
Dental Caries Definitions
1. Early childhood caries
Davies defined early childhood caries as a complex disease involving maxillary incisors within a month after the eruption and spreading rapidly to another primary teet
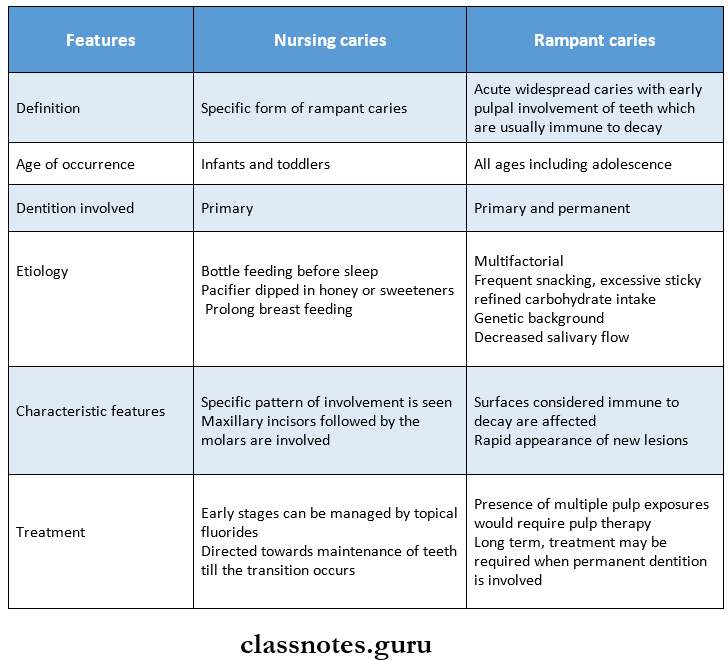
2. Rampant caries
It is an acute widespread caries with early pulpal involvement of teeth which are usually immune to decay
3. Nursing bottle caries
Caries caused by prolonged use of a bottle filled with any liquid other than the water
Read And Learn More: Pedodontics Short Essays Question And Answers
Dental Caries Important Notes
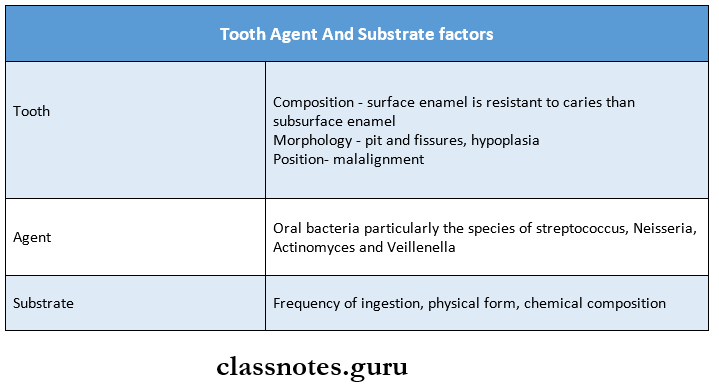
1. Keys triad
It includes a host (tooth), Agent, and substrate factors
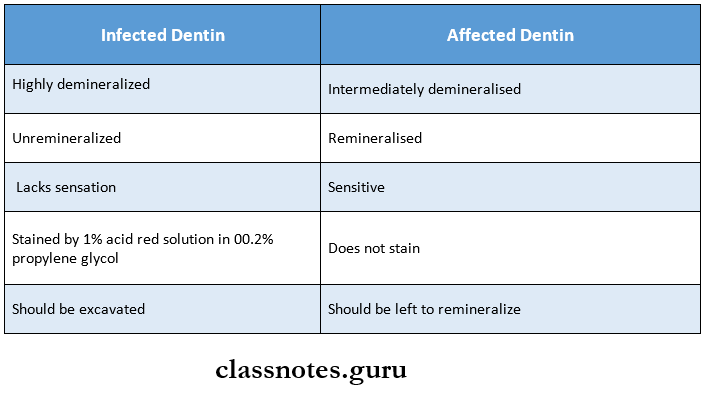
2. Infected v/s affected dentin
3. Lactose content of
- Breast milk – 7.2%
- Bovine milk – 4.5%
- Milk powder – 7%
4. Differences between nursing and rampant caries
5. Classification of early childhood caries
- Type 1 – Mild to moderate
- Caries in molars and incisors
- Seen in 2-5 years of age
- Type 2 – Moderate to severe
- Labiolingual caries with maxillary incisors with or without molars
- Seen soon after 1st tooth erupts
- Mandibular incisors unaffected
- Caused by inappropriate bottle feeding
- Type 3 – Severe
- Involve all teeth
- Seen in 3-5 years of age
Dental Caries Long Essays
Question 1. Define early childhood caries. Write notes on the window of infectivity, etiology, pathogenesis, clinical features, and management of early childhood caries.
