
Developing Dentition And Its Disturbances Important Notes
1. Developmental disturbances affecting the shape of teeth
2. Developmental disturbances affecting the size of teeth
3. Developmental disturbances in the number of teeth
Read And Learn More: Pedodontics Short Essays Question And Answers
4. Developmental disturbances affecting the structure of teeth
- Amelogenesis imperfecta
- It is a disorder of enamel formation
- Stages
- Stage 1 – Hypoplastic type
- Stage 2 – Hypomaturation type
- Stage 3 – hypo calcification type
- Stage 4 – Hypomaturation, Hypoplastic type
- Dentinogenesis imperfecta
- It is an inherited disorder of dentin formation characterized by excessive formation of defective dentin
- Types
- Type 1 – associated with osteogenesis imperfecta
- Type 2 – without osteogenesis imperfecta
- Type 3 – Bradywine type
- Dentin dysplasia
- It is an autosomal dominant inherited disorder causing defective dentin formation
- Types
- Type 1 – affects radicular dentin
- Type 2 – affects coronal dentin
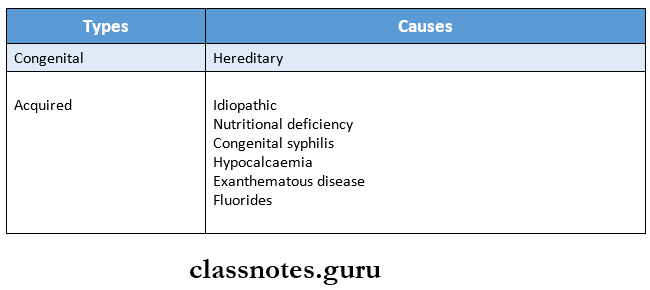
5. Enamel hypoplasia
- It is the incomplete or defective formation of the organic enamel matrix of teeth
- Types
6. Syndromes
Developing Dentition And Its Disturbances Short Essays
Question 1. Teething.
Answer:
- It means, in common terms, the eruption of primary dentition.
- Eruption of primary dentition begins in the 5th – 6th month of a child’s life.
Clinical Features:
- Local Features:
- Hypermia overlying erupting teeth.
- Flashing in the skin of the adjacent cheek.
- General Features:
- Irritability
- Crying
- Loss of appetite
- Sleeplessness
- Increased salivation
- Increased thirst
- Cough
- Systemic Problems:
- Fever
- Diarrhea
- Vomiting
- Cholera
- Infantile paralysis
- Local Problems:
- Eruption hematoma
- Eruption sequestrum
- Ectopic eruption
- Transposition
Management:
- Preventive Measures:
- Maintain the child’s oral hygiene.
- Wiping the gums with cotton soaked in antiseptic.
- Balanced diet/Nutritious diet.
- General Measures:
- Use of teething objects
- Toasted bread
- Hard fruits
- Teething necklaces
- Pacifiers
- Use of teething objects
- Medical Management:
- Topical application of glycerine, benzoyl alcohol.
- Use of mild purgatives.
- Use of soluble acetylsalicylic acid tablets
- In homeopathy, use of Chamomilla.
Question 2. Local and Systemic causes of delayed eruption.
Answer:
1. Local Causes:
- Aberrant tooth position
- Lack of space
- Early loss of deciduous
- Ectopic eruption
- Congenital anomalies
- Ankylosis of teeth
- Retained teeth
- Supernumerary
- Tumour
- Cyst
- Abnormal habit
2. Systemic Causes:
- Hypopituitarism
- Hypothyroidism
- Hypovitaminosis
- Cleidocranial dysostosis
- Achondroplasia
- Osteopetrosis
- Down’s syndrome
- Amelogenesis imperfecta
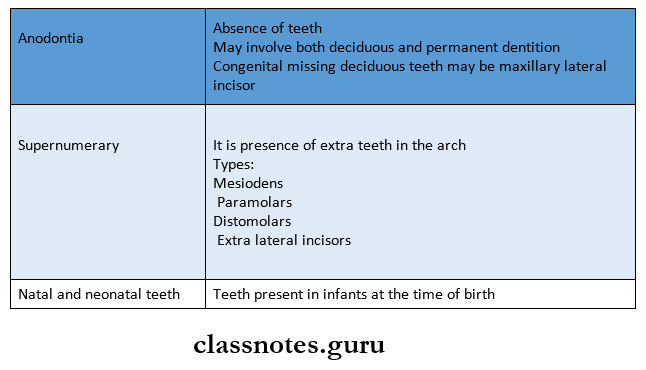
Question 3. Natal and Neonatal Teeth / Precociously Erupted Teeth.
