
Fractures General Principles Long Essays
Question 1. Lefort’s classification of fractures of the maxilla
Answer:
Lefort 1
Maxilla Clinical Features:
- Oedema of lower part of face
- Ecchymosis in buccal vestibule
- Bilateral epitaxis
- Mobility of upper teeth
- Disturbed occlusion
- Pain
- Upward displacement of fragment- telescopic fracture H ‘Cracked cup’ sound on percussion of upper teeth
- ‘Guerin sign- ecchymosis in the greater palatine region
Maxilla Management:
- Reduction
- Reduction of the impacted fragment with the help of disimpaction forceps (Rowe’s and William’s forceps)
- Placement of Rowe’s forceps:
- A straight blade is placed into the nostrils
- A curved blade is placed over the palate
- Placement of William’s forceps
- Placed over the buccal aspect
- Displaces maxilla in mesiodistal direction
- Fixation:
- Zygomatic suspension fixation is done
- Holes are drilled over the zygomatic arch
- Pass the wire through it
- Bring it up to the arches
- Twisted over are arch bars
- Inter Maxillary Fixation
- IMF done for 3-4 weeks
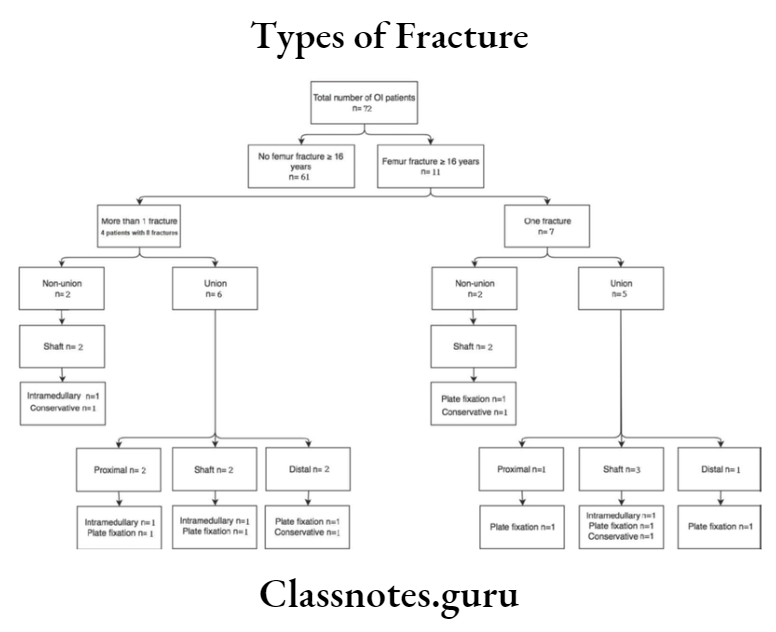
Types of bone fractures long essay
Lefort 2 Clinical Features:
- Cross edema of the middle third of the face.
- Ballooning of face
- Black eye
- Lengthening of face
- Bilateral subconjunctival hemorrhage
- Depressed nasal bridge.
- Anterior open bite
- Bilateral epistaxis
- Loss of occlusion
- Difficulty in mastication and speech
- Airway obstruction
- CSF leak
- Paraesthesia of cheek
- Step deformity
Read And Learn More: General Surgery Question and Answers
Lefort 2 Management:
- Reduction – reduction of the fragments through disimpaction forceps.
- Fixation Zygomatic suspension fixation is done,
- Inter – maxillary fixation
- It is done for 3-4 weeks.