Answer:
Definition: Davies defined early childhood caries as a Frequent bottle feeding at night complex disease involving maxillary incisors within a month after the eruption and spreading rapidly to other primary teeth
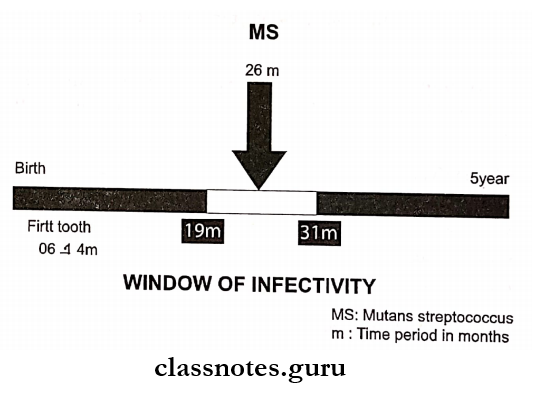
Window Of Infectivity:
- Introduced by Caufield
- He monitored levels of mutans S. in the oral cavity from birth to 5 years.
- As the deciduous teeth erupt, the oral cavity provides a natural habitat for the survival of MS/mutans strepto-coccus
- MS are the only organism present during this period
- It is limited to 7-31 months
- Later other organisms appear in the oral cavity
- This results in the competition of MS with other organisms
- Survival of MS becomes difficult
Etiology:
- Frequent consumption of liquids containing fermentable carbohydrates
- Poor feeding practices without appropriate preventive measures
- Frequent bottle feeding at night
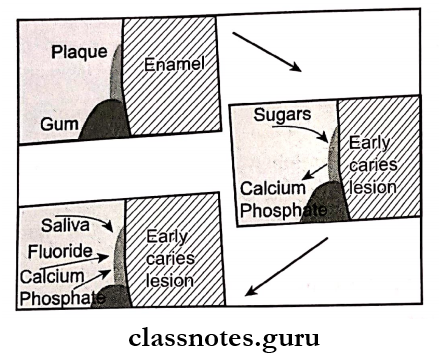
Pathogenesis:
Clinical Features Of Early Childhood Caries:
It occurs in the following stages
1. Very mild: Shows slight demineralization usually at the gingival crest and no cavitation
2. Mild: Show demineralization in a gingival third of the tooth and moderate cavitation
3. Moderate: Shows cavitation on multiple tooth surfaces
4. Severe:
- Consists of widespread destruction of tooth and partial to complete loss of the clinical crown
- Caries progresses from decalcification of upper primary incisors to primary molars and canines
Management:
1. Very mild cases:
- Preventive measures are undertaken to arrest the progression of the caries process
- It involves
- Diet counseling
- Oral hygiene measures
- Fluoride application
2. Mild cases:
Extensive and invasive treatment with multiple pulp therapies
3. Moderate and severe cases:
- Need pharmacological intervention
- Need multiple appointments and many local anesthetic injections to carry out pulp therapy and stainless steel crown
- Some teeth may need restorations while some others may need stainless steel crowns with or without pulp therapy
Question 2. Define rampant caries. Describe etiology, clinical features and management of it.
