
Acute Gingival Infections
Acute Gingival Infections Important Notes
1. Acute Necrotizing Ulcerative Gingivitis (ANUG)
- Also known as vincents infection, vincents stomatitis, trench mouth, fetid stomatitis, putrid stomatitis
- Smears from the lesions of ANUG show spirochaetes and fusiform bacilli
Acute Necrotizing Ulcerative Gingivitis Clinical Features:
- Punched out crater-like depressions at the crest of interdental papilla covered by pseudomembrane and extending into marginal gingiva
- The pseudomembranous slough is demarcated from the remaining gingival mucosa by linear erythema
- Attached gingiva and alveolar mucosa are rarely involved
Read And Learn More: Periodontics Question and Answers
Acute Necrotizing Ulcerative Gingivitis Zones:
- Listergarten described 4 zones in ANUG
- Bacterial zone
- Neutrophil rich zone
- Necrotic zone
- Zone of spirochaetal infiltration
- Mouthwash Used:
- 3% H2O2 with an equal dilution of water every 2 hours for 3 days gives the best results in patients with ANUG
- It creates an oxidative environment and prevents the growth of an anaerobic environment
2. Stages of ANUG
3. Predisposing factors of ANUG
- Local
- Smoking
- Pericoronal flaps – Injury to the gingiva
- Pre-existing gingivitis
- Systemic
- Nutritional deficiency
- Debilitating diseases
- Psychosomatic
4. Factors causing the recurrence of ANUG
- Pericoronal flap
- Inadequate local therapy
- Anterior overbite
5. Pericoronitis
Pericoronitis Clinical Features:
- Red, painful, swollen, and tender gingiva
- Radiating pain to ear, throat
- Foul taste
- Inability to close mouth
Pericoronitis Treatment:
- Gentle flushing with warm water to remove debris and exudate
- Swabbing with antiseptic after elevating the flap gently from the tooth with a scaler
- Antibiotics in severe cases
- If the flap is swollen and fluctuant, an incision may be necessary to establish drainage
- After the inflammation subsides, the tooth should be extracted
6. Pseudomembrane formation
- Pseudomembrane is seen in ANUG, diphtheria, erythema multiforme, leukemic ulcers, syphilis, and candidiasis
- Pseudomembrane can be easily removed in ANUG
- Undetachable in syphilis
- Difficult to remove in diphtheria
7. Primary herpetic gingivostomatitis
Primary herpetic gingivostomatitis is a primary infection of the oral cavity caused by the HSV type 1 virus
Primary Herpetic Gingivostomatitis Clinical Features:
- High-grade fever
- Lymphadenopathy Soreness of mouth
- Vesicles that rupture to form ulcers
- Ulcers are typically present in masticatory mucosa
- Preschool children are affected mostly by it
- Secondary herpes may manifest as herpes labialis, herpes genitalis, and ocular herpes. It occurs due to stimulation of latent virus in neuronal ganglia
Primary Herpetic Gingivostomatitis Treatment:
- Treatment is palliative
- Local anesthetic mouthwash
- Increased water intake
- Pain control
- Supportive antibiotics
- Lesions subside within 7-10 days
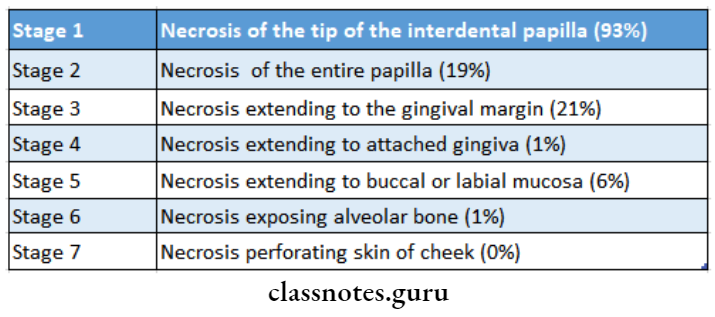
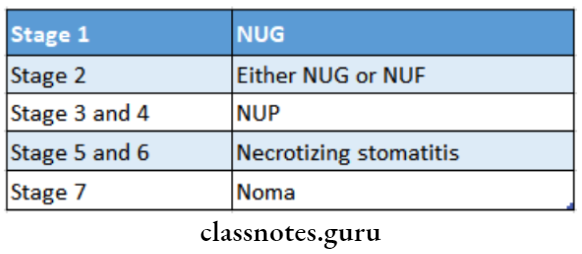
8. Staging of oral necrotizing disease by Horning and Cohen
Acute Gingival Infections Long Essays
Question 1. Describe the etiology, clinical features, and treatment of acute necrotizing ulcerative gingivitis.
