
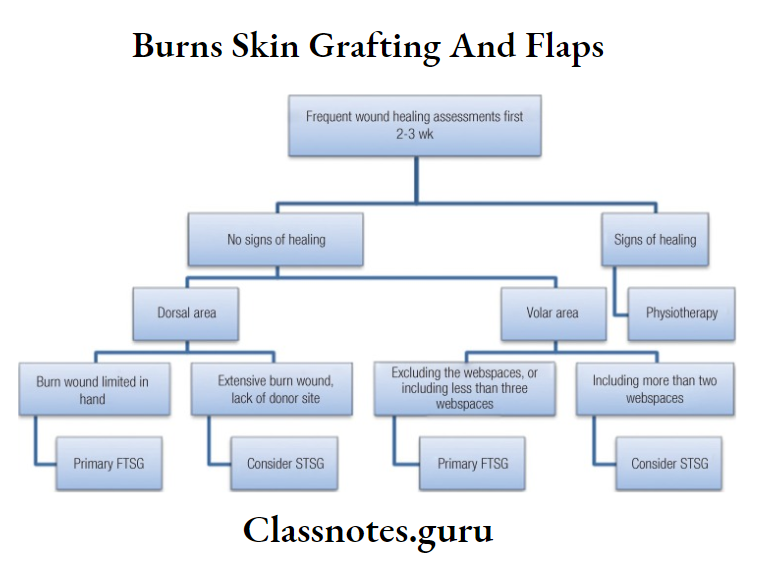
Burns Skin Grafting And Flaps Important Notes
- Depth Of Burns
- Depth Of Burns First degree
- Burns are confined to the epidermis
- They are painful, erythematous, and blanch to touch with an intact epidermal barrier
- Depth Of Burns Second Degree
- Divided into two types- superficial and deep
- Have some degree of dermal damage
- Depth Of Burns Third-degree
- Involves the epidermis and dermis
- Characterized by a hard, leathery eschar
- It is painless due to nerve damage
- Black, white, or cherry red
- Wounds heal by re-epithelization from the wound edges
- Deep dermal and full-thickness burns require excision with skin grafting
- Fourth Degree
- Burns involve other organs beneath the skin such as muscle, bone, and brain
- Depth Of Burns First degree
- Burns Skin Grafting And Flaps Classification
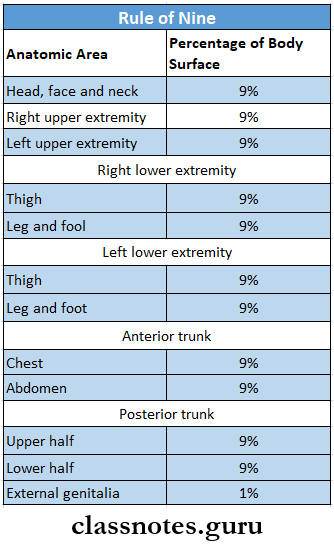
- Rule Of Nine
- Given by Wallace
- Used to calculate the severity of burns
- Head and neck – 9%
- Upper limb ( right and left) – 18%
- Thorax (front and hack) – 18%
- A Women (front and back) – 18%
- Lower limb ( front and back ) – 18%
- Lower limb ( right and left) – 18%
- Lxtemal genitalia – 1%
- Electrical Burns
- In it, the visible areas of tissue necrosis represent only a small portion of destroyed tissue
- Electrical current enters a part of the body through fingers or hand
- Proceeds through tissues with lower resistance to current such as nerves, blood vessels, and muscles
- The current then leaves the body at a grounded area typically the foot
- The muscle is the major tissue through which the current flows and thus it sustains the most damage
- Electrical Burns Features And Effects
- Patients may develop cardiac dysrhythmias
- Muscle damage results in the release of hemochromogens which are filtered in glomeruli
- May result in obstructive nephropathy
- Port wine-colored urine may be present
- A large amount of blood pigment may be deposited in the collecting tubules of the kidney as a result of hemolysis
- Hemoglobinuria will be gradually followed by oliguria ia and anuria, and the patient may die of uremia
- Management Of Burns
- Fluid replacement
- In 10% of burns in children
- In more than 15% of burns in adults
- The formula to calculate fluid replacement is
- % of burns * body weight / 2
- Use of nasogastric tube in >35% burns
- Blood replacement therapy in 25-50% burns
- Fluid replacement
- Effects Of Burns
- Local Effects
- Cell necrosis
- Collagen denaturation
- Infection
- Inflammation
- Systemic Effects
- Hypovolaemia
- Gastric or duodenal ulcer
- Multiple organ transfer
- Hypoxia
- Local Effects
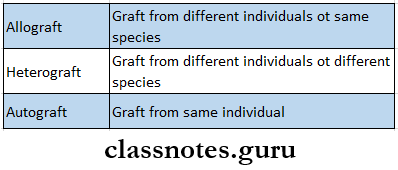
- Types Of Grafts
Burns and skin grafting question and answers
Burns Skin Grafting And Flaps Long Essays
Question 1. Classification of burns
Answer:
Classification Of Burnauburnernurn is a wound in which the tissues are coagulatively necrosised.