Answer:
Definition: It is an acute widespread caries with early pulpal involvement of teeth which are usually immune to decay
Rampant caries Etiology:
- Multifactorial in nature
- Excessive sticky carbohydrates
- Decreased salivary flow
- Hereditary
Rampant caries Clinical Features:
- It can be present at all ages
- Both dentitions is effected
- It involves all teeth including mandibular incisors
- Rapidly new lesions develop in addition to the present old lesions
- Carious tooth are with pulpal involvement
Rampant caries Management:
- Teeth affected require pulpal therapy
- Pulpotomy is carried out
Rampant caries Method:
- Anesthetize and isolate the tooth
- Remove the carious part
- The entire roof of the pulp chamber is removed
- With the help of a spoon or excavator cut out the coronal pulp
- Next, irrigate the pulp with water
- Control the bleeding with the help of moist cotton pellets
- Dry the pulp chamber
- Now, place cotton moistened with 1.5 concentration of Buckley’s formocresol
- Maintain it for 5 minutes
- Now remove it and dry the pulp chamber
- Restore it with a thick paste of ZOE
- A zinc polycarboxylate cement is placed over it
- Finally, restore with stainless steel crown
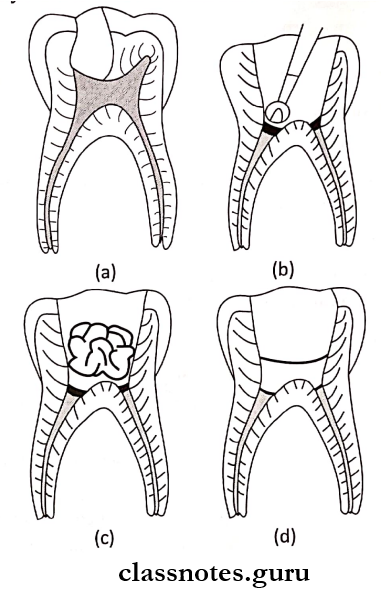
- (a) Cariously involved primary molar
- (b) Access cavity and removal of coronal pulp tissue
- (c) Placement of a cotton pellet moistened with formocresol
- (d) Pulp chamber filled with ZOE and crown is built up with glass ionomer before placement of stainless steel crown
Question 3. Define early childhood caries. Write about diet counseling and diet chart.
Answer:
Definition:
Davies defined early childhood caries as a complex dis-ease involving maxillary incisors within a month after the eruption and spreading rapidly to other primary teeth
Steps:
- Introduce diet diary
- 24-hour diet record is prepared
- A six days diet diary is advised
- Analyse complete records
- Isolating the sugar factors
- Patients education
- Consumption of sugar substitutes
Visits:
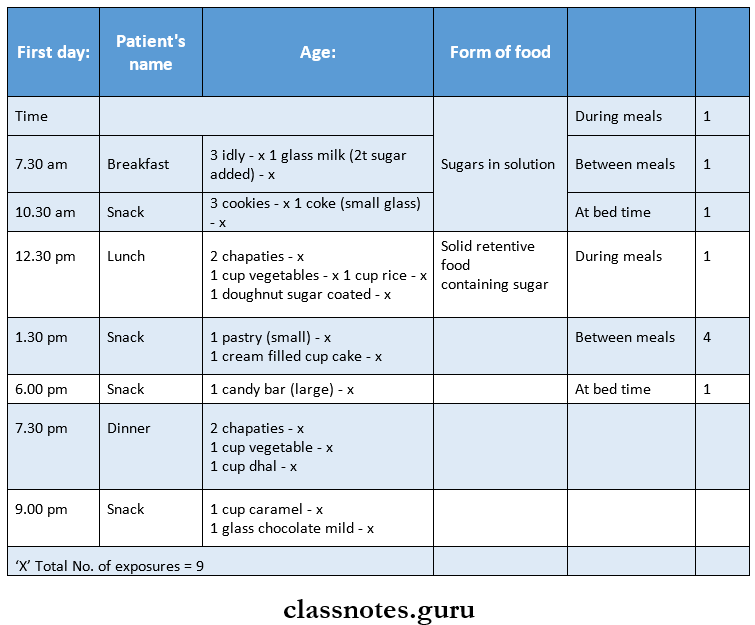
- First appointment:
- A diet diary of 6 consecutive days is prepared
- The form of particular food taken, its approximate amount along with snacks, candies, syrups, chewing gums consumption is recorded
- Identify the sugar-containing food items
- Mark such items with red Xs while others with blue Xs
- Explain the patient about the harmful effects of sugar-containing substances and explain to decrease the red Xs items while increasing blue Xs items
- Teach him as a game
- Suggest the sugar substitute like peanuts, walnuts
- Recall Visits:
- Recall appointments are carried out at regular intervals during the next months
- During these visits evaluate the patient’s progress and provide reinforcement
Dental Caries Short Essays
Question 1. Caries risk assessment.