Lefort’s 3 Clinical Features:
- Ballooning of face
- Panda facies
- Racoon eyes
- Bilateral subconjunctival hemorrhage
- Lengthening of face
- Separation of sutures
- ‘Dish face’ deformity
- Enophthalmus
- Diplopia
- Deviation of the nasal bridge
- Epitaxis
- CSF rhinorrhoea
Lefort’s 3 Management:
Bilateral frontomalar suspension
↓
Application of arch bars
↓
Intraosseous wiring
Classification of fractures in orthopedics
Question 2. Discuss the management of maxillofacial injuries
Answer:
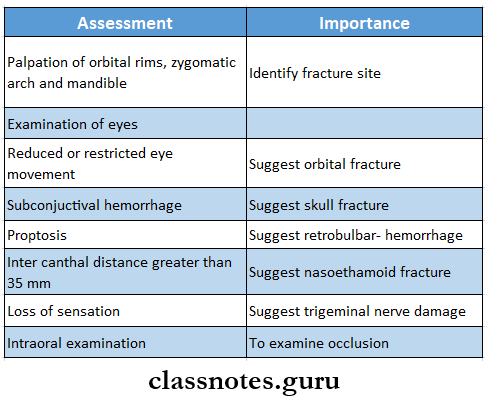
Management Of Maxillofacial Injuries:
1. Primary assessment
- Check for airway
- Bilateral anterior mandibular fractures have the risk of the tongue falling back, check for it
- Orotracheal intubation is carried out
- Hemorrhage is controlled
- Anterior and posterior nasal packing is used
2. Secondary assessment
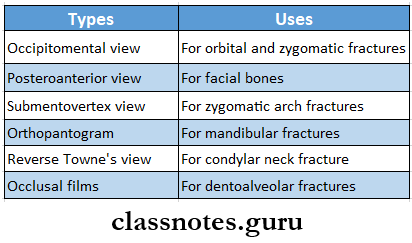
3. Radiography
Principles Of Management:
- Reduction
- Restoration of fractured fragments to their original position
- Brought by
- Closed reduction
- Open reduction
- Fixation
- Fractured fragments are fixed
- This prevents displacement of the fragments
- Consists of
- Direct fixation
- Indirect fixation
- Immobilization
- The fixation device is retained in position till a bony union is obtained
- Immobilization depends on the type of fracture and bone involved.
Question 3. Classify fractures of the face and discuss the management of each type of fracture
Answer:
Definition: Fracture is defined as a sudden break in the continuity of bone and it may be complete/incomplete
Fracture Classification:
- Lefort’s classification
- Lefort 1
- Lefort 2
- Lefort 3
- Erich’s classification
- Horizontal fracture
- Pyramidal fracture
- Transverse fracture
- Depending on the zygomatic bone
- Sub zygomatic
- Supra zygomatic
- Depending on level
- Low level
- Mid-level
- High level
Fracture Management:
- Open reduction
- In it, the fractured fragments are surgically exposed and visualized
- Indications
- Dislocation of the condyle into the middle cranial fossa
- Dislocation of condyle into the external auditory canal
- Lateral extracapsular displacement
- Inability to obtain the desired occlusion
- Bilateral subcondylar fractures in edentulous
- Bilateral subcondylar fractures associated with comminuted fractures
- Consists of
- Exposure of the site
- Detachment of the bone from all muscle attachments
- Reinserting
- Fixation of the segment
- Closed reduction
- In it, the fractured fragments are not openly visualized for anatomical alignment
- Consists of
- Manipulation of joint
- Intermaxillary fixation for 10 days
- Mobilization of the jaw
- Indications
- Fractures of the condylar neck that are not displaced
- Fractures of the condyle in children
- Intracapsular fractures
- Fixation
- The anatomically aligned fragments are then held in place by devices to fix it in that position
- It is divided into
- Nonrigid
- Semi-rigid
- Rigid
- Immobilization
- The fragments are retained without any movement for at least 4-6 weeks
- It enables callus formation and healing of fragments
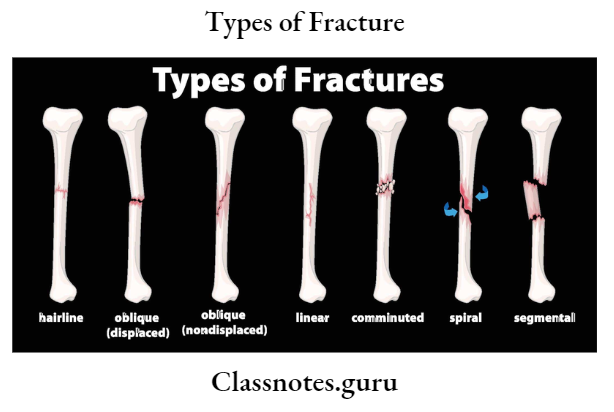
Essay on types of fractures
Question 4. Classify fractures. Describe the treatment of fractured mandible and clinical features.
