (AgX) in water: Order of polarisability of halide ions: I¯> Br¯ > Cl¯ > F¯ (polarisability increases with increase in size).
- Therefore, the covalent character of silver halides follows the order: Agl > AgBr > AgCl > AgF, i.e., the ionic character of these halides follows the reverse order. Consequently, the solubility of silver halides in the polar solvent, water, follows the order: AgF > AgCl > AgBr > Agl.
- Solubility of KC1 and K1 in alcohol: Since I¯ ion is larger than Cl¯ ion, I¯ gets more easily polarised than Cl¯. So, KI possesses more covalent character compared to KC1 and thus, it is more soluble in alcohol (a less polar solvent having low dielectric constant) compared to KC1.
- Thermal stability of metal carbonates: For the carbonates of Be, Mg, and Ca belonging to group-2 and possessing common anion (CO3), ionic potential (cf2) of the cations follows the order: Be2+ > Mg2+ > Ca2+.
So, the ionic nature of these compounds runs as follows:
BeCO3 < MgCO3 < CaCO3. Thus, their thermal stability follows the order: of BeCO3 < MgCO3 < CaCO3. Therefore, on moving down a particular group, the thermal stability ofthe metal carbonates gradually increases.
Color of different salts of metal:
- The tendency of the anions to get polarised increases with an increase in size. This facilitates the transition of electrons from the filled orbital of anions to the unfilled orbital of cations.
- The energy required for the electronic transition of an anion having high polarisability is lower than the energy required for that having low polarisability.
- Anions having high polarisability obtain the energy required for the electronic transition from the visible range while those with low polarisability, from the ultraviolet region.
- Thus the compounds having anions with high polarisability, are generally colored, depending on the wavelength absorbed, while those having anions with low polarisability are generally white.
For example, HgCl2 is white but Hgl2 is red; AgCl is white but Agl is yellow; PbCl2 is white, but Pbl2 is golden yellow.
- Non-existence of compound: PbCl4 exists but Pbl4 has no existence. In Pbl4, the charge on the cation, Pb4+ is much higher and it strongly polarises the large anion, I-.
- The degree of polarisation is so high that the two I- ions are oxidized to the I2 molecule by donating two electrons and the Pb4+ ion is reduced to the Pb2+ ion by gaining two electrons.
⇒ \(\stackrel{+4}{\mathrm{PbI}_4} \rightarrow \stackrel{+2}{\mathrm{PbI}_2^{-1}}+\stackrel{0}{\mathrm{I}}_2\)
Hence, Pbl4 does not exist. On the other hand, PbCl4 exists as the degree of polarization of relatively small Cl¯ is not very high, and hence no such electron transfer occurs. For the same reason, Fel3 does not exist but Fel2 does.
Coordinate Covalency Bond And Coordinate Bond Or Dative Bond
In 1921, Perkins suggested a special type of covalency known as coordinate covalency.
Coordinate Covalency:
Coordinate Covalency is a special type of covalent bond in which the shared pair is contributed by only one of the two combining atoms. This electron pair is shared by both of the combining atoms due to which both of them attain octet and the valency hence generated is called coordinate covalency.
Coordinate Bond:
A coordinate bond is a special type of covalent bond in which the shared pair of electrons is contributed by one of the two combining atoms.
Coordinate Compounds Compounds
- A coordinate bond is formed between two atoms, one of which has completed its octet and the other is short of two electrons to complete its octet.
- The former atom which donates a pair of electrons (lone pair) is known as the donor and the latter atom which accepts the electron pair to complete its octet is known as an acceptor.
- A coordinate bond is represented by an arrow pointing from the donor towards the acceptor Like a covalent bond, a coordinate bond is formed by overlapping of atomic orbitals of two atoms.
- As the atomic orbitals have specific orientations in space, coordinate bonds also have specific orientations in space. Note that a coordinate bond once formed cannot be distinguished from a covalent bond.
Conditions for the formation of coordinate bonds
- The donor atom must contain at least one lone pair of electrons in its valence shell.
- The acceptor atom must have at least one vacant orbital in its valence shell where the lone pair of electrons from the donor atom can be accommodated.
- The lone pair of the donor atom must be equally shared by both the donor and the acceptor atoms.
The electron pairs, which present the valence shell ofthe atoms or ions, which do not participate in the bond formation are termed ‘lone pairs of electrons.

For example, N-atom in NH3 molecule and O-atom in H2O molecule The molecules having atoms with lone pair of electrons e.g., ammonia (NH3), water (H26), methyl amine (CH3NH2), aniline (CgH5NH2), phosphine (PH3), triphenylphosphine (PH3P), alcohols (ROH), phenol (C6H5OH), diethyl ether (C2H5OC2H5), etc.] act as a donor in the coordinate bond formation.
On the other hand, hydrogen ions (H+) or molecules having atoms with electron sextet (e.g., BF3, BH3, etc.), or metal ions containing vacant orbital in their valence shell act as acceptors in the coordinate bond formation.
Mechanism for the formation of coordinate bond
The donor atom transfers one electron of its lone pair to the acceptor atom and as a result, the donor atom acquires a positive charge and the acceptor atom acquires a negative charge.

The two ions then contribute one electron each and this electron pair is shared by both the atoms to form a single covalent bond between them.
⇒ \(\stackrel{+}{\mathrm{A}}+\stackrel{\rightharpoonup}{\cdot} \longrightarrow \stackrel{+}{\mathrm{A}}: \overline{\mathrm{B}} \text { or } \stackrel{\mathrm{A}}-\overline{\mathrm{B}} \text { or } \mathrm{A} \rightarrow \mathrm{B}\)
Thus, the formation of a coordinate bond involves the transfer of electrons (as in the formation of an electrovalent bond) as well as the sharing of electrons (as in the formation of a covalent bond). Therefore, a coordinate bond may be regarded as a combination of a polar electrovalent bond and a non-polar or less polar covalent bond. For this reason, a coordinate bond is termed a semipolar bond.
Examples of coordinate bond formation:
Formation of an addition compound (complex) involving ammonia and boron trifluoride: In ammonia (NH3), the nitrogen atom has a lone pair and the boron atom in boron trifluoride (BF3)is short of two electrons to achieve its octet.

Therefore, when NH3 is subjected to react with BF3, the N-atom donates its lone pair to the Batom to form a coordinate bond which holds them together forming the addition compound, \(\mathrm{H}_3 \mathrm{~N} \rightarrow \mathrm{BF}_3.\)
An ion or a molecule that can donate an electron pair is called a Lewis base and an ion or a molecule that can accept an electron pair is called a Lewis acid. In the above example, ammonia is a Lewis base while boron trifluoride is a Lewis acid.
Class 11 Chemistry Chapter 4 Notes
Formation of ammonium ion (NH+4 ): [Donor: N-atom of NH3 molecule, Acceptor: H+-ions]

- From experimental observations, it can be said (bat all the four N— 1-1 bonds in ammonium ions are equivalent.
- So the ammonium ion can be represented as shown above.
- This concept is also applicable to those compounds in which coordinate bonds are present.
Formation of fluoroborate ion (BF–4): [Donor: F– -ion, Acceptor: B -atom of BF3 molecule]

Formation of hydronium ion or hydroxonium ion (H3O+): [Donor: O-atom of H2O molecule, Acceptor: H+-ion]

Formation of ozone molecule (O3): [Donor: Central O-atom, Acceptor: Terminal O-atom]

Formation of the sulphuric acid molecule (H2SO4): [Donor: S-atom, Acceptor: O-atom]

Formation of the nitric acid molecule (HNO3): [Donor: N atom, Acceptor: O-atom]

Formation of Al2Cl6 (dimer of aluminium chloride): [Donor: Cl-atom, Acceptor: Al-atom]

Formation of an orthophosphoric acid molecule (H3PO4) : [Donor: P-atom, Acceptor: O-atom

Formation Of ammonium chloride (coexistence of electrovalent valency, covalency, and coordinate valency):
Ammonia reacts with an aqueous solution of hydrogen chloride to form ammonium chloride. In the HCl molecule, the highly As a result, polarity develops in the H—Cl bond.
In the presence of H2O molecules, the polar H —Cl bond undergoes dissociation forming the H+ ion and Cl ion. The O-atom of H2O donates a pair of electrons to H+ to produce hydroxonium ion (H3O+) through the formation of a coordinate bond.
In the NH3 molecule, since the N-atom is less electronegative than the O-atom, it exhibits a greater tendency to donate its unshared pair. So, NH3 accepts a proton (H+) from H3O+ and produces an NH4 ion by forming a coordinate bond.

The NH4 ion thus formed combines with Cl- ion through electrostatic force of attraction to produce crystals of NH4Cl.
Thus, in NH4Cl, three H -atoms are attached to the N-atom by three covalent bonds, the fourth H-atom is attached to it by a coordinate bond and the two ions (NH4 and Cl-) are held together by an ionic bond, i.e., in NH4Cl, there exists electrovalency, covalency and Coordinate covalency. Some other examples of this type of compound are LiAlH4, NaBH4, Na2HPO4, etc.
Chemical Bonding And Molecular Structure Class 11
Characteristics of coordinate compounds
Coordinate bonds are a special type of covalent bond and coordinate compounds are in fact, covalent compounds. Hence, the characteristics of coordinate compounds are similar to those of the covalent compounds.
Some of their important characteristics are described below:
- Physical state: Coordinate compounds exist as gases, liquids, and solids under ordinary conditions.
- Melting and boiling points: Coordinate bonds are semipolar. Due to this, coordinate compounds are more polar than covalent compounds but less polar than ionic compounds.
- Consequently, the melting and boiling points of these compounds are usually higher than those of covalent compounds but lower than those of ionic compounds.
- Solubility: Coordinate compounds are usually insoluble or less soluble in polar solvents like water but soluble in non-polar (organic) solvents.
- Electrical conductivity: Coordinate compounds do not ionize in a fused state or solution and hence, these compounds do not conduct electricity.
- Isomerism: Since coordinate bonds are rigid and possess directional properties, coordinate compounds exhibit the property of isomerism.
- Type of relictions: Court in compiles undergoes molecular reactions which are much slower than those of ionic reactions.
Similarities and dissimilarities between covalent and coordinate bonds δ

Some Important Bond Parameters
Covalent bonds are characterized by certain parameters such as bond length, bond dissociation enthalpy or bond enthalpy, and bond angle.
Bond length
- Bond length is defined as the equilibrium distance between the centers of the nuclei of two bonded atoms in a covalent molecule.
- The bond lengths of different covalent bonds are determined by X-ray diffraction electron diffraction or spectroscopic methods. For a covalent bond, it is the sum of the covalent radii of the bonding atom.
- For example, if in a covalent molecule A — B, rA, and rB are the covalent radii of the atoms, A and B respectively, and the bond length is d, then d = rA + rB.
- It is generally expressed in terms of angstrom (lA = 10-10m) picometer (1 pm = 10‾12m).

Factors affecting bond length: Bond length depends on the following factors.
- Size of the atoms: Bond length increases with an increase in the size of the atoms. For example, bond lengths of —X
- Follow the order: H—I > H—Br > H—Cl > H—F.
- This is because the order of covalent radii of halogen atoms follows the sequence: I > Br > Cl > F.
- Bond multiplicity: Bond length decreases with an increase in multiplicity.
Bond lengths of different carbon-carbon bonds follow the order:
C=C (120 pm) < C=C(134 pm) < C—C(154 pm)
Types of hybridization (discussed later in article 4.8):
- Any s-orbital is closer to the nucleus than a p -p-orbital. So, electrons in the s -s-orbital are more tightly held by the nucleus than the electrons in the p-orbital.
- For this AATB [covalent molecule] [atoms or free radicals] A + B reason, with an increase in s -the character of the hybrid orbital the attraction on the electron increases and so, the length of the hybrid orbital decreases.
- As a consequence, the length of the bond obtained by overlapping the hybrid orbital with the s -s-orbital of another atom decreases.
- The s -characters of sp³, sp², and sp orbital are 25%, 33.33%, and 50% respectively.
Thus, the lengths of C—H bonds involving C -atoms with different hybridizations follow the order:
Electronic effects:
Bond length also depends on resonance, hyperconjugation, aromaticity, etc. For example, due to resonance, the carbon-carbon bond length in benzene is 1.39A while in the case of ethylene, the carbon-carbon bond length reduces to 1.34Å.

Bond dissociation enthalpy or bond enthalpy
- When a bond is formed between two atoms, some amount of energy is released. The same amount ofenergy is required to break the bond to get the atoms separated.
- This is called bond dissociation enthalpy which is a measure of bond strength and may be defined as the amount of energy required to break be gaseous state to produce neutral gaseous atoms or be gaseous state to produce neutral gaseous atoms or free radicals.
The bond dissociation enthalpy is usually expressed kJ.mol¯¹. It is to be remembered that the greater the bond dissociation enthalpy, the stronger the bond.

When a compound contains two or more same type of bonds, the average of their bond dissociation enthalpies is considered as bond enthalpy or bond energy.
Example: Bond dissociation enthalpies of four C — H bonds of a methane molecule (CH4) are 435.7, 444.14, 444.14, and 339.4 kj.mol¯¹.
Therefore, the average value of bond dissociation enthalpies of four C-H bonds = (435.7 + 444.14 + 444.14 + 339.4)/4= 415.84 kj-mol-1.
This average value of bond dissociation enthalpy is the bond enthalpy or bond energy of the C — H bond of methane. In the case of diatomic molecules like H2, Cl2, O2, N2, HC1, etc., the bond dissociation enthalpy and bond enthalpy are the same. For example, the bond dissociation enthalpy and bond enthalpy of chlorine (Cl—Cl) molecule are the same (247 kj.mol¯¹ ).
Factors affecting bond dissociation enthalpy:
- Size of the bonded atoms: The larger the size of the bonded atoms, the greater the bond length and less the bond dissociation enthalpy. Thus, the bond enthalpy decreases on moving down a group in the periodic table. For example, the bond dissociation enthalpy of the H —Cl bond (431 kj.mol¯¹) is larger than the bond dissociation enthalpy of the H—Br bond (368 kj.mol¯¹ ).
- Bond multiplicity: The Greater the bond multiplicity, the greater the bond dissociation enthalpy of the bond between two atoms.
- For example—C—C < C=C < C=C; N—N <N=N < N=N
- No. of lone pairs of electrons on the bonded atoms: As the number of lone pairs of electrons present on the bonded atoms increases, the electron-electron repulsion between the lone pairs of electrons on the two atoms increases. Thus, bond dissociation enthalpy decreases.
For example: Bond dissociation enthalpies of C—C (with no lone pair), O —O (with 2 lone pairs on each atom), and F—F bond (with 3 lone pairs on each atom) follow the order:
C—C (377 W-mol¯¹) >(213kj- mol¯¹ > F—F (159 kj-mol¯¹ ).
Types of hybridization: Bond enthalpy increases with an increase in s -character but decreases with an increase in p -character of the hybrid orbitals.
For example: C(sp) —C(sp) (435.1 kj.mol¯¹) > C(sp²)—C(sp²) (384.6 kl-mol-1) > C(sp³)—C(sp³) (347.6 kj.mol¯¹).
Types of bond:
The bond enthalpy of a sigma (cr) bond is greater than that of an api (r) bond.

Bond angle
The bond angle is defined as the angle between two bonds around the central atom in a molecule. For example, the H — C —H bond angle in methane (CH4) is 109°28′, the H — N —H bond angle in ammonia (NH3) is 107.3° and the H — O —H bond angle in water (H2O) is 104.5°.