Read And Learn More: General Surgery Question and Answers
Burns Classification:
- According To The Mechanism Of Injury
- Ordinary Burns
- Caused by dry heat like fire, open flame, airplane injury
- Scalds
- Caused by moist heat
- Example: hot liquid or hot steam
- Electric Bums
- Caused by low voltage electrical sources
- Tissue damage occurs
- The skin gradually undergoes coagulation necrosis
- It causes minimal destruction of skin
- The skin is involved at two points- at the point of contact and the point of exit
- Electrical injury to the muscles is associated with the release of haemo chromogens into the bloodstream
- Chemical Burn
- Caused by strong acid or base
- The severity of damage is related to the concentration of the chemical and duration of contact
- Radiation Injury
- Usually caused by x-rays or radium
- Radiodermatitis occurs which are of two types
- Acute radiodermatitis- exposure dose is highly excessive
- Chronic radiodermatitis- occurs due to small doses of irradiation
- Cold Burns
- Caused by exposure to cold like freezing injury, frostbite, trench foot
- Causes coagulative necrosis of tissue
- Ordinary Burns
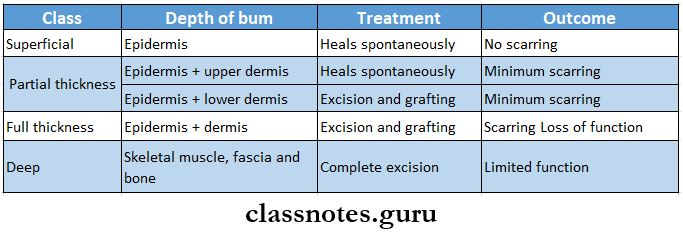
- According To Burn Depth
- First Degree Burn
- Involves epidermis only
- Manifests as erythema, painful, dry texture
- Heals in a week or less
- Second Degree Burn
- The entire thickness of the epidermis is destroyed
- Blebs or vesicles are formed between the separating epidermis and dermis
- Third Degree Burns
- Involves full thickness of the dermis
- Appears a stiff and white or brown scar
- Absence of pain
- Fourth Degree Burn
- Extends through skin, subcutaneous tissue, and into underlying muscle and bone
- Result in amputation and severe functional impairment
- First Degree Burn
- According To Burn Severity
- Major Burns
- Full thickness burns
- Associated with inhalational injury, electrical burns
- Require referral to a specialized burn treatment center
- Moderate Burns
- Full-thickness burns involving 2-10% of total body surface area
- Require hospitalization for burn care
- Minor Burns
- Full-thickness burns involving less than 2% of total body surface area
- Do not require hospitalization.
- Major Burns
Question 2. Pathology and treatment of burns and management of 50% burns in a person aged 40 years.