Answer:
- Natal teeth are those teeth which are present at birth.
- Neonatal teeth are those teeth which erupt during the first 30 days.
- The prevalence of natal and neonatal teeth is very less.
- About 85% are mandibular primary incisors.
- They always occur in pairs.
Etiology:
- Disturbances in the position of the tooth germ.
- Febrile incidence affecting the increased rate of eruption.
- Hormonal stimulation.
- Hereditary
- Syndrome associated
Incidence:
- The teeth affected are:
- 85% – mandibular incisors
- 11% – maxillary incisors
- 3% – mandibular cuspids
- 1% – maxillary cuspids
Question 4. Causes of Enamel Hypoplasia.
Answer:
1. Focal Enamel hypoplasia
- It occurs either due to the spread of infection from deciduous teeth or trauma to deciduous teeth.
- This causes damage to the ameloblast cells forming the crown of the underlying permanent successor.
2. Generalised Enamel Hypoplasia
1. Nutritional Deficiency:
- Deficiency of Vitamin A, C, and D often causes injury to the ameloblast cells.
- Hypocalcemia secondary to Vitamin D deficiency.
2. Systemic Conditions:
- Childhood infections
- Rickets
- Congenital hypoparathyroidism
- Birth injuries that cause transient cessation of ameloblastic activity
- Children of low birth weight exhibit enamel hypoplasia resulting from oxygen and mineral depletion to the ameloblast cells.
- Mottling, a type of enamel hypoplasia, is produced due to fluoride toxicity.
Question 5. Supernumerary Teeth.
Answer:
The presence of any extra tooth in the dental arch in addition to the normal series of teeth is called a supernumerary tooth.
Location:
- They can occur in any location.
- These are common in the maxilla.
Types:
- Mesiodens – Located between two upper central incisors.
- Distomolars – Located on the distal aspect of regular molar teeth.
- Paramolars – These are extra molar teeth, which are usually located either in the buccal or lingual aspect of normal molars.
- Extra lateral incisors – Common in the maxillary arch.
Features:
- They may be either single or multiple in numbers.
- They are either erupted or impacted.
Effects:
- Supernumerary teeth may produce crowding.
- These are directly/indirectly responsible for increased caries incidence and periodontal problems.
- Multiple supernumerary teeth occur due to syn¬dromes.
- Impacted supernumerary teeth are associated with cyst-like dentigerous cysts.
Treatments:
- Nonfunctional supernumerary teeth need to be extracted.
Question 6. Pulp Stones.
Answer:
These are nodular calcified bodies having an organic matrix and they occur frequently in relation to the coronal pulp.
Types:
1. True Pulp Stones:
- Composed of predominantly dentin and have dentinal tubules.
2. False Pulp Stones:
- They are composed of concentric layers of calcified material.
According to their location
1. Free Pulp Stones:
- These are surrounded on all sides by pulpal tissue.
- They are not attached to the dentinal wall.
2. Attached Pulp Stones:
- These are attached to the dentinal wall of the pulp chamber.
3. Interstitial Pulp Stones:
- These are surrounded by reactionary or secondary dentin.
Associated Symptoms:
- The affected tooth is vital.
- Mild, neurologic pain is present.