Factors affecting bond angle:
- Types of hybridization: The bond angle depends on the type of hybridization of the central atom in a molecule. For example, in the case of sp3 -hybridization of carbon, the bond angle is 109°28′, for sp2 -hybridization, it is 120°, and for sp -hybridization, it is 180°.
- Number of lone pairs of electrons: As the number of lone pairs of electrons present on the central atom increases, the bond angle decreases.
- Electronegativity of the central atom: As the Electronegativity of the central atom of a molecule of type ABx increases the bond angle increases.
- Electronegativity of the atoms hooded to the central atom: As electronegativity of the atom bonded to the Shape of the molecule Hood angles central atom of a molecule of AB- type decreases, the bond angle Increases.
[The last three points are discussed later in VSEPR theory.]
CBSE Class 11 Chemistry Chapter 4 Notes
Shapes Of Covalent Molecules And Valence Shell Electron Pair Repulsion (VSEPR) Theory
As already mentioned, Lewis’s concept is unable to explain the shapes of molecules. The first simple theory providing the simple procedure to predict the shapes of covalent molecules is known as the Valence Shell Electron Pair Repulsion (VSEPR) theory. The theory was proposed by Sidgwick and Powell in 1940 and was further developed by Nyholm and Gillespie in 1957. VSEPR theory may be expressed in terms of the following five rules:
Rule 1:
The shape of a molecule depends on the total number of valence shell electron pairs i.e., the total number of bond pairs and lone pairs of electrons or steric number (SN) around the central atom. All electron pairs repel each other. To minimize repulsions, the electron pairs tend to occupy a geometrical position such that the angular distance between them is maximum.
If the central atom of the n molecule does not possess a pair of electrons, the geometry of the molecule will be regular ami Is determined only by the bond pairs.
Number of bond pairs and shapes of molecules

Rule 2:
If the central atom Is surrounded by bond pairs as well as lone pairs of electrons, the repulsions among themselves are different. As a result, the molecule possesses an irregular or distorted geometry.
The repulsive interactions of various electron pairs decrease in the order:
Lone pair-lone pair (Ip-lp) > lone pair-bond pair (Ip-bp) > bond pair-bond pair {bp-bp).
When the angle between two electron pairs increases, the extent of repulsion decreases. These repulsions are found to be relatively greater If the electron pairs are to each other. If the angle between them Is 120° the repulsion becomes comparatively weaker and at 180° It Is the minimum.
Effect of lone pairs of electrons:
Nyholm and Gillespie (1957) pointed out that there is an important difference between the lone pair and the bond pair.
- While a lone pair is localized on the central atom (i.e., it is under the influence of only one atom), each bond pair is shared between two atoms.
- As a consequence, a lone pair occupies more space compared to a bond pair. This results in greater repulsive interactions between two lone pairs as compared to lone pair-bond pair and bond pair-bond pair repulsions.
- For example, In a CH4 molecule, the C -atom contains four electron pairs in its valence shell and they are situated tetrahedrally.
- Thus, CH4 is a regular tetrahedron with H —C —H bond angles of 109°28′. But, in the case of NH3, the central N atom contains 3 bond pairs and 1 lone pair of elections, and as die Ip-bp repulsion is greater than that of bp-bp repulsion, the H —N —2 bond angle shrinks from 109°28´ lo 107.3°, In H2, O-atom possesses 2 lone pairs along will) 2 bond pairs.
- Due to the strong repulsive forces of these two lone pairs acting on each bond pair, the — O —H bond angle significantly reduces to 104°2B´.
Rule 3:
- As the electronegativity of the hooded atoms for the central atom increases, the extent of repulsion between two bond pairs decreases and this is because the electron pairs are shifted away more from the central atom towards the bonded atoms.
- On the contrary, if the electronegativity of the central atom increases the electron pairs move towards the central atom giving rise to an increase in repulsion between the bond pairs.
Example:
The lone pairs and the bond pairs are tetrahedrally arranged in both NH3 and NF3 molecules. In the NF3 molecule, the N —p bond pair is drawn more towards the more electronegative F-atom. But in the NH3 molecule, the N — 11 bond pair is drawn more towards the more electronegative N -atom.
Therefore, bp-bp repulsion in NH3 is more than that in NF3.
Consequently, there is more distortion in NF3 (F—N—F bond angle:
- 102°29′ when compared to the NH3 molecule (H —N — H bond angle: 107.3°).
- For the same reason, the bond angle of H2O (104.5°) is greater than that of F2O (102°).
Rule 4:
The effect of electrons involved in the formation of a π-bond is not generally considered in determining the geometrical shape of a molecule.
- The electron cloud of a JI -bond is not tightly held by the nuclei of two atoms like that in a rr -bond.
- Therefore, a triple bond (one rr and two r -bonds) and a double bond (one a and one n -bond) occupy more space than a single bond.
- So, a multiple bond causes more repulsion than a single bond and the order is: multiple bond-multiple bonds> multiple bond single bond > single bond-single bond.
Example:
In the ethylene (CH2=CH2) molecule, the H—C—H bond angle reduces from 120° to 116° because of greater repulsion between the C —H and C=C bonds. For a similar reason, the Cl—C—Cl bond angle in phosgene (COCI2) reduces to 112°.
Two exceptional cases:
PH3(94°) < PF3(98°):
- Fluorine is more electronegative than hydrogen. So, according to rule III, the order of bond angles is expected to be the reverse [NF3(102.2°) <NH3 107.3°). This can be explained in terms of bond multiplicity.
- A coordinate covalent pn-dn bond is found to be formed between a filled 2p -orbital of F and an incomplete 3d -orbital of P.
- Due to resonance, each P —F bond in PF3 assumes a partial double bond character.
- Consequently, the P —F bond order becomes greater than 1, i.e., its multiplicity increases.
With the increase in bond multiplicity, repulsion between bond pairs increases and consequently, the F—P—F bond angle becomes greater than the H —P —H bond angle.

In the PH3 molecule, on the other hand, similar coordinate covalent n-bond formation is not possible because hydrogen has no unshared electron pair.
F2O(102°) < H2O(104.5°) < C12O(111°):
The increasing order of electronegativity of the terminal atoms of these compounds is H < Cl < F.
Therefore, the order of bond angles should be:
F2O< Cl2O< H2O. In this case, also, the correct order of bond angles can be explained in terms of bond multiplicity.
The coordinate covalent pn-dn bond is formed between the filled 2p -orbital of an oxygen atom and the vacant 3d -orbital chlorine atom and because of resonance, each O—Cl bond possesses a partial double-bond character. Due to an increase in bond multiplicity, the repulsive force operating between bond pairs increases and as a result, the value of the bond angle increases.

As there is no vacant orbital in the valence shells of hydrogen and fluorine, the formation of similar π-bonding is not possible. Therefore, it is the electronegativity of the terminal atoms which decides the bond angles of H2O and F2O.
Rule 5:
The unshared electron pair on a central atom having an incomplete valence shell (i.e., with vacant d-orbital) causes greater repulsion towards bond pairs or other lone pairs resulting in a significant contraction in bond angle compared to that on a central atom having a complete valence shell.
Example:
- There is no vacant orbital in the valence shells of the elements such as C, N, and O belonging to the second period of the periodic table.
- These elements can accommodate four electron pairs in their valence shells which are tetrahedrally arranged.
- In such cases, the repulsive interaction caused by the lone pair is less and this results in a small deviation in bond angle. For example, in an NH3 molecule, the H —N — H bond angle is 107.3° and in H2O, the H — O — H bond angle is 104.5°.
- On the other hand, the elements such as Si, P, and S belonging to the third period have vacant d -d-orbitals in their valence shells. If four electron pairs in their valence shells are tetrahedrally placed, then as a result of stronger repulsion by the lone pairs, considerable contraction in bond angle occurs.
- In fact, due to the availability of larger space, repulsion between bond pairs decreases and the stronger lone pair-bond pair repulsion compresses the bond angle almost to 90°. For example, in PH3 and H2S, the bond angles, instead of being 109°28´, are reduced to 94° and 92° respectively.
Determination of shapes of molecules and ions by valence shell electron pair repulsion (VSEPR) theory
A central atom having 2 electron pairs in its valence shell:
1. Beryllium chloride (BeCla) molecule:
In BeCl2, the total number of electrons in the valence shell of the central Beatom = 2 valence electrons of Be-atom + 2 electrons of two Cl-atoms involved in cr -bond formation = 4 electrons = 2 electron pairs of = 2 cr -bond pairs.
These two bond pairs experience minimum repulsion when they remain at an angle of 180°. Hence, the shape of the BeCl2 molecule is linear.
2. Carbon dioxide (CO2) molecule:
The total number of electrons in the valence shell of the central C -atom of CO2 molecule = 4 valence electrons of C -atom +4 electrons of two doubly-bonded O-atoms = 8 electrons = 4 electron pairs = 2cr -bond pairs + 2n -bond pairs, π-bond pairs have no role in determining the shape of a molecule. Therefore, the shape of the molecule is determined only by the two cr bond pairs.
Repulsion between these two bond pairs is minimal if they exist at an angle of 180°. Hence, the angular distance between two C=0 bonds is 180°, i.e., the shape ofthe CO2 molecule is linear.
[The shape of the carbon disulfide (S=C=S) molecule is also similar to that of the carbon dioxide molecule.]
3. Hydrogen cyanide (HCN) molecule:
In the HCN molecule, the total number of electrons in the valence shell of the central C -atom = 4 valence electrons of C-atom +3 electrons of one triply-bonded N -atom +1 electron of one singly-bonded H atom= 8 electrons = 4 electron pairs -2a -bond pairs +2 7T -bond pairs, n -bond pairs play no role in determining the shape of a molecule.
The two bond pairs experience minimum repulsion when they remain at an angle of 180°. Hence, the shape of the molecule is linear.

4. Acetylene (HC=CH) molecule:
The number of electrons surrounding each carbon atom of acetylene molecule = 4 valence electrons of carbon atom +3 electrons of one triply-bonded C-atom +1 electron one singly-bonded H -atom=8 electrons =4 electron pairs =2 a -bond pairs +2n bond pairs.
To minimize the force of repulsion between the bond pairs, the shape of the acetylene molecule is linear.

. A central atom having 3 electron pairs in its valence shell: Boron trifluoride (BF3) molecule:
The total number of electrons in the valence shell ofthe central B-atom of BF3 electron of b- atom +3 electron of three sin gly bonded f atoms =6 elctron3 electron pair trigonal planar bf3 Molecule= 3 bond pairs.
The three bond pairs experience minimum repulsion if they remain at a 120° angle concerning each other.

1. Therefore, the geometrical shape of BF3 is trigonal planar Nitrate (NOg) ion:
The total number of electrons surrounding the N -atom of NO2 ion =5 valence electrons of N-atom + 2 electrons of one doubly-bonded O-atom +1 electron of one singly-bonded O -atom (no electron from the O-atom.
Attached by a coordinate bond because bond oxygon In or deb iron bond n-bond only, loud puli plays no rob In the dimming shape of Ion, bond pahs, To minimize repulsion among hinted towards Trigonal planar of a triangle, nil NO bond minimi are 120-, Honca, the shape of Ion In trigonal planar.
2. Sulfur (NO2) molecules In HO2 molecule:
Electrons surrounding Central H -atom valence electrons of 8-atom 2 electrons of one doubly-hooded O-aloin (no electron from the O-atom a coordinate covalent bond) electrons or 4 electron pair n 2 <r -bond 11 lone pair r 1 n -bond pair. The n-bond pair has no role In determining the shape of the molecule.
To minimize the extent of repetition, 2 electron palms are oriented toward the corners of an equilateral triangle. However, because of greater lone pair-bond pair repulsion compared to bond pair-bond pair the— S — 0 bond angle IN reduced from 120° to 119.5°. Thun, SO molecule is angular.
The n-bond pair has no role In determining the shape of the molecule. To minimize the extent of repetition, 2 electron palms are oriented toward the corneum of an equilateral triangle. However, because of greater lone pair-bond pair repulsion compared to lo bond pair-bond pair population, the — S — 0 bond angle IN reduced from 120° to 119.5°. Thun, SO2 molecule IN angular

3. Ammonium (NH3) Molecule:
Ion, the total number of electrons surrounding the central N-atom i.e., In Its valence shell 3 valence electrons of N-atom +3 electrons of three singly-bonded H-atoms (no electron from the Hatom attached by a coordinate covalent bond) =8 electrons or 4 electron pairs =4 rr -bond pairs.
To Ammonium to be torn In NH Ion, the total number of electrons surrounding the central N-atom i.e., In Its valence shell 3 valence electrons of N-atom +3 electrons of three singly-bonded H-atoms (no electron from the Hatom attached by a coordinate covalent bond) =8 electrons or 4 electron pairs =4 rr -bond pairs. To 107.3°, i.e., the tetrahedron is somewhat distorted. Excluding the lone pair, the shape of the molecule is trigonal pyramidal.

4. Water (H2O) molecule:
In an H2O molecule, the total number of electrons surrounding the central O-atom = 6 valence electrons of O-atom +2 electrons of two singly-bonded Hatoms =8 electrons or 4 electron pairs =2o- -bond pairs +2 lone pairs. To minimize the extent of mutual repulsion, these four electron pairs are oriented towards the four comers of a tetrahedron.

However, the tetrahedron is somewhat distorted due to the strong repulsive forces exerted by the lone pairs on each bond pair of electrons. The H —O —H bond angle is reduced to 104.5° from the normal tetrahedral angle of 109°28′. Excluding the lone pairs, the shape of the molecule is angular or V-shaped.

5. Hydrogen sulfide (H2S) molecule:
In an H2S molecule, the total number of electrons surrounding the central S-atom =6 valence electrons of S-atom +2 electrons of two singly bonded H-atoms =8 electrons or 4 electron pairs =2crbond pairs +2 lone pairs.
These 4 electron pairs experience minimum repulsion if they occupy the four comers of a tetrahedron. Since the repulsion between two lone pairs is greater than that between two bond pairs, the tetrahedron is distorted and the H — S — H bond angle is decreased to 92° from the ideal tetrahedral angle (109°28′).
Due to the presence of vacant d -d-orbital in S-atom, the bond angle, in this case, reduces significantly. Therefore, excluding the lone pairs, the shape of the molecule is angular or V-shaped.

A central atom having 5 electron pairs in its valence shell:
1. Phosphorus pentachloride (PCI5) molecule:
In the PCl5 molecule, the total number of electrons surrounding the central P-atom =5 valence electrons of P-atom +5 electrons of five Cl-atoms =10 electrons or 5 electron pairs =5<r -bond pairs. These electron pairs experience minimum mutual repulsion if they orient themselves towards the five vertices of a trigonal.
In this geometry, all five P—Cl bonds are not equivalent. The three bonds lying In the trigonal plane are called equatorial bonds. The remaining two bonds, one lying above and the other below the trigonal plane and both making an angle of 90° with the plane, are called axial bonds. The axial bonds arc slightly longer than the equatorial bonds.

It is to be noted that the structure of the PC15 molecule is unsymmetrical. As a result, it is less stable and therefore, is more reactive.

2. An axial bond is longer than an equatorial bond:
It can be explained in terms of repulsive forces between electron pairs due to different bond angles. Let us consider the repulsive interactions experienced by an axial and an equatorial bond pair. An axial bond pair is repelled by three equatorial bond pairs at 90° and one axial bond pair at 180°.
On the other hand, an equatorial bond pair is repelled by two axial bond pairs at 90° and two equatorial bond pairs at 120°. It is known that the repulsion between two electron pairs decreases with an increase in the angle between them and hence, the repulsion between electron pairs at 120° and 180° may be neglected in comparison to hose at 90°.
Thus, considering only the repulsive interactions between electron pairs situated at 90° to each other, we find that each axial bond pair is repelled by three electron pairs while each equatorial bond pair is repelled by two electron pairs.
Therefore, an axial bond pair experiences greater repulsion than an equatorial bond pair and as a consequence, an axial bond becomes slightly longer than an equatorial bond.
Chemical Bonding Notes For NEET
3. Sulfur tetrafluoride (SF4) molecule:
In the SF4 molecule, the total number of electrons surrounding the central Satom = 6 valence electrons of S-atom +4 electrons of four F-atoms =10 electrons or 5 electron pairs =4 a -bond pairs +1 lone pair. Thus, to minimize the extent of repulsion, the five electron pairs around sulfur. Orient themselves in a trigonal bipyramidal geometry.
The lone pair preferably occupies the equatorial position to stabilize the structure. For such orientation of the lone pair, the trigonal bipyramidal structure is distorted (the bond angles are 89° and 177° instead of 90° and 180° respectively). Thus, the shape of the molecule is described as a distorted tetrahedron or a see-saw.

4. Chlorine trifluoride (CIF3) molecule:
In the ClF3 molecule, the total number of electrons surrounding the central Clatom =7 valence electrons of Cl-atom +3 electrons of three singly bonded F-atom = 10 electrons or 5 electron pairs =3 σ -bond pairs +2 lone pairs.
Thus, to minimize mutual repulsion, the five electron pairs orient themselves in a trigonal bipyramidal geometry in which two equatorial positions are occupied by two lone pairs. This is because, in such orientation, the structure acquires maximum stability. But, due to the presence of two lone pairs in the equatorial position, the trigonal bipyramidal structure is distorted (Ffl —Cl —Fe bond angle becomes 87°29′) and the molecule is T-shaped.

5. ICI2– ion:
In the ICl2 ion, the total number of electrons surrounding the central I-atom = 7 valence electrons of atom +2 electrons of two cr -bonded Cl-atoms +1 electron for the negative charge = 10 electrons = 5 = 2 electron pairs bond pairs and 3 lone pairs.
These five electron pairs arrange themselves in a trigonal bipyramidal geometry with three equatorial positions occupied by the three lone pairs because such an arrangement ensures maximum stability.

Since the three lone pairs are present at the comers of an equilateral triangle, there is no distortion of the Cl —I — Cl bond angle of 180°. Hence, the ion has a linear shape. Similar examples are XeF2.
A central atom having 6 electron pairs in its valence shell:
1. Sulfur hexafluoride (SF6) molecule:
In the SF6 molecule, the number of electrons surrounding the central S -atom = 6 valence electrons of the S -atom + 6 electrons of six σ bonded F-atoms = 12 electrons or 6 electron pairs = 6 cr-bond pairs.
To have the minimum force of repulsion, the six electron pairs are oriented towards the corners of a regular octahedron. Hence, the shape of the SF6 molecule is octahedral with a bond angle of 90°.

2. Bromine pentafluoride (BrF5) molecule:
In BrF5, the total number of electrons surrounding the central Br-atom = 7 valence electrons of Br-atom +5 electrons of five crbondedF-atoms = 12 electrons or 6 electron pairs =5 bond pairs +1 lone pair. To minimize the extent of mutual repulsion, these six electron pairs arrange themselves octahedrally in which any one of the positions (all positions are equivalent) is by the lone pair.
Due to the presence of a lone pair of electrons, the Br-atom slightly deviates from the equatorial plane. So, the BrFg molecule is square pyramidal. A similar example is IF5.

3. Xenon tetrafluoride (XeF4) molecule:
In the XeF4 molecule, the total number of electrons surrounding the central Xe-atom = 8 valence electrons of Xeatom + 4 electrons of four cr-bonded F-atoms =12 electrons or 6 electron pairs = 4 cr-bond pairs + 2 lone pairs. To minimize the extent of mutual repulsion, these electron pairs arrange themselves octahedrally in which two opposite axial positions are occupied by the two lone pairs. Therefore, the shape of the XeF4 molecule is square planar.

A central atom having 7 electron pairs In Its valence shell Iodine hepts (1F7) molecule/in IF7 molecule, the total number of electrons surrounding the central Iatom = 7 valence electrons ofI-atom +7 electrons of seven σ -bonded F-atoms = 14 electrons or 7 electron pairs – 7 σ-bond pairs.
To have the minimum force of repulsion, the seven electron pairs are oriented toward the corners of a pentagonal bipyramid. Hence, the shape of the IF7 molecule is pentagonal bipyramidal with bond angles of 72°, 90°, and 180°.