Answer:
Burns Pathology:
- Local Changes
- Severity of burn
- First degree burn
- Hyperemia of the skin with slight edema of the epidermis
- Second degree burns
- The entire thickness of the epidermis is destroyed
- Formation of blebs and vesicles
- Third degree burns
- Destruction of the epidermis and dermis
- First degree burn
- Severity of burn
- Extent Of Burn
- It is expressed as a percentage of the total surface area
- Estimated by the rule of nines
- Vascular Changes
- Dilatation of small vessels
- Local liberation of histamine
- Increased blood flow to the injured part
- Increased capillary permeability
- Blister formation
- Infection
- Due to the destruction of the epidermis, there is a loss of barrier against infection
- This causes severe infection
- Systemic Changes
- Shock
- Biochemical changes
- Electrolyte imbalance
- Hypoproteinaemia
- Hyperglycaemia
- Rise in blood urea and creatinine levels
- Changes In Blood
- Haemoconcentration
- Rise in hemoglobin level
- Increase in the number of RBCs
- Sludging of blood
- Fall in eosinophil count
- Aggregation of RBC, WBC, and platelets
- Anaemia
- Alteration in coagulation
- Systemic Lesions
- Extent Of Burn
Treatment of Burns:
- Treatment Of Shock
- Sedation
- As burn is very painful sedatives and analgesics are prescribed
- Administered during first 4-5 days
- Usually, injection of morphine is preferred
- Fluid Resuscitation
- Started as soon as possible
- A blood transfusion is required
- Ringer’s lactate solution is used
- Maintenance Of Airway
- Administration of 100% oxygen with ventilation support
- Sedation
- General Treatment
- Tetanus Prophylaxis
- Intramuscular administration of tetanus toxoid in the dose of 0.5 ml usually provides adequate prophylaxis
- Antibiotics
- Microorganisms contaminate the wound
- Thus systemic antibiotics are given on 1st or 2nd day of injury
- Nutritional Support
- Feeding is supported by a nasogastric tube through which nutrients are delivered. 24 hours a day
- Gastric Decompression
- Requires introduction of nasogastric suction as intestinal motility is gradually lost
- Gastric aspirates should be regularly monitored
- Tetanus Prophylaxis
- Local Treatment
- First-Aid Measures
- The patient is immediately removed from the source
- Apply cool clean water to the area
- Burn Wound Care
- The wound is cleansed with a surgical detergent and all loose nonviable skin is removed
- Blister is punctured
- Regular dressing is carried out
- Skin Grafting
- Excise the wound
- The patient’s donor skin can lie meshed to increase the size of the graft
- It is then covered with cadaveric skin
- First-Aid Measures
Skin Grafting And Flaps Management: Fluid Resuscitation
- The goal is to maintain the vital organ function as soon as possible
- Several formulas are proposed
- Evans’ Formula
- 1st 24 hours
- Normal saline- 1/2 ml/kg/% burn
- 2000 ml of 5% dextrose
- Colloid-containing fluid- 1 ml/kg/% burn
- 2nd 24 hours
- Normal saline- 1/2 of l st 24 hours
- 2000 ml of 5% dextrose
- Colloid containing fluid- 1/2 of 1st 24 hours
- 1st 24 hours
- Brooke’s Formula
- 1st 24 hours
- Ringer’s lactate solution 1.5 ml/kg/% burn
- Colloid containing fluid 0.5 ml/kg/% burn
- Dextrose solution- 2000 ml
- 2nd 24 hours
- Ringer’s lactate solution 1/2 – 3/4 th of 1 st 24 hours
- Colloid containing, solution 1/2 to 3/4 of 1st 24 hours
- Dextrose solution 2000 ml
- 1st 24 hours
Flaps in oral surgery questions and answers
Question 3. Define burns and scalds. Discuss management of 20% burns.
Answer:
Burns And Scalds Definition:
- Burns Burn is a wound in which there is coagulative necrosis of the tissue
- Scalds It is a thermal injury or burn caused by moist heal
Burns and Scalds Management:
- First-Aid Measures
- Remove the patient from the source
- Wrap the patient in a fire blanket
- Apply running cold water
- Remove clothing
- Maintain patent airway
- Airway Maintenance
- Breathing and ventilation
- Circulation is maintained
- Fluid resuscitation
- Wound Care
- Analgesic are preferred
- A blood transfusion is required
- Use of antibiotics to prevent infection
- Nutritional support
- Debridement of wound
- Regular dressing
- Excision of the devitalized tissues
- Skin grafting
Management of burns questions for medical students
Burns Skin Grafting And Flaps Short Essays
Question 1. Burn shock
Answer:
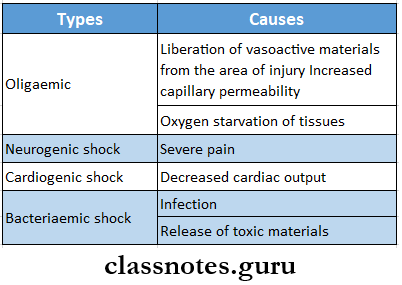
Burn Shock
- Shock is the most important effect of burns
- Burn Shock Types
Burn Shock Treatment:
- Sedation
- As the bum is very painful sedatives and analgesics are prescribed
- Administered during first 4-5 days
- Usually, injection of morphine is preferred
- Fluid Resuscitation
- Started as soon as possible
- A blood transfusion is required
- Ringer’s lactate solution is used
- Maintenance Of Airway
- Administration of 100% oxygen with ventilation support
Full thickness and split-thickness grafts questions
Question 2. Superficial burns
Answer:
Superficial Burns
- First-Degree Burns Are Called Superficial Burns
- Involves epidermis only
- Manifests as erythema, painful, dry texture
- Heals in a week or less
Superficial burns Management:
- First-Aid Measures
- Remove the patient from the source
- Wrap the patient in a fire blanket
- Apply running cold water
- Wound Care
- Analgesic are preferred
- Debridement of wound
Question 3. Rule of nine in burns
Answer:
Rule Of Nine In Burns
- The length and width of the burn wound are expressed as a percentage of the total surface area displaying 2nd or 3rd-degree burn
- The extent is estimated by the rule of nines which is as follows:
- It applies only to adults
Burns classification questions with answers
Question 4. Burns
Answer:
Burns: A burn is a wound in which there is coagulative necrosis of the tissues.