Answer:
Acute Necrotizing Ulcerative Gingivitis (ANUG):
Acute Necrotizing Ulcerative Gingivitis (ANUG) It is an inflammatory destructive disease of the gingiva
Acute Necrotizing Ulcerative Gingivitis (ANUG) Etiology:
- Bacteria- fusospirochaetal organisms and bacteroids intermedius
- Predisposing factors
1. Local predisposing factors:
- Pre-existing gingivitis
- Injury to gingiva
- Smoking
2. Systemic predisposing factors:
- Nutritional deficiency
- Debilitating diseases
- Psychosomatic factors
Acute Necrotizing Ulcerative Gingivitis (ANUG) Clinical Features:
1. Intraoral signs:
- Punch out crater-like depression
- Covering of pseudomembranous slough
- Gingival hemorrhage
- Fetid odor
- Increased salivation- pasty saliva
- Sensitive to touch
- Radiating gnawing pain
- Increased pain on having spicy foods
- Metallic foul taste
2. Extraoral signs:
- Lymphadenopathy
- Fever
- Loss of appatite
- Lassitude
- Leucocytosis
Acute Necrotizing Ulcerative Gingivitis (ANUG) Stages Of Progresson:
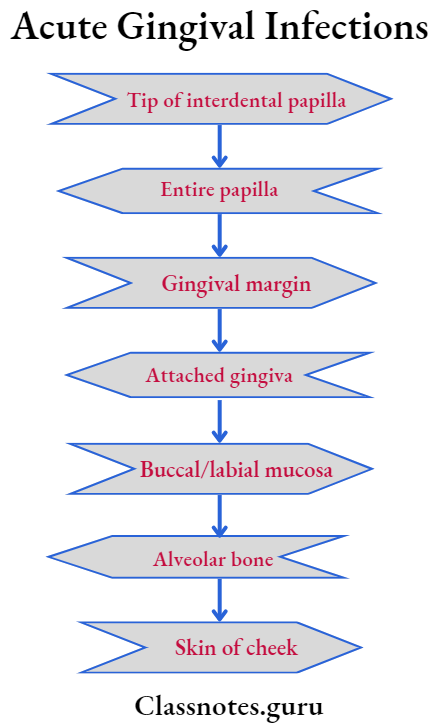
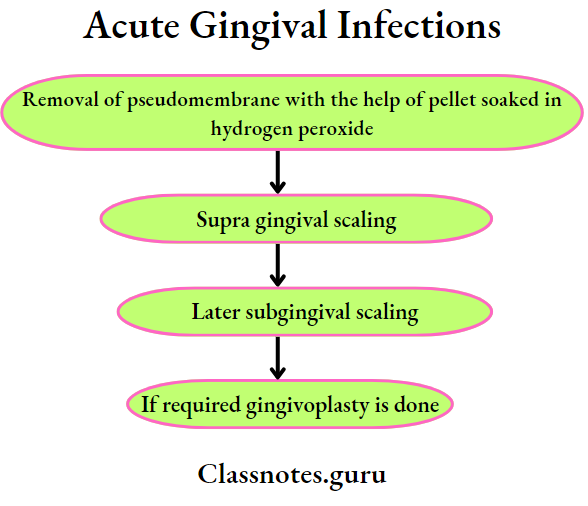
Acute Necrotizing Ulcerative Gingivitis (ANUG) Treatment:
1. Antibiotic coverage.
- Penicillin 500 mg TDS
- Metronidazole- 200-400 mg BID
2.
Question 2. Enumerate acute gingival infections. Describe the clinical features and management of ANUG.
Answer:
Acute Gingival Infections:
1. Traumatic lesions:
- Physical injury
- Chemical injury
2. Viral infections:
- Acute herpetic gingivostomatitis
- Herpangina
- Measles
- Zoster virus infection
3. Bacterial infection:
- Aug
- Tuberculosis
- Syphilis
4. Fungal diseases:
- Candidiasis
5. Gingival abscess:
6. Aphthous ulceration:
- Erythema multiforme
- Drug allergy
Acute Necrotizing Ulcerative Gingivitis:
- It is an inflammatory destructive disease of the gingiva
Question 3. Describe etiology, clinical features, and differential. diagnosis of acute herpetic gingivostomatitis.