Shapes of different types of molecules or ions according to VSEPB theory



Modern Bond Concept(Vbt) Of Covalency Valence Bond Theory
The valence bond theory was given by W. Heitler and F. London in 1927 and was later improved and developed by L. Pauling and J. C. Slaterin in 1931. It is based on atomic orbitals, electronic configurations of elements, overlap criteria of atomic orbitals, and stabilities of molecules.
Basic characteristics of valence bond theory
- A covalent bond is formed by overlapping the atomic orbitals of the two combining atoms having unpaired electrons of opposite spin. Opposite spins of the two electrons are mutually neutralized during the formation of the covalent bond.
- The extent of overlapping of the two half-filled atomic orbitals determines the strength of a covalent bond. The greater the overlapping of atomic orbitals, the stronger the covalent bond formed.
- The atomic orbitals having only unpaired electrons are involved in overlapping.
- Multiple bonds are for median atoms possessing more than one atomic orbital containing unpaired electrons.
- Atoms do not lose their identity in the molecule formed by the combination.
- During bond formation, only the valence electrons of each bonded atom lose their identity. The other electrons remain unaffected.
- The formation of a bond is accompanied by the release of some energy. The larger the amount of energy released, the stronger the bond.
- The orientations of the atomic orbitals involved in the overlapping determine the orientation of the covalent bond formed.
Explanation of the formation of H2 molecule with the help of valence bond theory
Letus consider the formation of hydrogen molecule which is the simplest of all molecules. Consider two hydrogen atoms, A and B approaching each other having nuclei NA and Nfi respectively and their electrons are represented by eA and eB. When the two atoms are far apart from each other, there is no attractive or repulsive interaction between them, and the potential energy of the system (isolated atoms)is assumed to be zero. When the two atoms come closer to each other, new attractive and repulsive forces start operating. These are:
- The force of attraction between the nucleus and its electron i.e., NA– eA and NB– eB
- The force of attraction between the nucleus of B and electrons of A (NA-eB) and the nucleus of A and electrons of B (NA-eB), the
- The force of repulsion between nuclei ofthe two atoms (NB– eA ) and
- The Force repulsion between electrons of the two atoms (eA-eB)- The diagrammatic representation of these forces is given in

We know that attractive forces tend to bring the atoms closer while repulsive forces tend to push them apart.

It has been observed experimentally that the magnitude of new attractive forces is greater than the new repulsive forces. As a consequence, the potential energy of the system decreases gradually as the two atoms come closer and closer.
Finally, a stage is reached where the total force of attraction is just balanced by the total force of repulsion. In this situation, the two hydrogen atoms are said to be bonded together to form a stable molecule, and the distance (r0) between the two nuclei is called bond length which is equal to 74 pm.
If the two atoms are brought still closer, the repulsive forces predominate. As a consequence, the potential energy of the system increases and the system becomes unstable. Hence, the two hydrogen atoms cannot be brought closer than 74 pm. The change in potential energy takes place in the formation of a hydrogen molecule.
NCERT Class 11 Chemistry Chapter 4
Since a certain amount of energy is released when a bond is formed between the two H -atoms, the hydrogen molecule is more stable than the isolated hydrogen atoms.
⇒ \(\mathrm{H}(\mathrm{g})+\mathrm{H}(\mathrm{g}) \longrightarrow \mathrm{H}_2(\mathrm{~g})+435.8 \mathrm{~kJ} \cdot \mathrm{mol}^{-1}\)
The energy so released is known as bond enthalpy or bond energy. The larger the amount of energy released, the stronger the bond formed and vice-versa. Conversely, 435.8 kg of energy is required to break the bond, i.e., to separate the atoms in one mole of H2 molecules.
⇒ \(\mathrm{H}_2(\mathrm{~g})+435.8 \mathrm{~kJ} \longrightarrow \mathrm{H}(\mathrm{g})+\mathrm{H}(\mathrm{g})\)
It is to be noted that the decrease in energy of the system during the formation of a chemical bond determines the strength of the bond formed and vice-versa.
Non-existence of helium molecule:
- When two helium atoms (HeA and HeB ) approach each other, four new forces of attraction and five new forces of repulsion come into play.
- The old and new attractive as well as repulsive forces, Since the overall repulsive forces are more than the attractive forces, the energy of the system increases.
- Hence, the formation of a chemical bond between two atoms is not possible.

Atomic Orbitals
- The three-dimensional region in space around the nucleus of an atom where the probability of finding an electron is maximum is called an atomic orbital.
- The size and shape of any orbital depend on the energy of the electron present in that orbital, i.e., on the principal energy level and subshell in which the electron resides.
- According to the energy content of electrons, the orbitals are expressed as s, p, d, and f.
- With the increase in principal quantum number, the size of an orbital of the same type (i.e., s, p, d, or) increases.
S-orbital:
- It is the spherical three-dimensional region in space around the nucleus having a fixed radius where the probability of finding the electron is maximum. Electron density on the surface ofthe sphere is maximum.
- Although different s -orbitals (Is, 2s, 3s, etc.) are expressed as spheres of different radii, the density of the electron cloud is not the same throughout the sphere (as 1=0 and m – 0);
- For Example: For 2s -orbital, electron density increases upto some distance from the nucleus then decreases and again increases at the surface of the sphere.
- The intermediate space where the electron density is minimum is called a spherical node.
- 2s and 3s-orbitals contain one and two nodes respectively but the ls-orbital does not contain any node.

P-Orbital:
In the case of the p -subshell,l = 1 and m =-1,0 and +1.
- So, it consists of three orbitals, designated as px, py, and pz. From the solutions of Schrodinger’s wave equation, it is known that p -p-orbitals have three possible orientations along the x-axis, y-axis, and z-axis, mutually perpendicular to each other.
- Each orbital has two lobes, separated by a plane where the probability of finding the electron is zero.
- This plane is called the nodal plane and the point at which the two lobes meet indicates the position of the nucleus of the atom and is called the node of the orbital. Each orbital is thus dumbbell-shaped.
- The electron density is maximum on the surface of the dumbbell. Being situated along the three axes, they have definite directions. Spatial orientations of px, py, and pz.

D-orbital: In the case of d -subshell,l = 2 and m – -2, -1, 0, +1 and +2. So there are five d -orbitals with equivalent energies.

Overlapping of atomic orbitals (AO): Formation of the covalent bonds
During the formation of a covalent bond, the combining atoms approach each other till they acquire minimum energy. At this stage, the half-filled atomic orbitals are so close to each other that they undergo partial interpenetration or partial merging. Such partial merging of atomic orbitals is called orbital overlap.
- This overlapping results in the pairing of electrons (with opposite spins) and causes a lowering of the energy of the system. The probability of finding electrons in the region of overlap is higher than in other places.
- The overlapping of half-filled atomic orbitals (containing electrons with opposite spins) leads to the formation of a covalent bond. The extent of overlap determines the strength of a covalent bond. The greater the extent of overlapping, the stronger the covalent bond.
- It is to be noted that the overlap between the atomic orbitals may be positive or negative depending on the nature of the overlapping of atomic orbitals. A positive overlap that leads to constructive interactions involves the overlap of the lobes of the same signs.
- A negative overlap which leads to destructive interactions, involves the overlap ofthe lobes of opposite signs. As the atomic orbitals (filled, partly filled, or vacant) have certain orientations, the covalent bonds also have specific orientations in three-dimensional space.
- When the electrons present in these orbitals form covalent bonds by pairing, then the covalent bonds formed have three-dimensional orientations. Hence due to the directional property of orbitals, covalent bonds too exhibit directional properties.
- Coordinate bonds also exhibit directional properties because coordinate bonds form due to the overlapping of filled orbitals of the electron donor atom with the empty orbital of the electron acceptor atom. The shape and orientation of the combining orbitals determine the shape of the compound formed.
Depending on the nature of overlapping, covalent bonds may be classified into two types:
- Sigma (σ) and
- pi (π) bond.
Sigma (r) bond: When a bond is formed between two atoms by the end-to-end (head-on) overlap of their atomic orbitals along the internuclear axis, i.e., the line joining the centers of the nuclei of the two atoms, it is called a sigma (σ) bond and the electrons constituting it are called sigma electrons.
Axial overlapping between two pure atomic orbitals:
s-s overlapping:
- This involves an overlap between the orbitals of the two approaching atoms. It is to be noted that s -orbitals are spherically symmetrical and can overlap to the same extent in all directions, along any axis.
- Since s orbitals are non-directional, the bond formed by the overlapping of s -s-orbitals is also non-directional.
For example, in the formation of an H2 molecule, the Is -orbital of one H-atom overlaps with the Is -orbital of another H-atom, forming a cr -bond.

s-p overlapping:
- This involves overlapping of s -the orbital of one atom with p -the orbital of another atom along their axes.
- The bond thus formed is called an (s-p) σ – bond. Since p -orbitals possess directional characteristics, the σ -bond formed by the overlap of s and p -orbitals, will also possess directional characteristics, which is similar to that of die p -orbital.
For example, in the formation of an HF molecule, the Is -orbital of one H-atom overlaps with the 2pzorbital of one F-atom thus forming a <x -bond. Thus, the z-axis is taken as the internuclear axis.

p-p overlapping:
- This involves the overlapping of p -p-orbitals of two approaching atoms along the internuclear axis.
- The bond thus formed is called a (p-p) σ -bond.
For example, the molecule of fluorine is formed by the overlapping of two 2pz -orbitals of two F -atoms.

Formation of σ-bond due to axial overlapping between a pure and a hybrid orbital (Sp3-s overlapping):
σ bond can be formed by the overlapping of pure s -orbital and a hybrid Sp3 -orbital 4 along their axes.
For example: the C—H <T -bond in CH4 is formed by the overlap between the Sp3 -orbital of the C-atom and the pure Is -orbital of the H-atom.

Formation of σ -bond due to axial overlapping between two hybrid orbitals (Sp3-Sp3 overlapping):
σ-bond can also be formed by the overlapping of two hybrid orbitals along their axes.
For example, the C—C σ -bond in ethane molecule is formed by the overlapping of two Sp3 -hybrid orbitals of two C-atoms.
Pi(π)bond:
- When a bond is formed by the lateral or sidewise overlap of two p -p-orbitals, it is called a pi (π) bond.
- The overlapping of orbitals occurs in such a way that their axes are parallel to each other and perpendicular to the internuclear axis.
- The resulting orbital is called a π-orbital and the electrons constituting it are called π-electrons.
Chemical Bonding And Molecular Structure Notes
- For example, in a C2H4 molecule, a sideways overlap of two parallel 2px -orbitals of two C-atoms occurs to form a n bond.
- A π-bond consists of two saucer-type charge clouds above and below the plane of the participating atoms.

- It is to be noted that a π-bond can be formed only in addition to a sigma bond, i.e., it is always present in the molecules having multiple bonds (double or triple).
- The spherically symmetrical s -s-atomic orbitals do not take part in sideways overlap to form a π-bond.
Strength of sigma and pi bond
- The strength of a covalent bond depends on the extent of overlapping between die-combining orbitals. The greater the overlapping, the greater the energy released and the stronger the bond.
- Axial overlapping of atomic orbitals leads to the formation of a σ-bond and sideways overlapping of orbitals leads to the formation of a σ-bond. Since the extent of axial overlapping is greater as compared to sideways overlapping, a π-bond is stronger than an n-bond.
- The π-bonds obtained by s-s, s-p, or p-p overlapping are not equal strengths.
- Two s -s-orbitals cannot overlap effectively with their spherical charge.
- On the other hand, the charge cloud of the σ-orbitals is concentrated along either the x, y, or z-axis.
- Their projected lobes can overlap effectively with s -s-orbitals and more effectively with other p -orbitals.
- Consequently, a p-p σ -bond is stronger than an s-p σ-bond which in turn is stronger than an s-s bond, i.e.,
- The order of decreasing bond strength is p-p > s-p > s-s.

Hybridization
According to the valence bond theory, a covalent bond is formed by the mutual overlap of two pure atomic orbitals. The formation of molecules like H2, Cl2, HCl, etc., can be easily, explained with the help of valence bond theory but, it fails to explain the formation of molecules like H2O, CH4, NH3, etc.
For example:
The H—O—H bond angle in a water molecule should be 90° as it involves the overlapping of pure 2p orbitals of O-atom but, the actual bond angle is 104.5°. Similar observations are found to occur in the case of NH3 molecules.
- To explain these experimental observations, a new concept called hybridization was introduced by L. Pauling.
- According to this concept, the atomic orbitals possessing slightly different energies mix up to form a new set of orbitals each having an equivalent amount of energy.
- These orbitals are called hybrid orbitals and the mixing is called hybridisation.
Hybridization Definition:
Hybridization may be defined as the intermixing of atomic orbitals of the same atom having the same or slightly different energies to redistribute their energies and form new orbitals of equal energies and identical shapes.
Salient features of hybridization:
- The number of hybrid orbitals formed is equal to the number of atomic orbitals taking part in hybridization.
- The energy and shapes of the hybrid orbitals are always equivalent.
- Hybrid orbitals are more effective in forming stable bonds as compared to pure atomic orbitals. This is because they can undergo more effective overlapping.
- The hybrid orbitals are oriented space in some preferred directions to have a stable arrangement with minimum repulsions among themselves. So, types of hybridization govern the geometrical shapes ofthe molecule.
Important conditions for hybridization:
- Only the orbitals present in the valence shell of the atom are involved in hybridization.
- The orbitals participating in hybridization should have comparable energies.
- Promotion of electrons is not an essential condition for hybridization.
- Not all the half-filled orbitals need to participate in hybridization.
- Only the half-filled orbitals don’t need to participate in hybridization. Filled orbitals of the valence shell can also participate in hybridization.
- Hybridization never takes place in isolated atoms. It occurs only when the atom takes part in bond formation.
Explanation of the tetravalency of carbon atoms:
- The electronic configuration of the carbon atom in its ground state is \(1 s^2 2 s^2 2 p_x^1 2 p_y^1 2 p_z^0\), i.e., one odd electron is present in each of 2px and 2py orbitals of carbon atom. Number of odd electrons present in the valence shell of odd electrons present in the valence shell of odd electrons present in the valence shell of an atom generally gives the measure of the covalency of that atom.
- So, the valency of carbon should be two. However, the valency of carbon in almost all organic compounds is 4, except for a few extremely unstable compounds, where the valency of C is 2, like methylene (: CH2), dichloromethylene (: CCl2), etc.
- During a chemical reaction, the 2 electrons in 2s-orbital become unpaired by absorbing energy, and one electron is promoted to 2pz -orbital. This is an excited state of a carbon atom and the electronic configuration of the carbon atom in this state is,\(1 s^2 2 s^1 2 p_x^1 2 p_y^1 2 p_z^1\). Thus in the excited state, 4 odd electrons are present in the outermost shell of a carbon atom. The presence of these four unpaired electrons accounts for the tetravalency of carbon atoms.

Sp3-hybridisation
When one s and three p -orbitals ofthe valence shell of an atom merge to form four new equivalent orbitals having the same energy and shape, it results in tetrahedral or Sp3-hybridization. The resulting orbitals are called Sp3 – hybrid orbitals.
Sp3-hybridisation Process

The four Sp3-hybrid orbitals each containing one electron, are directed towards the four comers of a regular tetrahedron making an angle of 109°28′ with one another and the atom lies generally given at the center of the tetrahedron.
Orbitals are oriented in such positions in space that minimum repulsions occur between them. The formation of Sp3-hybrid orbitals by the combination of s, px, py, and pz-atomic orbitals in

Sp3 -hybridization can be illustrated by the following examples:
Formation of methane (CH4) molecule:
- During the formation of a methane molecule, one 2s -orbital and three 2porbitals of excited carbon atom undergo hybridization to form four equivalent Sp3 -hybrid orbitals.
- The hybrid orbitals are directed toward the four comers of a regular tetrahedron with the C-atom at the center of the tetrahedron.
- Each hybrid orbital containing an unpaired electron overlaps with the Is -orbital of a hydrogen atom resulting in the formation of a total of four C —H bonds.
- Thus, the methane molecule has a highly stable tetrahedral geometry with each H —C —H bond angle equal to 109°28′.

Note that if the four atoms linked covalently to a carbon atom are not the same the geometry of the molecule wooly still be tetrahedral but it may not be regular in shape, Example methyl chloride (CH3Cl), chloroform (CHCI3), etc.

In these discs, the bond angles differ slightly from the normal value of 109°28′. Formation of ethane (CH6) molecule:
During the formation of the ethane molecule, each of the two C -atoms in their excited states undergo Sp3 -hybridization. Two hybrid orbitals, one from each C -atom, overlap axially to form a C — C σ -bond.
The remaining three hybrid orbitals of each carbon atom overlap with the half-filled Is -orbital of hydrogen atoms forming a total of six C — H σ-bonds, Each C —H bond in ethane is (Sp3-s) σ-bond having a bond length of 109 pm. The C —C bond is an (Sp3-Sp3) σ -bond having a bond length of 154 pm.
sp2-hybridisation
When one s -orbital and two p -orbitals of the valence shell of an atom merge and redistribute their energies to form three equivalent new orbitals of equal energy and identical shape, the type of hybridization involved is called sp² -hybridization. The new orbitals thus formed are called sp² -hybrid orbitals.

All three hybrid orbitals each containing one electron lie in one plane making an angle of 120° are directed towards three corners of an equilateral triangle with the carbon atom in the center of the triangle. The unhybridized 2pz -orbital (containing one electron) remains perpendicular to the plane of the triangle with its two lobes above and below that plane.

Therefore, a molecule in which the central atom is sp² -sp²-hybridized has a triangular planar shape and the hybridization is called planar trigonal hybridization. Formation of sp² -hybrid orbitals by the combination of s, px, and py -atomic orbitals.
sp² -hybridization can be illustrated by the following examples:
Formation of ethylene C2H4 molecule: in the formation of the ethylene molecule, each ofthe two carbon atoms undergo sp² -hybridization, leaving the 2pz -orbital unhybridised. The three sp²-hybrid orbitals of each carbon atom are planar and oriented at an angle of 120° to each other.