Significance:
- The presence of pulp stones may cause difficulties during endodontic treatment.
Question 7. Amelogenesis is imperfect.
Answer:
- Amelogenesis imperfecta is a developmental defect of the enamel with a heterogenous etiology that affects the enamel of both the primary and permanent dentition
Etiology
- Genetic mutation
- It is an autosomal dominant trait
Clinical Features:
- It has a wide range of clinical appearance
- Enamel appears pitted with horizontal and vertical ridges
- There is defective maturation of the crystal structure
- Affected teeth are mottled, and opaque with white brown-yellowish discoloration
- They have enlarged pulp chambers
Types
- Hypocalcified type
- Hypomaturation type
- Hypoplastic type
Treatment:
- Veneering or capping of teeth
Question 8. Down’s Syndrome/ Trisomy 21
Answer:
- It may occur due to trisomy of chromosome 21
Predisposing Factors:
- Advanced maternal age.
- Placental abnormalities
- Chromosomal aberration.
Features:
1. General:
- Skull:
- Brachycephalic skull
- Presence of a third fontanelle
- Flat nasal bridges
- Eye-Oblique palpebral fissures:
- Cataracts, scanty eyelashes
- Neck:
- Short and broad
- Hands:
- Broad and short
- Multiple loops on fingertips.
- Muscles and joints:
- Hypotonicity and hyperextensibility.
2. Oral Manifestation
- Mouth
- Open mouth
- Drooling of saliva
- Tongue
- Fissured tongue, macroglossia
- Lip
- Dry, fissured
- Occlusion
- Anterior open bite
- Palate
- The high palate, clefts, bifid uvula
- Teeth
- Retarded eruption
- Hypodontia, microdontia
- Low incidence of caries
- Periodontium
- Poor oral hygiene
- Impaired phagocytosis
Developing Dentition And Its Disturbances Short Answers
Question 1. Ectopic Eruption.
Answer:
- The direction of the improper eruption of the permanent tooth can be termed as ectopic eruption.
Effect:
- It causes resorption of the primary tooth.
- Commonly Affected Teeth:
- Maxillary first permanent molar
- Mandibular anterior teeth
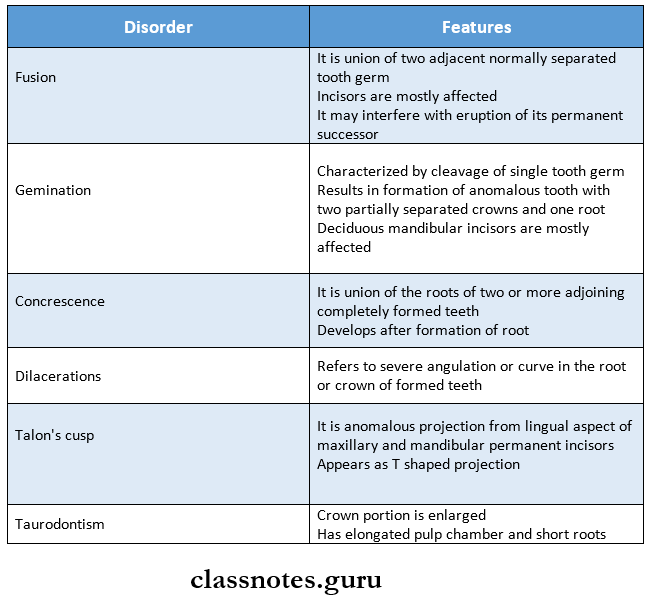
Question 2. Dilaceration.
Answer:
- Definition: It is an abnormal angulation or bends in the root of a tooth.
Etiology:
- An injury displacing the calcified form of the tooth germ.
- Secondary to the presence of a pathological condition.
Common Site:
- Dilaceration is commonly seen in the permanent maxillary incisors.
Question 3. Gemination and fusion.
Answer:
Question 4. Talon’s Cusp.