Burns Classification:
- According To The Mechanism Of Injury
- Ordinary burns
- Scalds
- Electric burns
- Chemical bums
- Radiation burns
- Cold burns
- According To Bum Depth
- First-degree bum
- Second-degree bum
- Third-degree bum
- Fourth-degree bum
- According To Severity
- Major bums
- Moderate bums
- Mild bums
Burns Management
- Treatment Of Shock
- Sedation
- As the bum is very painful sedatives and analgesics are prescribed
- Administered during first 4-5 days
- Usually, injection of morphine is preferred
- Fluid Resuscitation
- Started as soon as possible
- A blood transfusion is required
- Ringer’s lactate solution is used
- Maintenance Of Airway
- Administration of 100% oxygen with ventilation support
- Sedation
- General Treatment
- Tetanus Prophylaxis
- Intramuscular administration of tetanus toxoid in the dose of 0.5 ml usually provides adequate prophylaxis
- Antibiotics
- Microorganisms contaminate the wound
- Thus systemic antibiotics are given on 1st or 2nd day of injury
- Nutritional Support
- Feeding is supported by a nasogastric tube through which nutrients are delivered 24 hours a day
- Gastric Decompression
- Requires introduction of nasogastric suction as intestinal motility is gradually lost
- Gastric aspirates should be regularly monitored
- Tetanus Prophylaxis
- Local Treatment
- First-aid Measures
- The patient is immediately removed from the source
- Apply cold clean water to the area
- First-aid Measures
- Bum Wound Care
- The wound is cleansed with a surgical detergent and all loose nonviable skin is removed
- Blister is punctured
- Regular dressing is carried out
- Skin Grafting
- Excise the wound
- The patient’s donor skin can be meshed to increase the size of the graft
- It is then covered with cadaveric skin
Question 5. Skin Grafting
Answer:
Skin Grafting
Skin grafting is a surgical procedure involving the transplantation of skin or a skin substitute over a bum or nonhealing wound
Skin Grafting Indications:
- Extensive raw wound
- Large wound due to trauma or burn
- Contracted scar
- Skin loss from surgically removed malignant growth
- In reconstructive surgeries
Skin Grafting Types:
- Split Thickness
- Includes epidermis and a variable amount of dermis
- Healing occurs by re-epithelization from the dermis and surrounding skin
- Full Thickness
- Includes epidermis and all the dermis
- The donor site is sutured
- Composite Graft
- These are small grafts containing skin and underlying cartilage or other tissue
Burns and skin grafting viva questions
Question 6. PMMC flap
Answer:
PMMC Flap Procedure:
- Skin below and medial to nipple over the muscle is used
- The incision is made over the skin
- Below the line or 3rd rib to retain the deltopectoral hap area
- The lower border of the muscle is raised
- Care is taken to avoid injury to thoracoacromial vessels
- The flap is raised over the medial and lateral margins of the pectoral and is the major muscle
- Skin with muscle is dissected from the deeper structures
- The flap is raised upwards upto the coracoid
- Lateral pectoral vessels are retained
- Pectoral nerves should be retained
- The defect below is usually closed primarily with sutures
- The flap is tunneled in the subcutaneous plane towards the neck or oral cavity
- Postoperatively flap is observed for color changes, seroma, and infection
- The neck is flexed towards the flap side
- A suction drain is placed
- Neck flap covers the carotids
- In the case of the oral cavity, skin can be split in half to cover both the inner and outer aspects of the oral cavity
PMMC Flap uses:
- To cover the defect over the cheek/neck/pharynx/ intraoral lesions after wide excision
- Used along with deltopectoral flap.