- The unhybridized 2pz -orbital is perpendicular to the plane of sp² -hybrid orbitals. One sp² -hybrid orbital of one carbon atom overlaps axially with one sp² -hybrid orbital of the other carbon atom to form a C — C cr bond.
- The remaining two sp” -hybrid orbitals of each carbon atom overlap with the half-filled Is -orbitals of two hydrogen atoms resulting in the formation ofa total of four C —H σ -bonds. The unhybridized 2pz -orbital of one carbon atom overlaps with that of the other carbon atom in a sideways fashion to form an n-bond between the two carbon atoms.
Chemical Bonding Class 11 Chemistry
- The n-bond consists of two equal electron clouds distributed above and below the plane of carbon and hydrogen atoms. All the six atoms in the molecule lie in one plane. Thus, ethylene is a planar molecule.
- In this molecule, the C=C bond (one sp²-sp² σ -bond and one 7σ-bond) length is 134 pm, the C —H bond (sp²-s bond) length is 108 pm and each C—C—H or H —C —H bond angle is nearly equal to 120°.
Formation of boron trifluoride (BF3) molecule:
The excited state electronic configuration of boron is \(1 s^2 2 s^1 2 p_x^1 2 p_y^1\). One 2s -and two 2p -orbitals of boron undergo hybridization to form three equivalent sp² -hybrid orbitals (each containing one electron). The sp² -hybrid orbitals are directed towards the comers of an equilateral triangle and lie in one plane making an angle of 120° with one another.
Each of the sp² -hybrid orbitals overlaps axially with the half-filled 2p -orbital of fluorine to form three B —F σ- bonds. Due to the sp²-hybridization of boron, the boron trifluoride molecule has a trigonal planar shape. The formation of boron trifluoride (BF3) molecule.

sp- hybridization
When one s and one p -orbital of the valence shell of an atom merge and redistribute their energies to form two equivalent hybrid orbitals of equal energy and identical shape, tin; hybridization Involved is called ip-hybridization or diagonal hybridization, The orbitals lints obtained are called sp-hybrid orbitals.

The other two p -orbitals remain unhybridized. These sp hybrid orbitals are Inclined to each other at an angle of 180°. Therefore, a molecule in which the central atom is sphybridised is linear in shape and the hybridisation is also known as diagonal hybridisation. The formation of sp-hybrid orbitals by the combination of 2s and 2px -atomic orbitals.

Sp-hybridization can be illustrated by the following examples:
Formation molecules of bothacety lengthy C-atoms(HCsHC)are sp molecule:
Hybridized in Thereacetylene two Orbital overlap in BeF2 unhybridized orbitals (2py & 2pz) on each C-atom.
- Two sp-hybrid orbitals are linear and are directed at an angle of 180°, Urihybridised p -orbitals are perpendicular to the sp-hybrid orbitals and also perpendicular to each other. One sp -sp-hybridized orbital of one C-atom overlaps axially with a similar orbital of the other C-atom to form a C σ -bond.
- The remaining hybrid orbital of each C-atom overlaps with the half-filled s -s-orbital of the H-atom to form a total of two C—H σ -bonds. Thus, the acetylene molecule is linear, (fn hybridized py -orbitals of two carbons and the unhybridized pz -orbitals of two carbons overlap sideways separately to form two different n -bonds.
- Electron clouds of one n-bond lie above and below the internuclear axis representing the σ-bond whereas the electron cloud of the other π -bond liein the front and back of the internuclear axis. These two sets of n -n-electron clouds merge into one another to form a cylindrical electron cloud around the internuclear axis surrounding the C —C σ -bond.
- In the acetylene molecule, the C-C bond length is equal to 120 pm, the C—H bond length is equal to 108 pm and the C —C —H bond angle is equal to 180°.

Formation of beryllium fluoride (BeF2) molecule:
- The excited state electronic configuration of Be is \(1 s^2 2 s^1 2 p_x^1\). The 2s -orbital and the 2px -orbital containing one electron each undergoes hybridization to form two sp -hybridized orbitals.
- The two sp-hybrid orbitals are linear and oriented in opposite directions at an angle of 180°
- . These two hybrid orbitals overlap axially with the half-filled 2p orbitals of the two fluorine atoms to form two Be—F σ bonds.
- Thus, the BeF2 molecule is linear The formation of beryllium fluoride molecule.

Hybridizations involving s, p, and d-orbitals
Sp3 d-hybridization:
This type of hybridization involves the mixing of one s, three p, and one d -orbitals to form five equivalent Sp3d-hybrid orbitals. These hybrid orbitals are directed towards the five corners of a trigonal bipyramid and hence such hybridization is called trigonal bipyramidal hybridization.

Example: In PC15 molecule, P-atom using one 3s, three 3p, and one 3d -orbitals form five Sp3 d -hybrid orbitals which are directed towards the five comers of a trigonal bipyramid.

The five Sp3d -hybrid orbitals overlap axially with five half-filled 3p -orbital of five Clatoms to form five P bonds. Thus, PCl5 has a trigonal 120° bipyramidal shape. Each axial (a) P —Cl bond is involved in repulsive Interaction with the equatorial (e) P—Cl bond pair, whereas each equatorial P—Cl bond is Involved in repulsive interaction with two equatorial P—Cl bond pairs.

As a result of this, the length of the P—F axial bond somewhat increases compared to that of the P —F equatorial bond (P—F axial = 158 pm, P—F equatorial = 153 pm).
Sp3d2 -hybridization:
In this type of hybridization, one s, three p, and two d -orbitals (dx²-y² and dz²) intermix to form six equivalent Sp3d2 -hybrid orbitals. The molecules, in which these orbitals of the central atom are involved have octahedral geometry.

Example:
In the SF6 molecule, she orbitals (one s, three p, and two d -orbitals) of S-atom hybridize to form six new Sp3d2 – hybrid orbitals which are projected towards the six comers of a regular octahedron.

These six equivalent hybrid orbitals overlap with the 2porbitals of six fluorine atoms to form six S—F σ-bonds. SF7 molecule has a regular octahedral geometry. Since each S—P bond Is involved in similar repulsive interaction with five orthogonal S— F bond pairs, all the six S —F bonds are equal In length.
Molecular Structure Class 11 Notes
5p3d3-hybridization:
This type of hybridization Involves the intermixing of one s, three p, and three d -( dxy,dyz, da.) orbitals to form seven Sp3d2 -hybrid orbitals that adopt pentagonal bipyramidal geometry.

Example: In IF7 one 5s, three 5p, and three 5d -orbitals of Iatom hybridize to give seven Sp3d2 -hybrid orbitals.

These seven hybrid orbitals overlap axially with the half-filled 2p -orbitals of the atom forming seven I— F or bonds one to Sp3d2 -hybridization of the central molecule lists pentagonal bipyramidal geometry.
Five I—F bonds are directed towards 1 the vertices of a regular pentagon making an angle of 72° with each other. The remaining two I—F bonds are directed at an angle of 90- above and below the plane of the pentagon.
- Orbitals of an atom with the same energy level take part in hybridization.
- Before hybridization, the transfer of electrons is not mandatory.
- No. of hybrid orbitals is equal to no. of participating orbitals.
- Not only half-filled orbitals but also filled orbitals can take part in hybridization.
- Hybridization does not occur in discrete atoms.
- Hybridization occurs due to the formation of bonds.
- An idea about the geometrical shape of a molecule can be obtained from the nature of hybridization.
- Hybrid orbitals form more stable bonds than pure atomic orbitals.
- d -orbitals involved in various types of hybridization
- ⇒ \(\begin{aligned}
& s p^3 d: d_{z^2} ; s p^3 d^2: d_{x^2-y^2}, d_{z^2} ; s p^3 d^3: d_{x y}, d_{y z}, d_{z x} \\
& d s p^2: d_{x^2-y^2}
\end{aligned}\)
Determination of hybridization of the central atom
From the following general formula, the number of orbitals of the central atom of a molecule or ion undergoing hybridization (H) can be determined and hence the state of hybridization of that atom can be known.
From the knowledge of the type of hybridization of the central atom, the shape ofthe molecule orion may be ascertained.
⇒ \(H=\frac{1}{2}[V+X-C+A]\)
Where,
H = Number of orbitals involved in hybridization
V = Number of electrons in the valence shell of the central atom,
X = Number of monovalent atoms surrounding the central atom,
C = Charge on the cation, and A = Charge on the anion.

State of hybridization of the central atom of different molecules or Ions


Resonance
Sometimes, all the properties of some molecules or ions, cannot be predicted from a single electronic (Lewis) structure. In such cases, the molecule or ion is represented by two or more Lewis structures which differ in the arrangement of valence electrons keeping the basic structure involving the sigma skeleton the same.
Resonance Definition:
The Various Lewis Structure, That Differ In the Positions Of Non-bonding or Electrons But not in the relative position of the atoms are known as resonance structures or canonical forms, and the concept is called resonance. Resonance structures are imaginary and are considered to explain the physical and chemical properties of the molecules or ions.
The actual molecule or ion is a resonance hybrid of all the canonical forms that are involved in resonance. Resonance is also known as mesomerism. Various resonance structures are connected by double-headed arrows \((\longleftrightarrow)\).
Rules for writing meaningful resonance structures
The rules for writing meaningful resonance structures are:
- The various resonance structures should differ only in the position of electrons. The basic structure involving bonds between atoms should remain undisturbed.
- The number of unpaired electrons, if any, in the resonance structures must be the same.
- Only those atoms should be involved in the resonance which are coplanar (or nearly coplanar).
- The resonance structures should have nearly the same energy.
- Each structure must be a proper Lewis structure.
Examples: Carbonate ion \(\left(\mathrm{CO}_3^{2-}\right)\) is represented as a resonance hybrid of the following three resonance structures:1,2 and 3.
- In all three structures, there are two carbon-oxygen single bonds (1.43A) and one carbon-oxygen double bond (1.20Å). Experimental results have however revealed that all the carbon-oxygen bonds are of equal length (1.28Å) in carbonate ions.
- Thus, all the three carbon-oxygen bonds are equivalent. This shows that the actual structure of carbonate ion is intermediate between the structures 1, 2, and 3. So carbonate ion is often represented by the non-Lewis structure 4, which is also considered as the hybrid structure.

Nitrate ion (NO-3) is represented as a resonance hybrid ofthe following three equivalent resonating structures:

If we consider any one of the nitrogen-oxygen bonds, then we see that in one structure it is a double bond while in the other two structures is a single bond. So, every N-O bond is equivalent i.e., every N-O bond length is the same.
Resonance energy
Resonance energy Definition:
Resonance energy is defined as the difference in internal energy between the actual or observed value and that of the resonance structure with the lowest internal energy i.e., the structure with the highest stability.
Unit:
Resonance energy is expressed in terms of kcal-mol-1 or kj. mol¯1. With the increase in the value of resonance energy internal energy of the compound decreases and hence stability ofthe compound increases.
Calculation of resonance energy:
Resonance energy is not a measurable quantity. It can only be obtained from thermochemical data.
- Cyclohexene on hydrogenation forms cyclohexane. In this reaction, 28.6 kcal-mol-1 heat is generated. Thus, on hydrogenation of a double bond, 28.6 kcal-mol-1 of heat is obtained.
- Accordingly, on hydrogenation of three double bonds of 1,3,5-cyclohexatriene (benzene), 3 × 28.6= 85.8 kcal-mol-1 heat should be obtained.
- But, in reality, the heat of hydrogenation of benzene is 49.8 kcal-mol-1
- Thus, the internal energy of benzene is (85.8-49.8) = 36 kcal-mol-1 less than the predicted value. This 36 kcal-mol-1 is the resonance energy of benzene.
- The lowering of internal energy by 36 kcal-mol-1 is responsible for the extra stability of benzene.
Examples of resonance in some molecules or ions:


Electronegativity
Electronegativity Definition:
The electronegativity of an element is the tendency or ability of its atom to attract the bonding or shared pair of electrons towards itself in a covalent bond. It is represented by x.
Example:
In the HCl molecule, Cl is more electronegative than H. As a result, the Cl -atom draws the bonding electron pair towards itself. Thus Cl – atom acquires a partial negative charge and the H-atom acquires a partial positive charge 5+ <5- \([\stackrel{\delta}{\mathrm{H}}-\stackrel{\delta-}{\mathrm{C}}]\). So, the partial ionic character is developed in the covalent molecule HCl.
The Pauling scale of electronegativity
According to Pauling, the bond energy of any compound, A—B is greater than the geometrical jerage of the bond energies of its constituent molecules, A2 B2. i.e., \(E_{\mathrm{A}-\mathrm{B}}>\left(E_{\mathrm{A}-\mathrm{A}} \cdot E_{\mathrm{B}-\mathrm{B}}\right)^{1 / 2}\) terms indicate bond energy
The difference between \(E_{\mathrm{A}-\mathrm{B}}>\left(E_{\mathrm{A}-\mathrm{A}} \cdot E_{\mathrm{B}-\mathrm{B}}\right)^{1 / 2}\) is called the Ionic resonance energy of the A—B bond and it is expressed by AA _ \(E_{\mathrm{A}-\mathrm{B}}>\left(E_{\mathrm{A}-\mathrm{A}} \cdot E_{\mathrm{B}-\mathrm{B}}\right)^{1 / 2}\)
Here, EA_B bond energy includes both the ionic and covalent bond energies but, the source of both the bond energies, Δ A_A and EB_B is only the covalent bond. So, the value of AAB determines the extent of the ionic character of the A—B bond. In the opinion of Pauling, the value of AA B is related to the electronegativities of the two elements.
If XA and XB are the electronegativities of A and B respectively, then
⇒ \(\chi_{\mathrm{A}}-\chi_{\mathrm{B}} \propto\left(\Delta_{\mathrm{A}-\mathrm{B}}\right)^{1 / 2}\) or, \(\chi_{\mathrm{A}}-\chi_{\mathrm{B}}=K\left(\Delta_{\mathrm{A}-\mathrm{B}}\right)^{1 / 2}\) [where K constant]
If the die value of AA_B is expressed in the unit of k.J mol-1, then K = 0.208.
Thus, the equation reduces to
⇒ \(\chi_A-\chi_B=0.208 \times\left(\Delta_{A-B}\right)^{1 / 2}\)
As the values of EA_B, EA_ A, and EB_B can be determined by experiments, so for any compound, A—B, the value of AA_B can easily be estimated. Once the value of ΔA_B is determined, then from the knowledge of the electronegativity of either element A or B, the electronegativity of the other element can easily be calculated.
Based on this theory and calculations, Pauling determined the electronegativities of different elements (in normal oxidation state). The values of electronegativities of elements which are determined for electronegativity of 2 (2.1) is called the Pauling scale of electronegativity.

Mulliken’s scale of electronegativity
Mulliken regarded electronegativity as the average value of ionization potential (IE) and electron affinity (EA) of an atom of any element.
Therefore, Electronegativity (xA) = \(\frac{I E+E A}{2}\) [IE and EA are expressed in the union eV-atom-1]
Factors affecting the electronegativity of elements
Atomic size or radius:
If the atomic size or volume is small, the distance of the outermost shell from the nucleus becomes less. Consequently, the positive charge of the nucleus attracts the electron(s) to a greater extent. Hence, the smaller the die atomic size, the higher be electronegativity.
Example:
The electronegativity of elements belonging to group-1A of the periodic table gradually decreases from H to Cs.

Number of shells in an atom:
As the number of shells between the nucleus and the outermost shell increases, because of the shielding effect of the electrons In the inner shells, the electronegativity of elements decreases.
Example: Electronegativity of elements belonging to group A gradually decreases from F to I.

Atomic Electro negativity number or nuclear charge:
If the number of shells m remains the same, Then with an increase in atomic number (i.e., nuclear positive charge), electronegativity increases.
- Oxidation state: For an element that exhibits several oxidation states, electronegativity at a higher oxidation state is more than that in its lower oxidation state
- Example: Electronegativities of Fe, Fe2+, and Fe3+ are 1.8, 1.84, and 1.95 respectively. The electronegativity of sulfur in SFf) is higher than that in SCI2.
- Electron affinity: Generally, the higher the electron affinity of any element, the greater its electronegativity.
- Example: Halogens of the group- 7A are strong electronegative elements because of their very high electron affinity values. Alkali metals of group IA have low electron affinity. So, their electronegativity values are very small.
- Hybridization: Hybridisation of the atom of an element has a significant effect on the electronegativity of that atom. The greater the s -s-character of the hybrid orbital, the higher its electronegativity.
Example:

Nature of the substituents attached to the atom:
The electronegativity of an atom increases with an increase in the electronegativity ofthe atom bonded to it.
Example: C-atomic CF3I is more electronegative than CH3I.
Molecular Structure Class 11 Notes
Bond Polarity And Dipole Moment
Non-polar covalent bond :
- If two similar atoms (atoms having the same electronegativities) form a bond by sharing a pair of electrons, the shared electron parties just in the middle of the two nuclei.
- In other words, the electron cloud constituting the covalent bond is symmetrically distributed between the two bonded atoms.
- As a result, no poles are developed and in such a case, the covalent bond becomes almost pure. This type of covalent bond is called a non-polar covalent bond.
- The corresponding molecule is known as a non-polar covalent molecule.
Some examples of non-polar molecules are H2(H —H), C12(C1 —Cl), O2(0=0), N2(N = N) etc.
Polar covalent bond:
- When a covalent bond is formed between two atoms having different electronegativities, the shared pair of electrons gets displaced more towards the more electronegative atom. As a result, the more electronegative atom acquires a partial negative charge and the less electronegative atom acquires a partial positive charge.
- This type of bond is called polar covalent bond (i.e., covalent bond with partial ionic character), and the molecules having such bonds are called polar covalent molecules or simply polar molecules. HF, for example, is a polar molecule.
- The extent of the percentage of ionic character in a covalent bond depends on the difference in electronegativities of the two bonding atoms. The greater the difference in electronegativities, greater is the greater the percentage of ionic character in the bond (i.e., greater is the polarity of the bond).
For example, the order of polarity of bonds in halogen hydrides is:
H —F(60%) > H —Cl(19%) > H —Br(ll%) > H —1(4%). This is because the electronegativities of halogens decrease in the order F > Cl > Br >I.
If the difference of electronegativities between two combining atoms is 1.7, then the bond is said to possess 50% ionic character.
An approximate relation between the difference in electronegativities of the bonded atom and the resulting ionic character is given in the following table.