Answer:
- It refers to an accessory cusp-like structure projecting from the cingulum area of the maxillary or mandibular anterior teeth.
Etiology:
- It occurs as an outward folding of inner enamel epithelial cells and transient focal hyperplasia of the peripheral cells.
Features:
- It projects from the palatal surface of teeth and extends up to the incisal edge.
- In some cases, they are quite sharp while others have rounded and smooth tips.
Question 5. Taurodontism.
Answer:
- It is an abnormal enlargement of the body and pulp chamber of a multirooted tooth that leads to apical displacement of the pulpal floor.
Etiology:
- Hereditary
- Defect in the functioning of Hertwig’s epithelial root sheath.
Features:
- The commonly affected tooth is the third molar.
- It may be unilateral or bilateral.
- The tooth has short roots with an elongated pulp chamber.
- It lacks cervical constriction.
Question 6. Mammelons.
Answer:
It is any of the three rounded protuberances found on the incisal edges
- They occur on the newly erupted incisor.
- They are only present on permanent incisors.
- Soon after eruption, they are worn down by use.
Question 7. Premature loss of deciduous teeth.
Answer:
It refers to the loss of a tooth before its permanent successor is sufficiently advanced in development and eruption to occupy its place.
- Early loss of deciduous teeth can cause migration of adjacent teeth into the space.
- This prevents the eruption of the permanent successor.
- This further leads to malocclusion.
- For example:
- Loss of a deciduous second molar can cause a forward shift of the permanent first molar.
- This blocks the eruption of the second premolar which results in its impaction or deflection to an abnormal position.
Question 8. Retained Deciduous Teeth.
Answer:
- It refers to a condition where there is undue retention of deciduous teeth beyond the usual eruption age of their successor.
- This prevents the normal eruption of its successor.
- Prolonged retention of deciduous anterior results in lingual/palatal eruption of their permanent successors.
- Prolonged retention of buccal teeth results in buccal/lingual eruption of their permanent succes¬sors/their impaction.
Etiology:
- Absence of underlying permanent teeth.
- Hypothyroidism.
- Ankylosed deciduous teeth.
- Non-vital deciduous teeth.
Question 9. Ankylosis.
Answer:
- It is a condition wherein a part/whole of the root surface is directly fused to the bone with the absence of the periodontal membrane.
Etiology:
- Trauma to the tooth perforates the periodontal membrane.
- Certain infections.
- Endocrinal disorders.
- Congenital disorders.
Question 10. Eruption Sequence.
Answer:
1. Deciduous Teeth
- They erupt around 6-7 months of age
- Primary dentition is usually established by 3 years of age.
- Sequence is A-B-D-C-E
2. Permanent Teeth
- They may exhibit variation
- Frequently seen a sequence of eruptions is:
- 6-1-2-4-3-5-7 or 6-1-2-3-4-5-7
Question 11. Submerged Teeth.
Answer:
- Teeth that is located below the occlusal plane of the rest of the teeth in the arch.
- Commonly affected teeth are deciduous teeth.
- If the permanent teeth have erupted, it locks the sub-merged deciduous molar which usually becomes ankylosed.
- If the permanent teeth has not yet erupted, it gets impacted or may erupt buccally/lingually.
- A submerged tooth occurs because of the congenital absence of an underlying tooth.
Question 12. Turner’s Tooth.
Answer:
- In case of infections affecting the deciduous teeth, it spreads to the crown of underlying permanent teeth by affecting the ameloblast cells.
- Such an affected tooth is called “Turner’s Tooth”
Types: Depending on the severity of injury:
- Mild injury – Results in pitted areas on the enamel surface.
- Severe injury – Results in yellowish/ brownish discoloration of the surface.
Question 13. External Root Resorption.
Answer:
Pathological resorption initiated on the root/external surface of the tooth is called external root resorption.
Causes:
- Periapical inflammation.
- Reimplanted teeth.
- Impacted teeth.