Answer:
- Caries is a complex multifactorial disease
- Caries risk assessment is performed by doing a combination of the following analysis
1. Dietary analysis:
- The patient is asked for
- Quantity of sugar intake in the form of fermentable carbohydrates
- Frequency of intake
- Intake of acidic beverages
- It includes sports drinks, fruit juices, and soft drinks
- These provide energy to acidogenic and aciduric bacteria
- Frequency of snacking
2. Dental clinical analysis:
- The dental examination determines risk indicators and risk factors
- Risk indicators include:
- Visible cavitated caries lesion
- White spots on teeth
- Brown spots on teeth
- Risk factors include:
- Visible plaque or biofilm
- Exposed root surface
- Deep pits or grooves
- Prosthesis uses
- Poor quality of existing restorations
- Bacterial biofilm analysis:
- It helps to determine patient’s risk level
- It includes
- S. mutans count in saliva or plaque
- Lactobacilli count in saliva or plaque
- Adenosine triphosphate activity of the biofilm bacteria
- Risk indicators include:
3. Salivary analysis:
- It includes
- Salivary flow rate
- Salivary buffering capacity
- Salivary pH
Question 2. Caries susceptibility tests.
Answer:
1. Synder’s Test:
It is used for Lactobacillus count
Procedure:
- Paraffin-stimulated saliva is collected in test tubes
- It is inoculated into glucose and agar media
- pH 4.7-5.0 is maintain along with color indicator bromocresol green
- The color change indicates pH change and is compared to the standardized color chart and scored
- Recordings are carried out at the end of 24 hours, 48 hours, and 72 hours
Result:
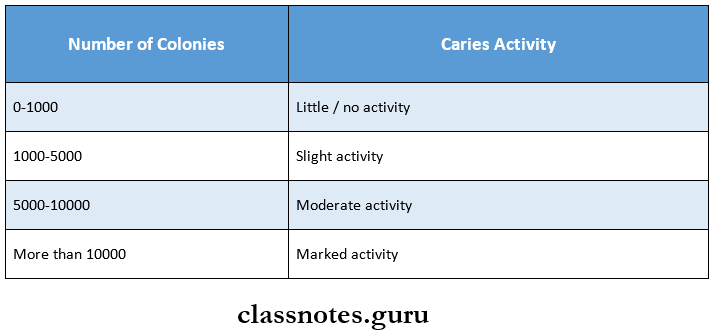
2. Lactobacillus Test:
- Described by Hadley in 1933
- Procedure:
- Collect paraffin-stimulated saliva (5-10 ml)
- Dilute to 1:10 dilution by pipetting 1 ml of saliva into 9 ml tube of sterile saline solution
- Similar again to 1:100 dilution using a 1:10 diluted sample
- Mix thoroughly
- Spread 0.4 ml of each dilution over agar plates
- Incubate for 3-4 days at 37° C
- Count the number of colonies
Result:
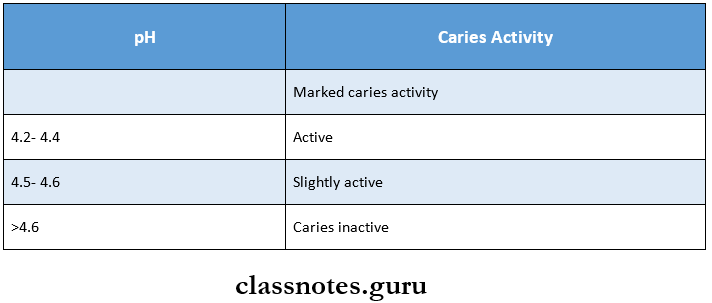
3. Swab Test:
- Procedure:
- The oral flora is sampled by swabbing the buccal surfaces of the teeth with a cotton applicator
- It is subsequently incubated in the medium
- The change in pH following a 48-hour incubation period is read on a pH meter
Interpretation:
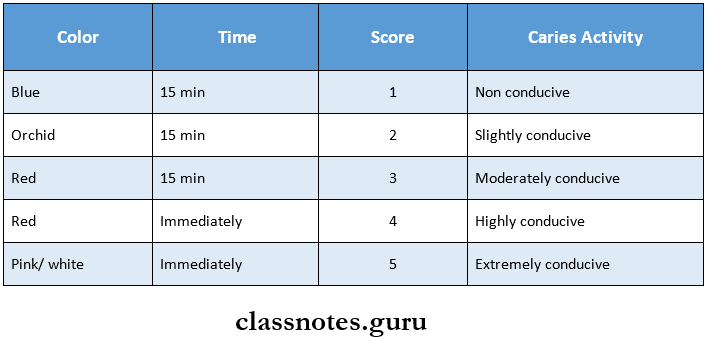
4. Salivary Reductase Test:
- Procedure:
- Paraffin-stimulated saliva is collected in a collection tube
- It is then mixed with the dye Diazo-resorcinol
- The caries conduciveness reading or color change is done after 15 minutes
- Resultt:
Question 3. Methods of Caries Detection.