Dipole moment
The product of the magnitude of positive or negative charge (q) and the distance (d) between the centers of positive and negative charges in a polar molecule is called dipole moment.
Dipole moment is usually represented by the Greek letter, ‘μ’ (mu). It can be expressed mathematically as μ = q x d.
Unit: The CGS unit of dipole moment is D (Debye). ID = 10-18 esu. cm. The SI unit of dipole moment is Coulomb-metre (C-m) and 1 C.m = 2.9962 × 1029 D.
General characteristics: Some important characteristics of dipole moment are mentioned below—
- The value of μ for a non-polar molecule is zero. For example, in the case of H2, O2, and N2 molecules, μ= 0 D . For polar molecules,μ has a definite value, Example for HF molecule, μ = 1.91 D. Polarities of molecules increase with an increase in the value of
- Since dipole moment is a vector quantity, it has magnitude as well as direction. Its direction is usually indicated by a crossed arrow \((\longmapsto)\) pointing from the positive to negative pole in a polar bond or polar molecule as a whole.
- Molecules formed by two different elements (A —B) are always polar i.e., they possess dipole moment. Due to the differences in electronegativities of the two atoms, the bond between them is polar. For example HC1 is a polar molecule \(\mathrm{H} \mathrm{Cl}\) (μ= 1.03D).
Polyatomic molecules may be non-polar although they possess polar bonds:
The dipole moment of a polyatomic lu molecule depends <not only on the polarity of the bonds present in it but also on the spatial arrangement of various bonds on the geometrical shape of the molecule because in such cases, the dipole moment of a molecule is considered to be the vector sum of the dipole moments of various bonds
Examples:
- If a triatomic molecule of the type, AB2 is linear (B—A—B) shaped, two equal but opposite \(A B\)(B Is more electronegative than A) bond moments cancel out each other, and hence, resultant dipole moment becomes zero. For example, C02, CS2, BeCl2, etc., have no net dipole moment.
- On the other hand, if the molecule is angular, two A \(A B\)(B is more electronegative than A or A \(A B\) (A is more electronegative than B) bond moments will not cancel out each other.
- So, there will be a resultant dipole moment \(A B\) and the molecule will be polar. For example, H2O, H2S, etc. possess a net dipole moment In fact, symmetrical molecules have no resultant dipole moment although their bonds are polar.
Applications of dipole moment
- To distinguish between polar and non-polar molecules: Molecules having specific dipole moment are polar while those having zero dipole moment are polar. Thus, BeCl2 (y = 0D) is a non-polar molecule while H2O (y = 1.85D) is a polar one.
- Comparison of relative polarities of molecules: The relative polarities of molecules can be compared from their dipole moment values because the greater the magnitude of the dipole moment, the higher the polarity of the molecule. Thus, H2O (1.85D) is more polar than H2S (1.10D).
- Determination of shapes of molecules: The dipole values help predict the general shapes of molecules containing three or more atoms. If a molecule is symmetrical, its dipole moment is found to be zero.
Example:
Molecules like CO2, CCl4, BF3, etc., have no net dipole moment. Therefore, these molecules have a perfectly symmetrical shape (CO2 is linear, CCl4 is tetrahedral and BF3 is triangular planar).

Percentage of ionic character of a bond:
From the knowledge of dipole moment and bond length, it is possible to determine the percentage of ionic character of a covalent bond.
Example:
The extent of the ionic character of the H—Cl bond in a hydrogen chloride molecule can be estimated from the value of its dipole moment (1.03D) and bond length (1.275Å). For 100% ionic character, the charge developed on H and Cl-atoms would be equal to the charge of an electron (4.8 × 10-10 esu). Therefore, the dipole moment of HCl when its bond is 100% ionic would be,
⇒ \(\mu_{\text {ionic }}=q \times d=4.8 \times 10^{-10} \mathrm{esu} \times 1.275 \times 10^{-8} \mathrm{~cm}\)
= \(6.12 \times 10^{-18} \mathrm{esu} \cdot \mathrm{cm}=6.12 \mathrm{D}\)
∴ Percentageionic character
= \(\frac{\mu_{\text {observed }}}{\mu_{\text {ionic }}} \times 100\)
\(\frac{1.03}{6.12} \times 100=16.83\)The distinction between stereoisomers (cis-and trans-isomers):
In a disubstituted ethene, the os-isomer usually has a higher dipole moment than the fracas-isomer. This is because, in the cis-isomer, the bond moments are not canceled out while in the trans-isomer, the bond moments are either totally or partially canceled out.
Example:
The cis-isomer of 1,2-dichloroethene has a definite dipole moment whereas the dipole moment of the transisomeris found to be zero.
The distinction between structural isomers (ortho, meta, and poro-isomers):
- The dipole moment of para-disubstituted benzene (with identical and symmetrical substituents) is zero and that of the ortho-isomer is greater than that of the mete-isomer (for electron-withdrawing substituents).
- From this knowledge, it is possible to distinguish between any two of these isomers or to identify all three isomers.
Prediction of relative boiling points of compounds:
If the value of the dipole moment is much higher, then the compound is highly polar indicating that, the dipole-dipole attractive forces among the molecules are sufficiently strong. Hence, a large amount of energy is required to separate the molecules from each other, i.e., the boiling point of such a compound is much higher.
Dipole moments (µ) of some molecules

Group moment:
The resultant moment of a group obtained as the vector sum of all the individual bond dipoles or bond moments present in it is called the group moment of that group. Benzene, for example, has no net dipole moment because oppositely oriented C —H bond moments cancel out each other.
When a -NO2 (nitro) group is substituted in place of any H-atom, the value of the dipole moment of nitrobenzene is found to be 3.95D. Therefore, it may be concluded that the group moment of the -NO2 group when attached to a benzene ring is 3.95D.

Prediction of dipole moments of some molecules from their geometrical shapes
Carbon dioxide (CO2) molecule:
In a CO2 molecule, the central carbon atom is sp -hybridized so CO2 is a linear molecule. For this type of structure, the two oppositely oriented C=O bond moments cancel out each other.
Because of this, CO2 is a non-polar molecule, i.e., it has no net dipole moment. Viewing alternatively, the center of positive charge and the center of negative charge coincide in this linear molecule; i.e., d = 0 and so, p =qxd = qxO =OD.
Beryllium hydride (8eH2) molecule:
The structure of the BeH2 molecule is similar to that of CO2 and hence, the linear BeH2 molecule is non-polar (µ = 0).
Carbon tetrachloride (CCI4) molecule:
c-atom in CCl4 molecule is sp³ -hybridized. So, it has a symmetrical tetrahedral structure. In such a geometrical shape, the resultant of the three C—Cl bond moments cancels the fourth C—Cl bond moment or the resultant of two C —Cl bond moments cancels the resultant of the other two C —Cl bond moments. Because of this, the dipole moment of the CCl4 molecule becomes zero, i.e., it is non-polar. Alternatively, the center of the positive charge and the center of the negative charge coincide in this tetrahedral molecule, i.e., d = 0 and = qxd = qxO = OD.
Boron trifluoride (BF3) molecule:
Since the B-atom in the BF3 molecule is sp² – hybridized, its geometrical shape is trigonal planar and the bond angles are 120°. Because of such a geometrical shape, the resultant of any two B —F bond moments cancels the third B —F bond moment. Hence, BF3 has no net dipole moment, i.e., it is non-polar.
Alternatively, the center of positive charge and center of negative charge coincide in this trigonal planar molecule, i.e., d = 0 and = qxd = qx0 = 0D.

Benzene (C6H6) molecule:
Due to the sp²-hybridization of the atoms involved, the benzene molecule is planar and all bond angles are 120°. Hence the shape of the molecule is hexagonal planar. In such a geometrical shape, each C —H bond moment is canceled out by another C —H bond moment lying opposite to it.
Hence, the molecule has no net dipole moment, i.e., it is non-polar. Alternatively, the centers of positive and negative charges coincide, i.e., d = 0 and µ= qxd=qx0 = 0D.
Chloroform (CHCl3) molecule:
Chloroform is a tetrahedral molecule because the central carbon atom is sp3 -sp3-hybridized. Because of such a geometrical shape, the resultant of the three C —Cl bond moments and the moment of the C —H bond (although very small) act in the same direction. Hence, the molecule possesses a net dipole moment, i.e., the molecule is polar.
Water (H2O) molecule:
The O-atom in H2O is sp³- hybridized. So, in this molecule, the two unshared electron pairs and the two 0 —H bonds are arranged tetrahedrally, and the actual shape of the molecule is angular. The h—O—H bond angle is 104.5°.
Because of such a geometrical shape, the resultant of two O —H bond moments and the resultant moment of the two unshared electron pairs act in the same direction. Thus, a water molecule possesses considerable dipole moment, i.e. it is a polar molecule.

Sulfur dioxide (SO3) molecule:
- The central sulfur atom in the SO2 molecule is sp² -hybridized. So, the two S = O bonds and the lone electron pair, are oriented towards the comers of an equilateral triangle, i.e., they lie mutually at an angle of about 120° and the molecule is angular or V-shaped.
- Because of such a shape, the resultant moment of the two polar S=O bonds is partly canceled by the moment contributed by an unshared electron pair acting in opposite directions. Hence, the SO2 molecule has a net dipole moment.
Nitrous oxide (N2O) molecule:
- Although N2O is a linear molecule, it possesses polarity because its structure is unsymmetrical (O -atom exists at one end). The (N → O) bond moment and the moment due to the unshared electron pair act in the opposite directions and the latter moment partly neutralizes the former one.
- Thus, the molecule has a net dipole moment of very small value.
Nitrogen trifluoride (NF3) molecule:
- The central nitrogen atom of the NF3 molecule is sp³ – hybridized. Thus, the three N—F bonds and one lone pair are arranged tetrahedrally, and excluding the lone pair, the shape of the molecule is pyramidal.
- Because of such a geometrical shape and higher electronegativity of fluorine, the resultant of the three N—F bond moments and moments contributed by the lone pair of electrons act in opposite directions.
- Thus, the molecule possesses a small but net dipole moment, Le„ the molecule is slightly polar.
Ammonia (NH3 ) molecule:
The geometrical shape of the ammonia molecule is similar to that of the NF3 molecule. However, because of the higher electronegativity of nitrogen compared to that of hydrogen, the resultant of the three N—H bond moments and the moment contributed by the lone pair act in the same direction. Consequently, it possesses a net dipole moment much higher than NF3.

Carbon monoxide (CO) molecule:
⇒\(\text { In }: C=\ddot{O}:\)
The molecule, a <xmoment (due to electron withdrawal through cr-bond) acts from carbon to the more electronegative oxygen atom. Also, a very weak n -moment operates from carbon to oxygen atom. Although the octet of O-atom is completed in this molecule, the carbon atom has a sextet.
So, oxygen donates an unshared pair of electrons to carbon and helps it to complete its octet by forming a dative σ- bond with it. As a result, a much stronger -moment acts from oxygen to carbon atom and since this moment is almost canceled by σ-moment and the weak r -moment acting in the opposite direction, the molecule possesses a very small net dipole moment.
Isomeric 1,2-dichloroethenes:
- Cis-i,2-dichloroethene is more polar than its trans-isomer. In the cis-isomer, the two C —Cl bond moments make an angle of 60° with each other.
- Consequently, a resultant moment acts in the molecule, i.e., the molecule possesses a net dipole moment.
- Conversely, in the trans-isomer, the two C —Cl bond moments acting in opposite directions neutralize each other.
Because of this, the molecule possesses no net dipole moment, i.e., the isomeris non-polar.

Isomeric 1,2- dichlorobenzenes:
Dipole moments of isomeric dichlorobenzenes follow the order:
- Ortho-or 1,2- dichlorobenzene > meta -or 1,3-dichiorobenzene > paraor 1, 4-dichlorobenzene.
- In para-isomer, the two C—Cl bond moments acting in opposite directions neutralize each other So, the isomer possesses no net dipole moment, i.e., the isomer is non-polarIn ortho-and meta isomers, the C- Cl bond moments act at an angle of 60° and 120° respectively.
- Since the resultant moment increases with a decrease in bond angle, the dipole moment of the ortho-isomer is higher than that of the meta-isomer, i.e., ortho-isomerism is more polar than meta-isomer.

The dipole moment of disubstituted benzenes (C6H4XY) can be determined by the equation:
⇒ \(\mu=\sqrt{\mu_1^2+\mu_2^2+2 \mu_1 \mu_2 \cos \theta}\)
Where px and p2 are group moments of the group, X and Y respectively and 9 is the angle between two group moments. In ortho, meta, and para-isomers, the values of 0 are 60°, 120°, and 180 ° respectively.
If any of the two groups is an electron with-drawing one, its group moment is to be represented with a negative sign. For example, the dipole moment of me to-nitrotoluene can be calculated as follows:
⇒ \(\mu_{\text {toluene }}=0.4 \mathrm{D}\)
⇒ \(\mu_{\text {nitrobenzene }}=0.35 \mathrm{D}\)
∴ \(\mu_{\mathrm{CH}_3}=0.4 \mathrm{D}\)
∴ \(\mu_{\mathrm{NO}_2}=-3.95 \mathrm{D}\)
∴ \(\mu_{m-\mathrm{CH}_3 \mathrm{C}_6 \mathrm{H}_4 \mathrm{NO}_2}=\mu\)
⇒\(\sqrt{\mu_{\mathrm{CH}_3}^2+\mu_{\mathrm{NO}_2}^2+2 \mu_{\mathrm{CH}_3} \mu_{\mathrm{NO}_2} \cos 120^{\circ}}\)
= \(\sqrt{(0.4)^2+(-3.95)^2+2 \times 0.4 \times(-3.95) \times-\frac{1}{2}}=4.16 \mathrm{D}\)
Numerical Examples
Example 1. Calculate the percentage of ionic character of HF. Given that the dipole moment of HF is 1.91 D and its bond length is 0.92A.
Answer:
If HF is 100% ionic, each atom would carry a charge equal to one unit, i.e., 4.8 x 10-10 esu. As the bond length of HF is 0.92A, its dipole moment for 100% ionic character would be
⇒ \(\mu_{\text {ionic }}=q \times d=4.8 \times 10^{-10} \mathrm{esu} \times 0.92 \times 10^{-8} \mathrm{~cm}\)
= 4.416 x 10-18 esu.cm = 4.416D
[l0-18 esu cm = ID]
∴ % ionic character \(=\frac{\mu_{\text {observed }}}{\mu_{\text {ionic }}} \times 100=\frac{1.91 \times 100}{4.416}=43.25\)
Example 2. The percentage of ionic character of LiH is 76.81% and the bond length is 1.596A. What is the value of the dipole moment of a molecule? [ID = 3.335 X 10-30Cm]
Answer:
If the molecule is 100% ionic, then
⇒ \(\mu_{\text {ionic }}=q \times d=1.602 \times 10^{-19} \mathrm{C} \times 1.596 \times 10^{-10} \mathrm{~m}\)
= \(2.557 \times 10^{-29} \mathrm{C} \cdot \mathrm{m}\)
⇒ \(\% \text { ionic character }=\frac{\mu_{\text {observed }}}{\mu_{\text {ionic }}} \times 100\)
∴ \(\mu_{\text {observed }}=\frac{\% \text { ionic character } \times \mu_{\text {ionic }}}{100}\)
⇒ \(\frac{76.81 \times 2.557 \times 10^{-29}}{100}=1.96 \times 10^{-29} \mathrm{C} \cdot \mathrm{m}\)
⇒ \(\frac{1.96 \times 10^{-29}}{3.335 \times 10^{-30}} \mathrm{D}=5.87 \mathrm{D}\)
Question 3. Calculate the fractional charge on each atom of HBr. The dipole moment of HBr is 0.78D and its bond length is 1.41A. [Electronic charge, e = 4.8 X 10_1° esu, ID = 10_18esu.cm].
Answer:
Dipole moment, μ = q× d or,
Or, \(=\frac{\mu}{d}=\frac{0.78 \times 10^{-18} \mathrm{esu} \cdot \mathrm{cm}}{1.41 \times 10^{-8} \mathrm{~cm}}\)
=\(0.55 \times 10^{-10}\)
⇒ \(\text { Fraction of charge }(\delta)=\frac{\text { Charge present }(q)}{\text { Electronic charge }(e)}\)
= \(\frac{0.55 \times 10^{-10} \text { esu }}{4.8 \times 10^{-10} \text { esu }}\)
= 0.11
∴ The fractional charge on hydrogen \(\delta_{\mathrm{H}^{+}}=0.11\) and the fractional charge on bromine,δBr = -0.11
Example 4. The dipole moment of NaCl is 8.5 D. Interatomic distance between Na+ and Cl- is 2.36 A. Calculate the percentage ionic character of the NaCl molecule.
Answer:
If NaCl is 100% ionic then,
⇒ \(\mu_{\mathrm{Na}^{+} \mathrm{Cl}^{-}}=e \times d=4.8 \times 10^{-10} \mathrm{esu} \times 2.36\)
= \(4.8 \times 10^{-10} \mathrm{esu} \times 2.36 \times 10^{-8} \mathrm{~cm}=11.328 \mathrm{D}\)
∴ % ionic Charchter \(=\frac{\mu_{\text {observed }}}{\mu_{\text {ionic }}} \times 100=\frac{8.5 \times 100}{11.328}=75.035\)
Hydrogen Bond
When a hydrogen atom Is covalently bonded to a small and largely electronegative atom, X (F, 0 or N), the electro¬ negative atom pulls the shared pair of electrons towards itself, resulting in the development ofa partial negative charge on the electronegative atom and a partial positive charge on the hydrogen atom.
This partially positively charged hydrogen atom behaves like a bare proton as Its nucleus gets exposed due to the displacement of the solitary electron.
Such a hydrogen atom of one HX molecule attracts a partially negatively charged Xatom of an adjacent HX molecule or a molecule of HY (where Y is an atom of another highly electronegative element) and the molecules are held together by a strong electrostatic force of attraction. The electrostatic force of attraction that exists between the hydrogen atom and the highly electronegative atom is known as the hydrogen bond.