Answer:
Acute Herpetic Gingivostomatitis:
Acute Herpetic Gingivostomatitis is an acute infection of the oral cavity
Acute Herpetic Gingivostomatitis Etiology:
Acute Herpetic Gingivostomatitis is caused by the herpes simplex type-I virus
Acute Herpetic Gingivostomatitis Clinical Features:
- Age-occurs during childhood
- Headache
- Fever
- Nausea, anorexia
- Lack of tactile and sensory sensation
- Sore throat
- Drooling of saliva
- Bilateral cervical lymphadenopathy
- Irritability
- Myalgia
- Site involved
- Gingiva
- Hard palate
- Dorsum of tongue
- Lips
- Vermillion border
- Perioral skin
- Nasopharynx
- Present as shiny erythematous gingival swelling
- Reddening of the oral mucosa
- Formation of numerous small, dome-shaped, or pin-head type vesicle
- Size-2-3 mm in diameter
- Vesicles contain clear fluid and rupture to form ulcers
- Ulcers are multiple, small, circular, punctuate, shallow and painful
- Have red margins and yellowish or greyish floor
- Small ulcers fuse to form diffuse, large, whitish ulcers
- Difficulty in swallowing
- Increased bleeding
- Soreness of the oral cavity
- Sensitive to touch
- Numerous vesicle formations over the tonsillar area and posterior pharynx
Acute Herpetic Gingivostomatitis Differential Diagnosis:
- Aug
- Erythema multiforme
- Lichen planus
- Steven-Johnson syndrome
- Desquamative gingivitis
Question 4. Define gingival abscess. Write in detail about the etiology and treatment of it.
Answer:
Gingival Abscess:
- A gingival abscess is a localized, acute inflammatory lesion that may arise from a variety of sources including microbial plaque, trauma, and foreign body impaction
Gingival Abscess Etiology:
- When bacteria are carried deep into tissues due to the -full embedding of foreign particles into gingiva-like
- Toothbrush bristles
- Piece of apple core
- Lobster shell fragment
Gingival Abscess Clinical Features:
- Involves marginal gingiva or interdental papilla
- It appears as red swelling with a smooth shiny surface
- Sudden in onset
- It is a rapidly expanding lesion
- Within 24-48 hours the lesion usually becomes fluctuate- ant and points with the surface orifice
- Lesion generally ruptures spontaneously
- The adjacent teeth are often sensitive to percussion
Gingival Abscess Treatment:
- Administration of topical or local anesthesia
- Scaling and root planning
- Drainage of abscess
- The fluctuant area is incised and the exudate is drained by gentle digital pressure
- Irrigation of area with water
- Cover the area with a gauge under light pressure
- Once bleeding is stopped, relieve the patient
- Instruct the patient to rinse with warm salt water every 2 hours
- After 24 hours the area is reassessed
Acute Gingival Infections Short Essays
Question 1. Aphthous Ulcers.
Answer:
Aphthous Ulcers is a common disease characterized by the development of painful, recurrent, solitary ulceration of the oral mucosa
Aphthous Ulcers Etiology:
- Immunological abnormalities:
- Due to T cell-mediated immunological abnormality
- Genetic predisposition
- Increased susceptibility to RAS
- Microbial organism
- Form L form of a hemolytic streptococci
- Systemic factors
- Nutritional deficiency
- Cyclic neutropenia
Aphthous Ulcers Classification:
- Minor aphthae: the ulcers are less than 1 cm in diameter
- Major aphthae: they are over 1 cm in diameter
- Herpetiform ulcers: they are small ulcers throughout the mucosa
Aphthous Ulcers Clinical Features:
- Age and sex: common in women in the second and third decade of life
- Site: it occurs most commonly on buccal and lingual mucosa, tongue, soft palate, pharynx, and gingiva
- Prodromal symptoms:
- Next ulcer appears
- The ulcer gradually enlarges over the next 48-72 hours
- Later symptoms
- The lesion is typically painful
- It interferes with eating for several days
- It begins as a single or multiple superficial erosion covered by grey membrane it is surrounded by localized areas of erythema
- Lesions are round, symmetrical and shallow
- Multiple lesions are present
1. Minor aphthae:
- Size: 0.3-1 cm
- They heal without scar formation within 10-14 days
2. Major aphthae:
- Size: upto 5 cm in diameter
- They interfere with speech and eating
- The large portion may be covered with deep painful ulcers The lesions heal slowly and leave scars
- Due to it there is decreased mobility of the uvula and tongue
3. Herpetiform ulcers:
- Multiple small shallow ulcers often up to 100 in number
- It begins as small pinhead-size erosions that gradually enlarge in size
- Lesions are more painful
- It is present continuously for one to three years
- Patients get relief immediately with 2% tetracycline mouthwash
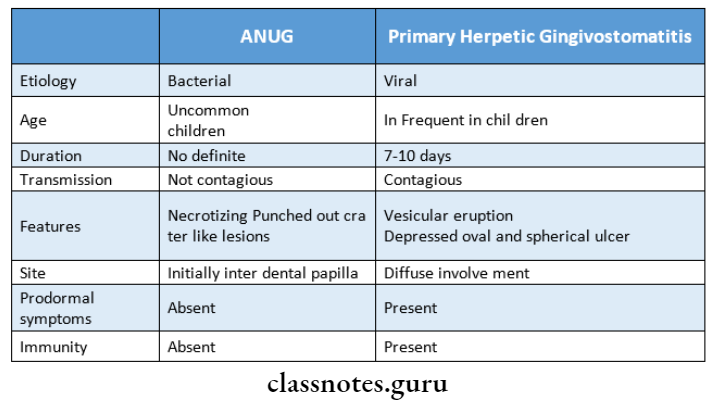
Question 2. Differentiate between ANUG and primary herpetic gingivostomatitis.