Answer:
Fractured Mandible General Classification:
- Simple/ closed
- Doesn’t communicate with the exterior
- Compound
- It communicates with the exterior
- Comminuted
- Bone is crushed into pieces
- Complex
- Involvement of vital structures
- Impacted
- One fragment is driven into other
- Greenstick
- Fracture of one fragment and bending of other
- Pathological
- Superimposition of disease
Management Of Fractured Mandible:
- Closed Reduction And Indirect Fixation:
1. Wiring:
- Essig’s wiring
- Used to stabilize dentoalveolar structures
- Steps:
- Move the luxated teeth back to the position
- Adapt wire to the teeth
- Pass the wire’s one end buccally and the other lingually
- Join both ends
- Pass small wires interdentally and fix it
- Twist it, cut it, and adjust it interdentally
- Gilmer’s wiring
- The pre-stretched wire is passed around the individual tooth
- Both ends are brought together and twisted
- Repeat for each tooth
- Repeat for both the arches
- Final twisting of mandibular and maxillary wires
- Twist cut it, and adapt interdentally
- Risdon’s wiring
- Pass the wire around both the 2nd molar
- Both ends are twisted together
- Repeat for each tooth
- Both the base wires are bought to the midline
- Twisted together
- Cut it
- Adapt it to the neck of the teeth
- Eyelet wiring
- Prepare loops in the center of wire
- Two tails of the wire are passed interdentally
- One end is passed around the distal tooth from lingually to buccally
- Another end is passed around the mesial tooth lingually to buccally
- Twist both ends
- Cut it short
- Multiloop wiring
- Adapt solder wire around the buccal surface of the tooth
- Adapt wire buccally from the last molar to the midline
- Pass the other end distal to the 2nd molar over the lingual side
- Pass interdentally bring it to the buccal side by passing under the wire
- Now pass it from buccal to lingual
- Round it around the tooth
- Repeat the same procedure
2. Arch Bar Fixation:
- Arch Bar Fixation is a method of indirect fixation used in the management of mandibular fractures
- Open Reduction And Direct Fixation:
- Transosseous wiring or osteosynthesis
- Plating using compression plates
- Lag screw fixation
- Titanium or stainless steel mesh fixation
- Open Reduction And Direct Fixation:
Fractured Mandible Clinical Features:
- Change in the contour of the face
- Lacerations
- Ecchymosis of the floor of the mouth
- Occlusal disturbances
- Step deformity of the mandible
- Pain and tenderness rismus
- Deviated mouth opening
- Anesthesia and paraesthesia of the lower lip and chin
Long answer on bone fractures and types
Question 5. Clinical signs, symptoms, and general principles of treatment of fractures.
Answer:
Treatment Of Fractures Clinical Features:
- Pain at or near the site of fracture
- Tenderness or discomfort on gentle pressure over the area
- Swelling
- Loss of sensation
- The injured part cannot move normally
- The contracting muscles may cause the broken ends of the bone to override
- Irregularity of the bone
- Crepitus may be heard or felt
- Unnatural movement at the site of fracture
Principles Of Fracture Management:
- Reduction
- Restoration of fractured fragments to their original position
- Brought by
- Closed reduction
- Open reduction
- Fixation
- Fractured fragments are fixed
- This prevents displacement of the fragments
- Consists of
- Direct fixation
- Indirect fixation
- Immobilization
- The fixation device is retained in position till a bony union is obtained.
- It depends on the type of fracture and bone involved.