Hydrogen Bond Definition:
The electrostatic force of attraction existing between the H-atom covalently bonded to an electronegative atom (F, O, or N) in a molecule and the electronegative atom of another molecule (of a similar or different type) is known as a hydrogen bond, Generally, a hydrogen bond Is represented as X —H Y, in which the X—H bond is covalent and H-Y bond is the hydrogen bond. Here, Y is the hydrogen bond acceptor and X —H is the hydrogen bond donor. The hydrogen bond acceptor may or may not contain H-atom.
Conditions for hydrogen bond formation
- Hydrogen atoms should be bonded to a highly electronegative atom such as F, O, or N. The common examples are HP, H2O, and NH3.
- The size of the electronegative atom should be small. This Is because the smaller the size of the electronegative atom, the higher its charge density and hence greater the electrostatic attraction. Thus NIL, molecules are involved in hydrogen bonding but HC1 molecules are not, although both N and Cl have the same electronegativity.
- An electronegative atom that participates in H-bonding must have at least one unshared pair of electrons.
Only the firm of elements such as F, O, and N can form effective hydrogen bonds. Although the electronegativities of chlorine and nitrogen are the same (3,0), chlorine cannot form a stable hydrogen bond but nitrogen can do so.
The reason Is that the atomic size of the chlorine atom (atomic radius of Cl-atom – 0.99A) is greater than that of the nitrogen atom (atomic radius of N-atom = 0.70A ).
Exception:
Intramolecular H-bond is found in compounds like chloral hydrate and art to-chlorophenol and rmolecular H-bond is found in para-chlorophenol.
Characteristics of hydrogen bonding
- H-bond is much weaker than a covalent bond but stronger than van der Waals forces of attraction. The strength of the H-bond is only 12.6-41.8 kj.mol-1 while that of a covalent bond is ofthe order of 400 kj. mol-1 .
- The strength of the hydrogen bond depends on the electronegativity of the atom to which the H-atom is attached. The larger the electronegativity of the atom, the greater the strength of the H-bond. For example, electronegativities of F, O, and N decrease in the order: of F(4.0) >0(3.5)>N(3.0).
Consequently, the strength of the H-bond decreases in the order
F—H—F (41.8kj.mo-1 )> O—H—O (29.3 kj-mol-1 )>N—H-N (12.6kJ.mol-1 )
- The position of the H-bond depends on the orientation of the lone pair of the electronegative atom, i.e., like a covalent bond, the hydrogen bond also has a definite direction of bonding.
- Because of the smaller size of hydrogen atoms, the valence shell electrons of the two atoms linked by hydrogen bonds experience considerable repulsion. To minimize the repulsion, all three atoms lie in a straight line [X—H- -X (X = F, O, N) ].
- The magnitude of H-bonding depends on the physical state of the compound. It is maximum in the solid state and minimum in the gaseous state. Thus, hydrogen bonding strongly influences the structure and properties of compounds.
- A large number of molecules remain associated with hydrogen bonding.
Types of hydrogen bonding
Intermolecular hydrogen Bonding:
When 11-bonding occurs between different molecules of the same or different compounds, it Is called Intermolecular hydrogen bonding.
Examples Hydrogen fluoride( HF):
In an HF molecule, (lie highly electronegative fluorine atom acquires a partial negative charge and the hydrogen atom acquires a partial positive charge. The negatively charged P -atom of one IIP molecule attracts the positively charged hydrogen atom of the other molecule to form a strong hydrogen bond between them.
In this way, a large number of molecules gel associated through hydrogen bonding and exist in a giant molecule which can be represented as (HF)n. In the solid (crystalline) slate, hydrogen fluoride consists of long zig-zag chains of molecules associated together through hydrogen bonds. In liquid and gaseous state, the length of the chain somewhat shortens.

Water (H2O):
- A water molecule contains one highly electronegative oxygen atom bonded to two H -atoms. Thus, the oxygen atom becomes partially negatively charged and the two hydrogen atoms become partially positively charged.
- The negative end of one molecule attracts the positive end of the other to form a hydrogen bond. In this way, a large number of water molecules become associated through hydrogen bonding to form a macromolecule which can be represented as (H2O)n.

Ammonia (NH3):
In an ammonia molecule, a moderately electronegative nitrogen atom is bonded to three hydrogen atoms and as a consequence, the nitrogen atom acquires a partial negative charge and each hydrogen mam acquires a partial positive charge. For this reason, the molecules of ammonia remain associated through hydrogen bonding to form a polymeric species which may be represented as (NH3)n.

Acetic acid (CH3COOH):
In the gaseous state, two acetic acid molecules get associated through hydrogen bonding to form an eight-membered cyclic dimer. However, in a liquid state, a large number of molecules remain associated through hydrogen bonding to form a polymeric species [(CH3COOH)n].

Intramolecular hydrogen bonding:
When hydrogen bonding takes place within the same molecule, it is called intramolecular hydrogen bonding. This type of hydrogen bonding is also known as chelation as it results in the formation of a ring. It is found to occur frequently in organic compounds and is favored when a six or five-membered ring is formed.
Examples:
It is normally found in disubstituted benzene compounds in which the substituents are attached to adjacent carbon atoms, i.e., they are ortho to each other. For example, ortho-nitrophenol, ortho hydroxybenzaldehyde, salicylaldehyde, and ort/zo-chlorophenol possess intramolecular hydrogen bonding.

It is found in some aliphatic compounds in which the groups involved in hydrogen bonding are situated at adjacent carbon atoms. For example, chloral hydrate [CCl3CH(OH)2] and ethylene glycol (HOCH2CH2OH) possess intramolecular hydrogen bonding.

Effect of H-bond on different properties of compounds
- Intermolecular hydrogen bonding causing the association of molecules of any compound results in an increase in the effective molecular mass of that compound. Consequently, the properties such as physical state, melting and boiling points, latent heat of vaporization, viscosity, concentration, surface tension, etc., which depend on molecular mass, are found to increase.
- Again, as the number of molecules decreases due to hydrogen bonding, the values of colligative properties of compounds such as osmotic pressure, elevation of boiling point, depression of freezing point, etc. decrease.
- Also, solubilities and acidities of compounds are often markedly influenced by hydrogen bonding. It is to be noted that the effect of intramolecular hydrogen bonding on the physical properties of compounds is negligible.
Chemistry Chapter 4 Class 11 – Chemical Bonding
Question 1. Although oxygen and sulfur belong to the same group (VIA) of the periodic table, at ordinary temperature, the hydride of oxygen (HzO) is a liquid whereas the hydride of sulfur (H2S) is a gas.
Answer:
Since the electronegativity of oxygen is higher than that of sulfur, the O —H bond in water is more polar than the S —H bond in H2S. Also, the size of the O-atom is smaller than that of the sulfur atom. So, the molecules of water are associated through intermolecular hydrogen bonding. Hence, water exists in the liquid state but hydrogen sulfide exists in the gaseous state at ordinary temperature.
Question 2. Among the hydrides of halogens (P, C, Br, and I) belonging to group-VIIA of the periodic table, only HF is a liquid at 19.5°C, while each of IICl, IiBr, and HI exists as a gas at this temperature.
Answer:
Because of the highest electronegativity and smaller atomic size of fluorine, HF molecules remain extensively associated through strong JutermoleeuJar hydrogen bonding. So, a large amount of energy Is required to separate the molecules. Hence, HF exists in the liquid state at 19,5°0, On the other hand, Cl, fir, and 1 atom are larger and less electronegative compared to F-atom, So, the formation of intermolecular hydrogen bonding leading to the association of the molecules Is not possible in case of HCI, HUr, and HI, Thus, each of them exists In the gaseous state at this temperature.
Question 3. KHF2 exists But KHCI2 has no existence
Answer:
F-atom In HF can form strong hydrogen bonds due to higher electronegativity and smaller size of F-atom. However, Cl does not form a hydrogen bond due to its comparatively low electronegativity and larger atomic size. In an aqueous solution, HF ionizes partially giving only one H+ ion per molecule.
Consequently, HF behaves as a weak monobasic acid. \(\mathrm{H} \rightleftharpoons \mathrm{H}^{+}+\mathrm{F}^{-}\) The fluoride Ion thus produced forms hydrogen bond with undissociated HF molecule to form fluoride anion HF2-.
⇒ \(\mathrm{F}^{-}+\mathrm{HF} \rightleftharpoons\left(\mathrm{F} \cdots-\mathrm{H}-\mathrm{F}^{-} \text {or } \mathrm{HF}_2^{-}\right.\)
This explains the existence of the salt KHF2. As Cl-atom cannot form an H-bond, so anion like HCl2 is not formed. Hence the salt, KHCl2has no existence.
Question 4. Although the molecular mass of PH3(34) (the hydride of the second element of group 15) is twice that of NH3 (17) (the hydride of the first element of the same group), the boiling point of PIf3 (—87.4°C) is much less than that of NH3 (-33.4°C).
Answer:
The electronegativity of nitrogen (3.0) is higher than that of phosphorus (2.2) and the atomic size of N is smaller than that of P. So, the N— H bonds in NH3 are relatively more polar than the P —H bonds In PH3.
Hence, Nil, molecules remain associated through intermolecular hydrogen bonding, but no H-hond is formed among PH2 molecules. Therefore the boiling point of NH3 is much higher than that of PH3 even though the molecular mass of PH3 is twice that of NH3.
Question 5. The boiling point of ethyl alcohol (78.5°C) is much higher than that of isomeric dimethyl ether (-24.9°C).
Answer:
Due to the much higher electronegativity and smaller size of oxygen, the O—H bond in ethyl alcohol (C2H5OH) is much polar and so, its molecules remain Associated through Intermolecular hydrogen bonding. A greater amount of energy IN is required To separate the molecules Hence, ethyl alcohol volatile unit tin boiling point IN is relatively much higher.
On tin other hand, the O-uto in In dimethyl ether (CH2OCH3) IN not bonded to any hydrogen atom. TIUIH, there IN no Possibility of formation of hydrogen bond. Consequently, the ether CXINIH is a discrete molecule. So, It IN more volatile, and the UN boiling point IN much lower than that of ethyl alcohol.

Question 6. The boiling point of formic acid (100.5°C) is higher than that of ethyl alcohol (78.5°C) even though their molecular masses are the same (46)
Answer:
Explanation:
Both formic acid and ethyl alcohol contain polar O—H bonds and remain associated through hydrogen bonding. Since the polarity of the O —H bond present in the —COOH group of formic acid Is much higher than that of the O—H bond in ethyl alcohol, the strength of the hydrogen bond in formic acid is much stronger than in ethyl alcohol.
(In formic acid, the polar bond of the carboxyl group is involved in the formation of hydrogen bonds). In the vapor state, the formic acid molecules are also involved in forming an eight-membered ring of the diner by intermolecular H-bond.

Because of the stronger hydrogen bond, the boiling point of formic acid is higher than that of ethyl alcohol even though both compounds have the same molecular mass.

In formic acid, the strength of the H-bond increases enormously, due to resonance.
Question 7. n -propylamine (CH3CH2C1I2NH2) boils at a much higher temperature (49″C) than the isomeric trimethylamine (Me., N, 3°C).
Answer:
In n -n-propylamine, the electronegative N -atom is bonded to twoIl-atoms. So Its molecules get associated through Intermolcculur hydrogen bonding. Because of this, it boils at a much higher temperature than the Isomeric trimethylamine in which, the formation of hydrogen bonds is not possible since there is no hydrogen atom directly attached to the electronegative N -atom.
Question 8. The melting and boiling points of p -p-nitrophenol are much higher than those of o-nitrophenol.
Answer:
In o-nitrophenol, -OH and -NO2 groups are situated at the two adjacent carbon atoms so that they are involved in intramolecular hydrogen bonding. Thus, these molecules exist as discrete molecules and consequently, the compound possesses lower melting and boiling points. On the other hand, in p-nitrophenol, the -OH and -NO2 groups are situated far apart from each other so intramolecular H-bonding is not possible. The molecules remain associated through intermolecular H-bonding.
Hence, the melting and boiling points of p-nitrophenol are much higher than those of nitrophenol. Due to its low boiling point, o-nitrophenol is steam volatile whereas p-nitrophenol is not.

Intramolecular H-bonding in ortho-nitrophenol molecule

Intermolecular H-bonding in para-nitrophenol molecule For the same reason, the volatility of o -hydroxybenzoic acid is higher than that of its meta- and para-isomers.
Question 9. Ethyl alcohol (C2H5OH) dissolves in water in all proportions but dimethyl ether (CH3OCH3) is sparingly soluble in water.
Answer:
Bach ethyl alcohol molecule, containing a polar O—H bond, forms 2 hydrogen bonds with two water molecules. So it dissolves in water molecules in all proportions. On die other hand, each dimethyl ether molecule forms one H-bond with a single water molecule through its electronegative O-atom. Hence, dimethyl ether is sparingly soluble in water.

Question 10. Alcohols having lower molecular masses are soluble in water but those with higher molecular masses are insoluble in water.
Answer:
An alcohol molecule (R—OH) is made of a polar -OH group (the hydrophilic part) and a non-polar alkyl group, —R (the hydrophobic part).In lower alcohols (i.e., alcohols having lower molecular masses), the hydrophilic -OH group overcomes the effect of the hydrophobic hydrocarbon group ( —R). Thus, these alcohol molecules dissolve in water by forming an H-bond with water molecules
On the other hand, in higher alcohols (i.e., alcohols having higher molecular masses) the hydrophobic character of the hydrocarbon group predominates over the effect of the polar hydrophilic group. Because of this, the higher alcohols show a negligible tendency to form H-bonds with water molecules and consequently, they are insoluble in water.
Question 11. Ammonium chloride (NH4Cl ) is more soluble than sodium chloride (NaCl) in water.
Answer:
Na+ ion, obtained by dissociation of NaCl is Stabilized by solvation, involving ion-dipole interactions (water acts as a dipole). But NH4 ion, obtained by dissociation of NH4Cl, becomes more stabilized by solvation involving the formation of stronger intermolecular hydrogen bonds with H2O molecules. Thus, NH4Cl is more soluble than NaClin water.
Question 12. Despite being organic compounds, glucose (C6H12O2) and sugar (C12H2O2) are soluble in the polar solvent, water.
Answer:
In glucose and sugar molecules, there are six and eight —OH groups respectively. Due to the presence of a large number of — OH groups, the molecules of these compounds form extensive H-bonds with water molecules. This accounts for the high solubility of these two organic compounds in the polar solvent, water.
Question 13. Although boric acid [H3BOs or B(OH)3] contains 3 —OH groups, its solubility in water is very poor.
Answer:
Boric acid molecules form a cyclic two-dimensional network, leading to a giant molecule by forming much stronger intermolecular H-bonds. Boric acid molecules can’t form hydrogen bonds with water molecules by breaking these strong hydrogen bonds. Hence, the solubility of boric acid in water is very poor.

Question 14. Grillo-nitrophenol is less soluble in water than its meta- or para-isomer.
Answer:
In o-nitrophenol, -OH and -NO2 Groups are involved in intramolecular H-bonding. So, the molecules of o-nitrophenol cannot form H -bonds with water molecules. Hence, o-nitrophenol is less soluble in water. On the other hand, both m-andp-nitrophenol are incapable of forming intramolecular H-bonds, and their —OH and —NO2 groups are free to form H-bonds with water molecules. So, these are more water-soluble.
o-nitrophottol being loss soluble In water Is steam-volatile. On the other hand, being more soluble In the water is not steam-volatile. Steam distillation, therefore, is an easy method of separation of o-nitrophenol from the other two Isomers.
Question 15. Although H2 SO4 And H3 PO4 Have the Same Molecular mass H3PO4 HAs a Higher Boiling Point And viscosity.
Answer:
H3PO4 molecule contains three —OH groups whereas each H2SO4 molecule contains only two —OH groups. So the extent of association through Intennolecular hydrogen bonding in H3PO4 is greater than that in H2SO4. Because of this, the boiling point and viscosity of H3PO4 are higher than that of H2SO4, even though their molecular masses are the same.

Question 16. Glycerol (CH2OHCHOHCH2OH) is a highly viscous liquid whereas ethyl alcohol is not.
Answer:
Glycerol molecules with three —OH groups, remain extensively associated through intermolecular hydrogen bonding and exist as long chains with many interlocking cross-linkages. For this reason, glycerol is a highly viscous liquid.
On the other hand, ethyl alcohol molecule with a single —OH group, remains associated through intermolecular hydrogen bonding. Though it exists as an associated molecule it does not possess interlocking cross linkages like glycerol. Therefore, ethyl alcohol is not a viscous liquid.
Question 17. ortho-hydroxybenzoic acid Is more acidic than parahy droxybcnzolc acid.
Answer:
Be conjugate base of o-hydroxybenzoic acid gets additional stability through intramolecular hydrogen bonding because the —OH and groups are attached to two adjacent ring carbons. On the other hand, the conjugate base of p-hydroxybenzoic acid is not stabilized by intramolecular hydrogen bonding because the groups are far apart from each other. Because of greater stability ofthe conjugate base, o-hydroxybenzoic acid releases H+ ion more easily, i.e., it exhibits more acidic properties than its para-isomer.