- Cysts/Tumour
- Excessive occlusal forces
Effect:
- Nonvital tooth
- Teeth is easily fractured.
Question 14. Turner’s syndrome.
Answer:
It is caused by missing X chromosome
Clinical Features:
- Heart-shaped facies
- Prominent ears
- Webbing of posterior neck
- Low posterior hairline
- Congenital lymphedema
- Broad chest
- Hypogonadism
- Short stature
- Auditory defects
- Amenorrhea
- Sparse pubic hair
- Hypoplastic nails
- Pigmented nevi
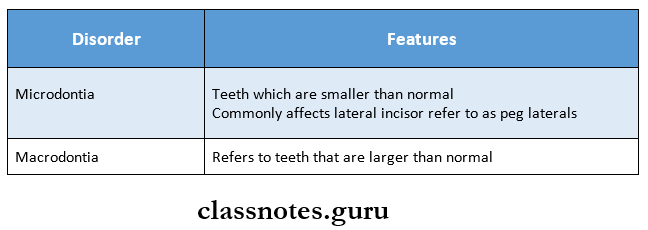
Question 15. Microdontia.
Answer:
It refers to the teeth that are smaller than normal
Types:
1. Truly generalized microdontia
- All teeth are smaller than normal
2. Relative generalized microdontia
- Normal or slightly smaller than normal
3. Microdontia affecting a single tooth
- It affects the maxillary lateral incisor and third molar
Treatment:
- No specific treatment is indicated
Question 17. Riga feds disease.
Answer:
- In 1881 and 1890 Riga and Fede described this lesion
- Hence it is known as the Riga-Fede disease
- It is one of the complications of the natal teeth
- In this condition laceration, traumatic ulceration of the ventral surface of the tongue, and frenulum of the lip due to the sharp incisal edge of the natal teeth are seen
- The more appropriate and descriptive term is neonatal sublingual traumatic ulceration
Treatment:
- Teeth may have to be removed
- Inflamed tissue around teeth should be controlled by applying chlorhexidine gluconate gel three times a day
Question 18. Munchausen syndrome by Proxy.
Answer:
- In Munchausen syndrome by proxy, children below 6 years of age and too young to reveal the deception exhibit parentally fabricated or induced illness
Clinical Features:
- Bleeding from various sites
- Recurrent sepsis from injecting contaminated fluids
- Chronic diarrhea from laxatives
- Fever from rubbing or heating thermometers
- Rashes from rubbing the skin or applying caustic substances
Question 19. Fusion
Answer:
- Fusion arises through the union of two normally separated tooth germs
- Depending upon the stage of development of the teeth at the time of the union, fusion may be either complete or incomplete
- It may occur between a normal tooth and a supernumerary teeth
- Associated with spacing and periodontal conditions
Question 20. Dens invaginatus
Answer:
- It refers to folding or invaginatus on the surface of the tooth towards the pulp before calcification of the tooth
Types:
1. Coronal type
- In it invagination occurs on the crown portion of the tooth
- Type 1 – invagination occurs within the crown of the tooth
- Type 2 – invagination extends below center- name junction
- Type 3 – invagination extends through the root
2. Radicular type
- Invagination occurs in the root portion of teeth
Clinical Forms
- Mild
- Intermediate
- Extreme
Significance
- Susceptible to
- Caries
- Pulpitis
- Pulp necrosis
- Periapical cyst
- Periapical abscess
Developing Dentition And Its Disturbances Viva Voce
- The eruption sequence of primary dentition is ABDCE
- The eruption sequence of permanent dentition is 6124357 or 6123457
- Natal teeth are teeth present at birth
- Neonatal teeth are seen within the first 30 days of birth
- The most common complication of natal teeth is Riga- Fede disease
- Fusion is the joining of two tooth buds
- Concrescence is the joining of two teeth by cementum
- Dentinogenesis imperfect is an autosomal dominant trait
- Dentin dysplasia is characterized as rootless teeth