Skin flaps and grafts dental question bank
Burns Skin Grafting And Flaps Short Answers
Question 1. Split skin grafting
Answer:
Split Skin Grafting
- Split skin grafting includes epidermis and variable amount of dermis
- Donor Sites
- Thigh
- Buttock
- Healing occurs by re-epithelization from the dermis and surrounding skin
Split Skin Grafting Indications:
- Resurfacing large wound
- Lining cavities
- Resurfacing mucosal deficits
- Closure of flap donor sites
- Resurfacing muscle flaps
Split Skin Grafting Types:
- Thin- 0.005-0.012 inch
- Intermediate-0.012-0.018 inch
- Thick- 0.018-0.030 inch
Split Skin Grafting Disadvantages:
- More fragile
- Cannot withstand radiotherapy
- Contract during healing
- Gets hypo or hyperpigmented
- Less esthetic
- Lack of smooth texture
Question 2. Composite skin graft
Answer:
Composite Skin graft
- Composite skin graft contains more than one tissue like skin, bone, tendons, cartilage, and muscle
- For example, it is used in the treatment of basal cell carcinoma
Composite Skin graft Procedure:
- A graft is excised from the donor site
- A desired shape is obtained from it
- It is picked using a special instrument
- Placed over the injured part
- Secured in place with the help of sutures
Indications of skin grafts – question and answer format
Question 4. Plasma expanders
Answer:
Plasma Expanders
Plasma expanders are high molecular weight substances which when infused IV exert osmotic pressure and remain in the body for a long time to increase the volume of circulating fluid
Plasma Expanders Ideal Properties:
- Should exert oncotic pressure comparable to plasma
- Should be long lasting
- Should be nonantigenic
- Should be pharmacologically inert
Burns first aid management questions
Plasma Expanders Plasma Expanders Used Are:
- Dextrans
- Gelatin polymer
- Hydroxyethyl starches
- Polyvinyl pyrrolidone
- Human albumin obtained from pooled human plasma
Question 5. Burns of face
Answer:
Burns Of Face
- Facial burns vary from superficial to deep burns.
- Over 50% of burns involve the head and neck region.
Burns Of Face Causes:
- Flame
- Electric current
- Steam
- Hot substances
- Chemicals
Burns Of Face Treatment:
- Objectives
- Restoration Of Function
- Airway patency
- Protection of cornea
- Neck mobility
- Restoration Of Function
- Comfort
- Appearance
Question 6. Skin grafting indications
Answer:
Skin Grafting indications
- Extensive raw wound
- Large wound due to trauma or bum
- Contracted scar
- Skin loss from surgically removed malignant growth
- In reconstructive surgeries
Question 7. Scalds
Answer:
Scalds
- Scald is a thermal injury or bum caused by moist heat such as boiling water, hot oil, or tar
- Injury is severe and sometimes life-threatening H Skin grafting is required
- Most thickness burn grafting results in scarring
- They result in a higher percentage of body surface area burned and longer stay in the hospital
Complications of skin grafting – dental questions
Question 8. Third degree burns
Answer:
Third-Degree Burns It involves of entire depth of the epidermis and dermis
Third Degree Burns Features
- It is painless due to the destruction of nerves Skin appears tough, dry, and eschar
- Thrombosed subcutaneous veins are seen
- In 3-5 weeks, eschar gets separated
Question 9. Types of skin grafting
Answer:
Types Of Skin Grafting
- Split Thickness
- Includes epidermis and a variable amount of dermis
- Healing occurs by re-epithelization from the dermis and surrounding skin
- Full Thickness
- Includes epidermis and all the dermis
- The donor site is sutured
- Composite Graft
- These are small grafts containing skin and underlying cartilage or other tissue
Question 10. Electric burns
Answer:
Electric Burns
- Caused by low voltage electrical sources
- Tissue damage occurs
- The skin gradually undergoes coagulation necrosis
- It causes minimal destruction of skin
- The skin is involved at two points – at the point of contact and the point of exit
- Electrical injury to the muscles is associated with the release of hemochromogens into the bloodstream
Classification of burns with clinical examples
Burns Skin Grafting And Flaps Viva Voce
- Head and trunk in severely burnedpatientstaccounts for 45% of total body surface
- Split-thickness grafts are used when the burns are extensive
- Full-thickness grafts used to cover small areas
- Lactated Ringer’s solution without dextrose is the fluid of choice except in children younger than 2 years
- 5% dextrose Ringer’s lactate is used in children