Question 18. 2,6-dihydroxybenzoic acid is much more acidic (nearly 800 times) than benzoic acid.
Answer:
In The Conjugate Base Of 2,6 dihydroxybenzoic acid the -coo- group undergoes intramolecular hydrogen bonding six-membered rings. The acid, PhCOO-, on the other hand, is not stabilized by H-bonding. Hence, 2,6- dihydroxybenzoic acid is more acidic than benzoic acid.

Question 19. The volume of ice decreases on melting or the density of ice is less than that of water.
Answer:
In the crystal of ice, each oxygen atom is surrounded tetrahedrally by four H-atoms, two H-atoms by usual covalent bonds, and the other two by H-bonds. Because of such tetrahedral arrangement and cage-like structure, there remains enough space among the water molecules.
When the ice melts, these tetrahedral arrangements of water molecules are largely destroyed. Water molecules come closer to each other and the intermolecular space is reduced. So, the same number of water molecules are now present in a smaller volume. Hence, the density of ice is less than that of water.

Question 20. The density of water is maximum at 4°C and decreases with an increase in temperature.
Answer:
When water is heated, the breaking of the tetrahedral structure having an ordered arrangement of H-bonds continues up to 4°C and the contraction caused by the proximity of water molecules is greater than thermal expansion (molecular agitation due to vibrational and kinetic energy).
Consequently, the volume goes on decreasing up to 4°C. Normal expansion of volume on heating starts only after 4°C. Therefore, water has its highest density at 4°C and it decreases with an increase in temperature.
Question 21. On heating a crystal of blue vitriol or cupric sulfate pentahydrate (CuSO4.5H2O ), four molecules of water of crystallization are easily removed. However, the removal of the last molecule of the water of crystallization requires thermal energy.
Answer:
Explanation:
Among the five molecules of water crystalized in the structure of blue vitriol, four molecules are linked to the Cu2+ ion through coordinate covalent bonds, and the remaining one molecule of water is joined to the sulfate ion (SO2-4). Two out of four molecules of water are linked also through H-bonds with the fifth water molecule which is further hydrogen bonded with SO2-4 ion.

Dehydration of blue vitriol, i.e., removal of water of crystallization from blue vitriol occurs in three steps.

This is due to the presence of different types of bonds between CuSO4 and molecules of water of crystallization. Two water molecules are bonded to the Cu2+ ion by coordinate bonds. Thus they are loosely held and on heating, they are removed at a comparatively low temperature (30°C).
The other two water molecules are bonded to the Cu2+ ion by coordinate bonds as well as to the fifth water molecule by H -bonds. Hence, they are tightly held and are removed at a comparatively high temperature (100°C).
The fifth water molecule is bonded to the third and fourth water molecules as well as to the two O-atoms of the sulfate ion through H-bonds. Thus, it is more tightly held and its removal requires even more energy i.e., much higher temperature (250°C). This water molecule is called anion water.
Participation C—H band in hydrogen hand formation:
Since there is negligible difference in electronegativity between carbon and hydrogen, so H-atom of the C —H bond is not expected to participate in hydrogen bond formation. But if an atom of any strong electronegative atom or electron-attracting group is attached to a carbon atom, then in some cases C—2 bond does take part in the formation of hydrogen bond, Example molecules of acetonitrile (CH3CN) get associated through intramolecular hydrogen bond; chloroform (CHCl3) molecules form hydrogen bonds with the molecules of acetone (CH3COCH3).
Difference between Hydrogen bond and covalent bond:

Molecular Orbital Theory (MOT)
Although the concept of hybridization could explain the structure and shapes of most of the covalent compounds quite satisfactorily, some of the characteristics of molecules such as their relative bond strengths, paramagnetic and diamagnetic nature, etc., including the formation of odd electron molecules or ions could not be explained successfully by this concept.
To explain these, the molecular orbital theory was put forward by F. Hund and R.S. Mulliken in 1932. As this theory is based on the linear combination of atomic orbitals, it is also called LCAO-MO theory.
Salient features of molecular orbital theory:
When two atomic orbitals overlap, they lose their identity and form new orbitals called molecular orbitals.
- Molecular orbitals are formed only by those atomic orbitals which are of comparable energy and proper symmetry. One s -s-s-orbital, for example, can combine only with another s -s-orbital but not with any 2s-orbital.
- An electron in an atomic orbital is influenced by only one nucleus, but in a molecular orbital, it is under the influence of two or more nuclei depending on the number of atoms in the molecule. Therefore, an atomic orbital is monocentric while a molecular orbital is polycentric.
- The number of molecular orbitals formed is the same as the number of combining atomic orbitals. Half of the new molecular orbitals have lower energy and hence have greater stability than the participating atomic orbitals.
- These orbitals with lower energy are called bonding molecular orbitals. The other half of the new molecular orbitals having higher energy than the participating atomic orbitals are called antibonding molecular orbitals.
Thus two atomic orbitals combine to form two molecular orbitals one of which is a bonding and the other one antibonding. The shapes of the resultant molecular orbitals depend on the shapes of atomic orbitals undergoing combination.
- The molecular orbitals are filled with electrons according to the same rules as applied to the filling of atomic orbitals.
- The molecular orbitals are filled in the order of their increasing energies (Aubau principle).
- A molecular orbital can accommodate a maximum of two electrons having opposite spin (According to Pauli’s exclusion principle).
- The pairing of electrons in degenerate molecular orbitals (molecular orbitals of equal energy) does not take place until each of them is singly occupied (Hund’s rule).
Formation of molecular orbitals: Linear Combination of Atomic Orbitals (LCAO)
In wave mechanics, atomic orbitals are expressed by wave functions which represent the amplitude of the electron waves. These are obtained from the solution of the Schrodinger wave equation.
- A similar wave equation can be formed to describe the behavior of electrons in molecules. However, because of the complex nature of the equation, it is very difficult to determine wave functions of molecular orbitals by solving the equation.
- To obtain die wave functions of molecular orbitals, an approximate method, a linear combination of atomic orbitals (LCAO) method has been adopted.
- Let us apply this method to the homonuclear diatomic H2 molecule. Let us consider that the hydrogen molecule is composed of two hydrogen atoms HA and HB. In the ground state, each hydrogen atom has one electron 1s -orbital.
- These atomic orbitals may be represented by the wave functions iff and i/fg which represent the amplitudes of the electron waves of the atomic orbitals of the two atoms HA and HB respectively.
According to the LCAO method, the linear combination of atomic orbitals to form molecular orbitals can take place by addition and subtraction of wave functions of the individual atomic orbitals as shown below:
⇒ \(\psi_{\mathrm{b}}=\psi_{\mathrm{A}}+\psi_{\mathrm{B}} \text { and } \psi_{\mathrm{a}}=\psi_{\mathrm{A}}-\psi_{\mathrm{B}}\)
These two types of combinations give rise to two molecular orbitals. The molecular orbital if formed by the addition of wave functions of the two atomic orbitals is called bonding molecular orbital (BMO) and the molecular orbital formed by the subtraction of wave functions of the two atomic orbitals is called antibonding molecular orbital (ABMO).
- The combination of Is -orbitals of the two H-atoms to form molecular orbitals is shown in the given figure. It becomes clear from the figure that in the bonding molecular orbital, the electron density is mainly concentrated between the two positive nuclei.
- This high electron density between the two nuclei decreases their mutual repulsion and holds the nuclei together. Therefore, the hooding molecular orchid always possesses lower energy than either of the combining atomic orbitals. Electrons placed In it bond molecular orbital
- Formation of molecular orbital by a combination of li-atomic orbital stabilizes a molecule. On the other hand, in the antibonding molecular orbital, most of the electron density is mainly located away from the space between the nuclei, creating a node In between them.
- As a consequence, the two nuclei repel each other strongly. Therefore, the antibonding molecular orbital always possesses higher energy than either of the combining atomic orbital and the electrons placed in the antibonding molecular orbital destabilize the molecule.
- The formation of bonding and antibonding molecular orbitals can also be explained In terms of constructive interference (or additive effect) and destructive interference (or subtractive effect) of the electron waves of the combining atoms.
Bonding molecular orbital:
During constructive Interference, the two electron waves are in phase and the amplitudes of the waves get added up and reinforce each other. As a consequence, there is high electron density between the two nuclei, favoring bond formation. The resulting wave corresponds to a bonding molecular orbital.
Antibonding molecular orbital:
When the two electron waves of two combining atoms arc out of phase, there is destructive interference, and the amplitudes of the waves get subtracted. Thus, the resulting wave is weakened and consequently, there is low electron density between the nuclei.
Note that the crests of the electron wave are usually given by the’ +’ sign and the troughs by the ‘- ‘ sign. The bonding molecular orbital is formed by a combination of ‘+’ with’ +’ or with part of the electron waves whereas the antibonding molecular orbital is formed by the combination of ‘ + ’ with the ‘- ‘ part. For a homo-dinuclear molecule, since, if =, the amplitude of ABMO is zero.
Nodal plane:
In the antibonding molecular orbital, the plane perpendicular to the line joining the two nuclei where the probability of finding the electron (i.e., electron density) is zero, is called the nodal plane.
Energy of bonding and antibonding molecular orbitals
Linear combination of two atomic orbitals of hydrogen, for example, gives rise to a bonding molecular orbital of lower energy (higher stability) and an antibonding molecular orbital of higher energy (lower stability).

The energy difference between the bonding molecular orbital and the combining atomic orbitals is known as stabilization energy and the energy difference between the antibonding molecular orbital and the combining atomic orbitals is known as destabilization energy. Further, it may be noted that bonding MO is stabilized to the same extent (A) as the antibonding MO is destabilized.

An electron occupying the bonding molecular orbital lowers the energy ofthe system while an electron occupying the antibonding molecular orbital raises the energy of the system by an equal amount.

Different types of molecular orbitals
The molecular orbitals of diatomic molecules are designated as cr (sigma), 7r(pi), d(delta), etc.
σ-molecular orbitals:
The molecular orbitals formed by overlapping of atomic orbitals along the internuclear axis are called sigma (σ) molecular orbitals. Such molecular orbitals are symmetrical about the internuclear axis or bond axis.
Antibonding sigma molecular orbitals are expressed by the symbol cr. To denote the constituent orbital from which any molecular orbital is formed, the atomic orbital is mentioned beside the symbol of the molecular orbital or as its subscript.
Example: Combination of two σ∗1s -orbitals results in the formation of curls and cr s molecular orbitals.
Formation Of σ∗1s and one antibonding MO of higher energy \(\sigma_{2 s}^*\)
In the same way, additive and subtractive combinations of two Is orbitals result in the formation of curls and crl5 molecular orbitals respectively.

By the combination of two 2pz-atomic orbitals:
According to modem convention, the z-axis is taken as the internuclear axis. Hence, the 2pz -orbital is assumed to lie along the internuclear axis.
Therefore, the molecular orbital formed by the addition of wave functions of two 2pz -orbitals is a bonding σ-MO designated as cr2p the molecular orbital formed by the subtraction of wave functions of two 2pz -orbitals is an antibonding σ-MO designated as
⇒ \(\sigma_{2 p_z}^*\).

x-molecular orbitals:
The molecular orbitals that are formed by sideways or lateral overlap of two atomic orbitals are called pi (π) molecular orbitals. Such molecular orbitals are not symmetrical about the internuclear axis.
Formation of π -molecular orbitals:
By the combination of two 2px -atomic orbitals:
The axis of px -atomic orbital, according to modem convention, is perpendicular to the internuclear axis.
The Molecular orbital formed by the lateral overlap of two 2px- atomic orbitals involving the addition of electron waves is a bonding π-MO designated as 7r2p and the molecular orbital formed by the lateral overlap of two 2px -atomic orbitals involving the subtraction of electron waves is an antibonding π-MO designated as \(\pi_{2 p_x}\)

By a combination of two 2py-atomic orbitals:
The axis of py -the atomic orbital, according to the modem convention, is perpendicular to the internuclear axis.
Therefore, the lateral additive combination of two parallel 2py -orbitals leads to the formation of a bonding π-MO designated as π 2py, and the lateral subtractive combination of two parallel 2py orbital leads to the formation of an antibonding n -MO designated as \(\pi_{2 p_y}^*\).

Differences between σ and π- molecular orbitals

Conditions For the combination of atomic orbitals from molecular orbitals
The following conditions must be satisfied for the combination of atomic orbitals to form molecular orbitals;
The energies of the combining atomic orbitals must be the same or nearly the same.
Example: In the case of the formation of homonuclear species like H2, N2, or O2, the ls-orbital of one atom can combine with the Is-orbital of the other. But there is no possibility of the ls-orbital of any atom to combine with the 2s-orbital of another.
The extent of overlap between the combined atomic orbitals must be large.
The combining atomic orbitals must possess the same symmetry about the molecular axis, i.e., they must have proper orientations.
Examples: 2px -orbital of one atom can combine with 2px orbital of another atom but not with 2 py or 2pz orbital.
0 2s -orbital of an atom can overlap with the 2pz -orbital of another but not with 2 px or 2py, -orbital (which remain perpendicular to the internuclear axis). The reason is that in the second case, the overlapping of V with ‘+’ cancels the overlapping of V with ‘-‘.
The situation is shown below:

According to the present convention, the z-axis is taken as the internuclear axis.
- A bonding molecular orbital is formed by the addition of wave functions of two atomic orbitals.
- Antibonding molecular orbital is formed by subtraction of wave functions of two atomic orbitals.
- Combining atomic orbitals, and forming the molecular orbitals, must be of comparable energy.
- The axis of the pz -atomic orbitals of the combining atoms lie along the internuclear axis. So, pz -orbital is capable of forming cr -molecular orbital by overlapping along this axis.
- The axes of px and -atomic orbitals are perpendicular to the internuclear axis and hence they can form n-molecular orbitals with bilateral overlapping.
Energy level diagram of molecular orbitals:
Order of energy of homonuclear diatomic molecular orbitals
Two Is -orbitals of two atoms combine to form two molecular orbitals— crls and cr*s. In the same manner, two 2s-atomic orbitals give rise to two molecular orbitals (cr2i and or2S) and six 2p-atomic orbitals on combination give six molecular orbitals \(\left(\sigma_{2 p_z}, \sigma_{2 p_z}^*, \pi_{2 p_x}, \pi_{2 p_x}^*, \pi_{2 p_y}, \pi_{2 p_y}^*\right)\).
The energy sequence of these ten molecular orbitals can be determined by the following information:
The energies of molecular orbitals depend on the energies of the corresponding atomic orbitals involved in their formation. For example, since 2s-atomic orbitals have higher energy than tire Is -atomic orbitals, the pair of molecular orbitals obtained from 2s-atomic orbitals have higher energy than that obtained from Is -atomic orbitals.
Within the same pair of molecular orbitals, the bonding MO has lower energy than the antibonding MO.
For Example: \(\sigma_{1 s}<\sigma_{1 s}^*, \pi_{2 p_x}<\pi_{2 p_x}^* .\)
⇒ \(\pi_{2 p_x}\) and \(\pi_{2 p_y}\) molecular orbitals have equal and molecular orbitals also have equal energies i.e., they are also degenerate orbitals than the sideways or lateral overlapping.
This is quite true for O2 and molecules such as F2 and Ne2(hypothetical) where the energy difference between 2s and 2p -atomic orbitals are quite large. However, in molecules up to N2, the energy difference between these atomic orbitals is very small and the molecular orbitals <x2s and are so close that they experience mixing interactions.
(repulsion between the electrons present in them). As a result, the energy of cr2p orbital increases and becomes greater than N2p and N2p, which do not experience such intermixing interactions.
The energy of a2p molecular orbital is greater than that of N2p or N2p molecular orbital. From the above information and spectroscopic studies, it has been established that the energy of the first ten molecular orbitals of the homonuclear diatomic molecules or ions such as Li2, Be2 (hypothetical), B2, C2, N2 follow the order
⇒ \(\sigma_{1 s}<\sigma_{1 s}^*<\sigma_{2 s}<\sigma_{2 s}^*<\left[\pi_{2 p_x}=\pi_{2 p_y}\right]<\sigma_{2 p_z}\) \(<\left[\pi_{2 p_x}^*=\pi_{2 p_y}^*\right]<\sigma_{2 p_z}^*\)
The energy of the first ten molecular orbitals of the homonuclear diatomic molecules such as O2, F2, and Ne2 (hypothetical) follow the order:
⇒ \(\sigma_{1 s}<\sigma_{1 s}^*<\sigma_{2 s}<\sigma_{2 s}^*<\sigma_{2 p_z} <\left[\pi_{2 p_x}=\pi_{2 p_y}\right]\)\(<\left[\pi_{2 p_x}^*=\pi_{2 p_y}^*\right]<\sigma_{2 p_z}^*\)
The above two energy sequences ofthe molecular orbitals are shown in the following figures:

The difference in MO energy diagrams can be explained as follows. Since cr -bonds are generally stronger, therefore, it would be expected that cr{2p) orbital would be of lower energy than a comparable n{2p) orbited.
However, for most ofthe elements, the σ(2p) orbital lies at a higher energy than n{2p) orbitals because the difference between 2s and 2p atomic energy levels is small (except in the case of O2, F2, and Ne2 (hypothetical) where the difference in energy levels of 2s and 2p is large).
As a consequence, σ(2s), and σ(2p) are so close together that the repulsive forces between the electrons presenting them raise the energy of cr(2p) above that of n(2p) molecular orbitals. In the words, in the case of O2, F2, etc., there is no 2s-2p mixing, while for B2, C2, and N2, there is 2s-2p mixing.
Rules for filling up molecular orbitals
- Molecular orbitals get filled up with electrons according to the Aufbau principle. At first, the electrons enter the molecular orbital of the lowest energy and gradually that higher energy.
- Molecular orbitals can accommodate a maximum of 2 electrons which must have opposite spin (Pauli’s exclusion principle).
- The pairing of electrons in degenerate orbitals does not occur until each degenerate orbital is singly filled with electrons having parallel spin (Hund’s rule).
- Electrons presenting bonding molecular orbitals are called bonding electrons (Nb) and those in antibonding molecular orbitals are called antibonding electrons (Na).
Molecular Behavior and Electronic Configuration The important rules relating molecular behavior with electronic configuration are as follows:
- Stability of molecules in terms of bonding and antibonding electrons: From electronic configuration, we get the number of Nb and Na.
- If Nb > Ng, the molecule is stable. Because a greater number of bonding orbitals are occupied by electrons than antibonding orbitals, resulting in a net force of attraction (stronger bonding).
- IfNa < Nb, the molecule is unstable. Because a greater number of antibonding orbitals are occupied by electrons than bonding orbitals, resulting in a net force of repulsion.
- If Nb = Na, the molecule is unstable. Because the destabilization caused by electrons in antibonding molecular orbitals is greater than the stabilization gained by bonding electrons.
Bond order: The number of covalent bonds in a molecule is expressed by bond order. Bond order is defined as half the difference between the number of electrons present in bonding and antibonding orbitals,
⇒ \(\text { Bond Order (B.O.) }=\frac{1}{2}\left(N_b-N_a\right)\)
Important points regarding bond order
A molecule with B.0. 1, 2, or 3 indicates that it has a single bond, double bond, or triple bond respectively.
The relative stability of molecules in terms of bond order:
The stability (bond dissociation enthalpy) of the diatomic molecules is directly proportional to the bond order.
Thus, a molecule with bond order 3 (for example nitrogen, N =N, having bond dissociation enthalpy 945 kj mol‾1) is more stable than a molecule with a bond order 2 [e.g., oxygen, 0=0, having bond dissociation enthalpy 498 kj. mol¯1 ) which in turn is more stable than a molecule with a bond order 1 (Example fluorine, F—F, having bond dissociation enthalpy 158 kj. mol-1 ).
Bond length in terms of bond order:
Bond order is inversely proportional to bond length. For example, the bond length of the N2 molecule having bond order 3 is 1.10A whereas that of the O2 molecule having bond order 2 is 1.21A.
Magnetic nature of molecules:
- It can be predicted successfully by MO theory. If all the electrons in a molecule are paired, it is diamagnetic and if it contains one or more unpaired electrons, it is paramagnetic.
- The greater the number of unpaired electrons in a molecule or ion, the greater its paramagnetic nature. H2, for example, is diamagnetic while 02 is paramagnetic. The fractional value of bond order indicates that the molecule is paramagnetic.
Electronic configuration & nature of bonding of some homonuclear diatomic molecules & their ions
1. Hydrogen molecule (H2):
- An H2 molecule is formed by the combination of two H-atoms with one electron present in each -orbital. The two Is -orbitals combine mutually to form two molecular orbitals (trail and curls).
- The two electrons will occupy the lower energy curls MO and according to Pauli’s exclusion principle, the electrons have opposite spins. So, according to MO theory, the electronic configuration of the hydrogen molecule is 2
- . The MO energy level diagram for the H2 -H2-molecule is shown below.

Stability: A positive value of B.O. indicates that the H2 is – 1} stable. A much higher value of bond-dissociation energy (438kj. mol-1 ) of H2 indicates that it is a very stable molecule.
Magnetic nature: As the two electrons present in this molecule are paired, the molecule is diamagnetic.
2. Positive hydrogen ion (H2):
This is formed by the combination of the H -atom containing one electron and one H+ion having no electrons. Therefore, the H2 ion has only one electron which is occupied in the lower energy bonding MO i.e., curls orbital.
The electronic configuration of H2+ is 1. The following figure shows the MO energy level diagram of this ion.

Bond order of H2+ ion \(=\frac{N_b-N_a}{2}=\frac{1-0}{2}=\frac{1}{2}\)
Stability: Bond order positive. This shows that the Ion In somehow stable but it In less stable than, the molecule (bond dissociation enthalpy: H2+= 280 kj – mol-1 ). The existence of H2+ has been established spectroscopically.
Magnetic nature: From the electronic configuration, it is evident that the fl2 Ion contains one odd electron, Therefore, the ion Is paramagnetic.
3. Negative hydrogen ion (H2–):
When one hydrogen atom, 11 having one electron in its )s-orbital combines with a hydride Ion (H–) having two electrons in 1 s-orbital, the anion, (H2) is formed. Thus, the H2 ion contains three electrons.
Thus the electronic configuration of H2– ion: \(\left(\sigma_{1 s}\right)^2\left(\sigma_{1 s}\right)^1\)

Stability: A small positive bond order suggests that the ion is somewhat stable. Note that the H2 ion is slightly less stable than the H+ ion even though both have the same bond order (0.5). This is because the antibonding MO of H2 ion contains no electron whereas the antibonding MO of H2 contains one electron which causes destabilization.
Magnetic nature: Since the ion contains one unpaired electron, it is paramagnetic.
4. Helium molecule (He2):
Each He-atom has two electrons in Is -orbital. Therefore, the total number of electrons in the He2 molecule is four. Two of them occupy orbital while the other two occupy \(\sigma_{1 s}^*\) orbital.
Thus, the electronic brv configuration of He2 molecule is: \(\left(\sigma_{1 s}\right)^2\left(\sigma_{1 s}\right)^2\).
The MO diagram for this molecule is given as follows:
Bond order of He2 molecule ,\(=\frac{N_b-N_a}{2}=\frac{2-2}{2}=0\)

Energy diagram of molecular orbital of He2 molecule As bond order is zero, the He2 molecule has no real existence. In reality, helium gas consists of monoatomic molecules.
5. Helium molecule-cation (He2+):
This ion contains 3 electrons, two from one He -atom and one from one He+ ion. Two electrons occupy the bonding MO\(\left(\sigma_{1 s}\right)\) while the third electron occupies the antibonding MO (curls).
Thus the electronic configuration of He ion is: \(\left(\sigma_{1 s}\right)^2\left(\sigma_{1 s}\right)^1\). The MO energy level diagram for this ion is given below.

Bond order of \(\mathrm{He}_2^{+} \text {ion }=\frac{N_b-N_a}{2}=\frac{2-1}{2}=\frac{1}{2}\)
Stability: The positive value of bond order indicates that the formation of He2 ion is possible. Its bond dissociation enthalpy is 242.67kj. mol-1 .
Magnetic nature: Since the ion contains one unpaired electron, it is paramagnetic. 2 Note that the He. J Ion has the same bond order as the H2 ion and both have the same number of electrons in the antibonding orbitals. Therefore, they should have similar stability (bond dissociation enthalpy), bond length, and paramagnetic nature.
6. Lithium molecule (Li2):
The electronic configuration of lithium (Z = 3 ) is Is²2s¹. Thus, there are six electrons in the lithium molecule.
The electronic configuration of the Li2 molecule is written as:
⇒ \(\left(\sigma_{1 s}\right)^2\left(\sigma_{1 s}^*\right)^2\left(\sigma_{2 s}\right)^2 \text { or } K K\left(\sigma_{2 s}\right)^2\)
Where KK represents the closed K -K-shell structure:
⇒ \(\left(\sigma_{1 s}\right)^2\left(\sigma_{1 s}^*\right)^2\)
Bond order of Li2 molecule \(=\frac{N_b-N_a}{2}=\frac{4-2}{2}=1\)
Stability: From the value of bond order it is clear that there is a single bond between the two Li -atoms and therefore, the Li2 molecule is stable.
Magnetic nature: Since it has no impaired electron, it is diamagnetic.
7. Beryllium molecule (Be2):
The electronic configuration of beryllium (Z = 4) is ls²2s². So, the Be²molecule contains a total of eight electrons. The electronic configuration of the Be2 molecule, is, therefore, written as:
⇒ \(K K\left(\sigma_{2 s}\right)^2\left(\sigma_{2 s}^*\right)^2\)
Bond order of Be2 molecule= \(=\frac{N_b-N_a}{2}=\frac{2-2}{2}=0\).
As the bond order of the Be2 molecule is zero, it has no real existence. These predictions from MO theory are in agreement with the fact that diamagnetic Be molecules are found to exist in the vapor phase as monoatomic molecules
8. Boron molecule (B2):
The electronic configuration of boron(Z = 5) is 1s²2s²2p¹. So, there are ten electrons in the B2 molecule.
The electronic configuration of B2 is, therefore, written as:
KK\(\left(\sigma_{2 s}\right)^2\left(\sigma_{2 s}^*\right)^2\left(\pi_{2 p_x}\right)^1\left(\pi_{2 p_y}\right)^1\)
Bond order of B2 molecule = \(\frac{N_b-N_a}{2}=\frac{4-2}{2}\)
= 1
Stability: The molecule has bond order, 1. So it is somewhat stable. The bond dissociation enthalpy of the B2 molecule is 290 kl-mol-1
Magnetic nature: Since the molecule contains two unpaired electrons (one each in π2px and π2py MO ), it is paramagnetic
9. Carbon molecule (C2):
The electronic configuration of carbon (Z = 6) is ls²2s²2p². There are twelve electrons in the C2 molecule. The electronic configuration of the C2 molecule Is written as
KK \(\left(\sigma_{2 s}\right)^2\left(\sigma_{2 s}^*\right)^2\left(\pi_{2 p_x}\right)^2\left(\pi_{2 p_y}\right)^2\)
Bond order of C2 molecule \(=\frac{N_b-N_a}{2}=\frac{6-2}{2}\)
= 2
Stability: Since the bond order Is 2, the molecule is stable. The bond dissociation enthalpy of C2 is 620 kj-mot-1. The two bonds present in the C2 molecule are both K bonds because of the presence of four electrons in two n -n-molecular orbitals. This is different from the usual double bonds that are made up of σ -bond and an π -bond.
Magnetic nature: Since a die molecule contains no unpaired electrons, it is diamagnetic. Diamagnetic C2 molecules have been detected in the vapor phase.
10. Nitrogen molecule (N2): The electronic configuration of nitrogen (Z = 7 ) is ls22s22p3.
Thus the total number of electrons present in the N2 -molecule is 14. The electronic configuration of N2 can, therefore, be written as:
KK \(K K\left(\sigma_{2 s}\right)^2\left(\sigma_{2 s}\right)^2\left(\pi_{2 p_x}\right)^2\left(\pi_{2 p_y}\right)^2\left(\sigma_{2 p_z}\right)^2\)
Bond order of N2 molecule = \(=\frac{N_b-N_a}{2}=\frac{8-2}{2}\)
= 3
Generally, the completely filled \(\sigma_{1 s} \text { and } \sigma_{1 s}^*\) are not consideredin the calculation ofbond order.

Stability:
The bond order value of 3 suggests that the two nitrogen atoms are linked to each other by a triple bond (N = N). This in turn suggests that the molecule must have n much higher value of bond dissociation enthalpy greater stability (compared to all other diatomic molecules) and a shorter bond length. This is in agreement with the experimentally determined values of bond dissociation enthalpy (945kj mol-1 ) and bond length ( 1. 10 Å). Molecular nitrogen is, therefore, quite inert to chemical combinations.
Magnetic nature: The presence of no unpaired electron indicates that the molecules diamagnetic in nature
11. Oxygen molecule (O2):
The electronic configuration of oxygen (Z = 8 ) is ls22s22p4 Thus O2 molecule contains a total of 16 electrons.
The electronic configuration of O2 molecules, therefore, is written as:
KK \(\left(\sigma_{2 s}\right)^2\left(\sigma_{2 s}^*\right)^2\left(\sigma_{2 p_z}\right)^2\left(\pi_{2 p_x}\right)^2\left(\pi_{2 p_y}\right)^2\left(\pi_{2 p_x}^*\right)^1\left(\pi_{2 p_y}^*\right)^1\)
In the case of elements having atomic numbers greater than nitrogen, the energy of σ 2pz orbital is lower than that of π2px or π2py orbital.
Bond order of O molecule = \(=\frac{N_b-N_a}{2}=\frac{8-4}{2}\)
= 2
Stability: The bond order value of 2 suggests the presence of a double bond in the O2 -molecule. Thus the molecule is considerably stable (bond dissociation enthalpy: 501 kj . mol-1.).
Magnetic nature: The presence of two unpaired electrons in \(\pi_{2 p_x}^* \text { and } \pi_{2 p_y}^*\) -molecular orbitals accounts for the paramagnetic nature ofthe molecule. The molecule is weakly attracted by a magnetic field.

12. Superoxide ion (O2– ):
O2– Ion Is formed by the addition of one electron to O -molecule \(\mathrm{O}_2+e \rightarrow \mathrm{O}_2^{-}\). This electron enters into \(\pi_{2 p_x} \text { or } \pi_{2 p_y}\) molecular orbital. The electronic configuration of 02 ion, is, therefore, written as:
⇒ K K\(\left(\sigma_{2 s}\right)^2\left(\sigma_{2 s}^*\right)^2\left(\sigma_{2 p_z}\right)^2\left(\pi_{2 p_x}\right)^2\left(\pi_{2 p_y}\right)^2\left(\pi_{2 p_x}^*\right)^2\left(\pi_{2 p_y}^*\right)^1\)
Bond order of \(\mathrm{O}_2^{-} \text {ion }=\frac{N_b-N_a}{2}=\frac{8-5}{2}=1.5\)
Stability: Since its bond order is lower than that of O2, its bond dissociation enthalpy is lower and its bond length is longer than that of O2.
Magnetic nature: Owing to the presence of one unpaired electron, it is paramagnetic.
13. Peroxide ion (O22- ) ⇒ \(\mathrm{O}_2^{2-}\) ion is formed when O2 accepts two electrons: \(\mathrm{O}_2+2 e \rightarrow \mathrm{O}_2^{2-}\)
These two electrons enter into molecular orbitals
Therefore, the electronic configuration of O2- ion can be written as:
KK \(\left(\sigma_{2 s}\right)^2\left(\sigma_{2 s}^*\right)^2\left(\sigma_{2 p_z}\right)^2\left(\pi_{2 p_x}\right)^2\left(\pi_{2 p_y}\right)^2\left(\pi_{2 p_x}^*\right)^2\left(\pi_{2 p_y}^*\right)^2\)
Bond order of \(2_2^{2-} \text { ion }=\frac{N_b-N_a}{2}=\frac{8-6}{2}=1\)
Stability: Since its bond order is lower than that of O2. its bond dissociation enthalpy is lower and the bond length is longer than that of O2.
Magnetic nature: Since the ion contains no unpaired electron, it is diamagnetic
Relative bond dissociates lot enthalpies, liabilities, and bond lengths of
⇒ \(0_2(B .0,=2), 0_2^*(8,0,-2.5), 0_2^{-}(B .0,=1.5)\)
- Bond dissociation energy: Bond dissociation enthalpy is directly proportional to bond order. Hence, bond dissociation enthalpies follow the order \(\mathrm{O}_2^{+}>\mathrm{O}_2>\mathrm{O}_2^{-}>\mathrm{O}_2^{2-}\)
- Stability: The greater the bond order, the greater the stability The stability order Is: \(\mathrm{O}_2^{+}>\mathrm{O}_2>\mathrm{O}_2^{-}>\mathrm{O}_2^{2-}\)
- Bond length: As bond length Ls is inversely proportional to bond order, the bond lengths of these species follow the order: \(\mathrm{O}_2^{2-}>\mathrm{O}_2^{-}>\mathrm{O}_2>\mathrm{O}_2^{+}\)
14. Fluorine molecule (F2):
The electronic configuration of fluorine (Z = 9) is 1s22s22p6. Thus molecule contains a total of 18 electrons.
The electronic configuration of the F2 -molecule is, therefore, written as:
⇒ \(K K\left(\sigma_{2 s}\right)^2\left(\sigma_{2 s}^*\right)^2\left(\sigma_{2 p_z}\right)^2\left(\pi_{2 p_x}\right)^2\left(\pi_{2 p_y}\right)^2\left(\pi_{2 p_x}^*\right)^2\left(\pi_{2 p_y}^*\right)^2\)
Bond order of F2 molecule \(=\frac{N_b-N_a}{2}=\frac{8-6}{2}=1\)
Stability: Since its bond order is 1, its bond dissociation enthalpy (stability) is not too high (129 kj mol‾1 ).
Magnetic nature: The absence of unpaired electrons indicates the diamagnetic nature of the F2 molecule.
15. Neon molecule (Ne2):
The electronic configuration of (Z = 10) is ls22s22p6. So, the total number of electrons present in Ne2 -molecule =10+10 = 20.
The electronic configuration of the Ne2 molecule is, therefore, written as:
KKI \(\left(\sigma_{2 s}\right)^2\left(\sigma_{2 s}^*\right)^2\left(\sigma_{2 p_z}\right)^2\left(\pi_{2 p_x}\right)^2\left(\pi_{2 p_y}\right)^2\left(\pi_{2 p_x}^*\right)^2\left(\pi_{2 p_y}^*\right)^2\left(\sigma_{2 p_z}^*\right)^2\)
Bond order of Ne2 molecule \(=\frac{N_b-N_a}{2}=\frac{8-8}{2}=0\)
Since the bond order is zero, no bonds are formed between the two Ne -atoms, or in other words, Ne is a monoatomic gas and the Ne2 molecule does not exist. Thus, both He (discussed before) and Ne are monoatomic gases. Hence, it can be concluded that the noble gas elements are monoatomic in nature.
Molecular orbital population along with molecular properties of diatomic molecules:






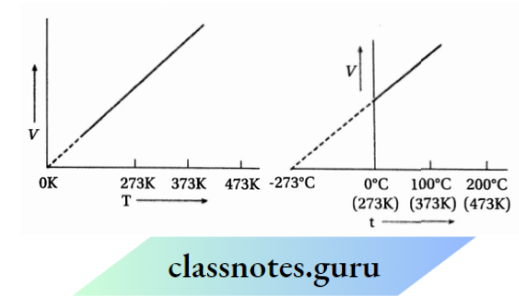








































































































































































































































































































 molecules and are always optically active.
molecules and are always optically active.





























































































































































 are not obtained as intermediates because these compounds are more reactive than benzene.
are not obtained as intermediates because these compounds are more reactive than benzene.