Answer:
Question 3. Pericoronitis.
Answer:
Pericoronitis Definition:
- Inflammation of gingiva and surrounding soft tissues of an incompletely erupted tooth
- ITIS – Inflammation ‘PERI’ – Surrounding `CORO’ – Crown
Pericoronitis Types: Acute, Sub-acute, or chronic
Pericoronitis Features:
- Red, erythematous lesion
- Tenderness
- Radiating pain
- Difficulty in closing jaws
- Foul taste
- Swelling of the cheek region
Pericoronitis Sequel:
- Pericoronal abscess
- Cyst formation
- Spread of infection into adjacent areas
- Lymphadenitis
- Peritonsillar abscess
- Cellulitis
- Ludwig’s angina
Pericoronitis Treatment:

Cleanse and Anesthetize the area
- Reflection of flap
- Debridement
- Post-operative instructions
- Rinse with warm water along with salt
- Copious fluid intake
- Systemic antibiotics
- Recall
- Next visit decide
- To retain tooth
- To extract
- Impaction
Acute Gingival Infections Short Answers
Question 1. Differential diagnosis of acute herpetic gingivostomatitis.
Answer:
- AUG
- Erythema multiforme
- Lichen planus
- Steven-Johnson syndrome
- Desquamative gingivitis
Question 2. Management of acute herpetic gingivostomatitis.
Answer:
- Antiviral therapy 15 mg/kg of acyclovir suspension given 5 times daily for 7 days
- Scaling- to remove plaque and food debris
- Topical application of chlortetracycline
- Administration of NSAIDs
- Nutrient supplements
- Relief of pain by topical anesthetic mouthwash
Question 3. Diagnosis of acute herpetic gingivostomatitis.
Answer:
- Diagnosis is made by
- History
- Clinical examination
- Virus culture
- Immunologic tests
Question 4. Bacterial microflora of ANUG.
Answer:
- Treponema micodentium
- Intermediate spirochaetes
- Vibrios
- Fusiform bacilli
- Filamentous organisms
- Borrelia species
Question 5. Enumerate acute infections of the gingiva
Answer:
1. Traumatic lesions:
- Physical injury
- Chemical injury
2. Viral infections:
- Acute herpetic gingivostomatitis
- Herpangina
- Measles
- Zoster virus infection
3. Bacterial infection:
- Aug
- Tuberculosis
- Syphilis
4. Fungal diseses
- Candidiasis
5. Gingival abscess
6. Aphthous ulceration
- Erythema multiforme
- Drug allergy
Question 6. Define gingival abscess.
Answer:
A gingival abscess is a localized, acute inflammatory lesion that may arise from a variety of sources including microbial plaque, trauma, and foreign body impaction
Gingival Abscess Etiology:
- When bacteria are carried deep into tissues due to the force-fully embedding of foreign particles into gingiva-like
- Toothbrush bristles
- Piece of apple core
- Lobster shell fragment
Acute Gingival Infections Viva Voce
- ANUG and Vincent angina are fusospirochaetal infec- tions
- 3% H2O2 diluted to one part peroxide and 2 parts water twice a day is recommended in patients with desquamative gingivitis
- Spirochaetes are classified into 3 groups: small, in- intermediate, and large
- Intermediate spirochaetes are present in great numbers in ANUG
- Dark field microscopy is used to demonstrate spiro-chapters
- Corticosteroids are contraindicated in ANUG
- Extraction and periodontal surgery should be planned 4 weeks after the signs and symptoms of ANUG have subsided
- Herpes is common in preschool children
- ANUG is common in adolescents
- Juvenile periodontitis is common in young adolescents
- Viridians group of streptococci and anaerobes pre- dominate in samples collected in pericoronitis
- Aphthous ulcers are predominately present in labial mucosa.
- Color changes of Gingiva is diffuse in acute herpetic gingivostomatitis gingivostomatitis
- Diffuse erythema of the Gingiva with no ulcers is seen in streptococcal gingivostomatitis
- Necrotizing ulcerative gingivitis is caused by spiro- chapters and fusiform bacilli
- Herpetic gingivostomatitis is a viral infection
- Vesicles in herpetic gingivostomatitis rupture approximately after 24 hours
- Tzanck cells are seen in herpetic
- Healing of the lesions with scarring is seen in large aphthous ulcers
- The pseudomembrane in ANUG should be removed at the first visit
- Amoxicillin is the drug of choice in ANUG