Answer:
Visual Examination:
- It compresses the detection of white spot
- Discoloration or cavitation
Tactile Examination:
- Usually, explorer is used for occlusal caries
- Findings
- Softness at the base
- Catch by an explorer
- Tug back or resistance to removal
Use Of Floss:
- Used for proximal caries or with patients complaining of food lodgement between the teeth
- Passing the floss through carious lesion results in fray-ing of it
Radiographs:
- A radiograph detects the carious lesion as a radiolucent area
- Its extent depicts the extent of caries
Caries Detection Advances:
- Digital Radiography
- Xeroradiography
Fiber Optic Transillumination:
- It is based on the difference in the transmission of light for decayed and sound tooth
- An area of decay shows darkened shadow as compared to sound tooth.
Ultrasonics:
- It is based on the use of sound waves
- Echo produced are of the different amplitude of both normal and decayed tooth
- A decayed tooth produces an echo of higher amplitude
Dyes:
- Different dyes are used for the detection of caries
- Ex. Calcein – for enamel caries
- Fuschin – for dentin caries
- Layers of dentin can also be differentiated as basic fuschin stains that only infected dentin and not affected one
Question 4. Strip Mutans Test – By Jenssen and Bratthal.
Answer:
- It is used to count the presence of streptococcus mutans in the oral cavity
- Streptococcus mutans can be considered as an indicator of caries activity
- But as caries is a multifactorial disease, this test gives only a relative information
- Patients with streptococcus mutans in their oral cavity may show no sign of caries
- While the patient with caries lesion may not have any number of streptococcus mutans
Principle:
It is based on the fact that bacitracin inhibits the growth of all other oral streptococci except mutans on the mitis salivary medium
Uses:
- Patient selection
- Evaluates the effect of mouth rinses
- Helpful in health education
- Patient as well as parents education
Question 5. Nursing bottle Caries.
Answer:
Nursing bottle Caries Definition:
- Caries caused by a prolonged use of a bottle filled with any liquid other than the water
Nursing bottle Caries Etiology:
- Bovine milk, milk formulas
- Sweeteners like honey-dipped pacifiers
- Micro-organisms like Streptococcus mutans
- Fermentable carbohydrates
- Hypoplasia of teeth
- Decreased salivary flow
- Malnutrition
Nursing bottle Caries Clinical Features:
- All teeth except the mandibular anterior are affected.
- This is because of the position of the tongue that man¬dibular interiors are spared.
- Initially, caries appear as a dull, white area along the gingival margin.
- This progresses to the cervical margin to form a ring-like lesion.
- Finally, whole crown of the tooth is destroyed.
Nursing bottle Caries Treatment:
- First visit:
- Excavate and restore all carious lesions
- Pulp therapy is done if required
- Drainage of abscess
- Topical fluoride application
- Second visit:
- Diet counseling
- Evaluating the restoration and if required re-restoration done
- Third visit:
- Endodontic treatment
- Extraction of unrestorable teeth
- Recall the patient after every 3 months
Question 6. Role of Diet in Dental Caries/Nutrition and Dental Caries.
Answer:
The presence of fermentable carbohydrates results in loss of caries immunity
Factors Responsible For It:
- Frequency of intake of carbohydrate
- Physical and chemical forms of it
- Route of administration
- Presence of other food constituents
Various Dietary Studies:
- Vipeholm study by Gustafsson et.al in 1959
- Hopewood House study by Sullivan in 1958
- Turku Sugar study by Scheinin in 1975
- Seventh-day Adventist Children Study
- Hereditary Fructose Intolerance
Results:
- An increase in carbohydrates increased the level of dental caries
- The risk of caries is greater for sticky food
- The risk of caries is greater if sugar is consumed between meals
- Monosaccharides and disaccharides are more harmful than polysaccharides
- Frequent use of xylitol in between meals produces an anti-cariogenic effect
- Caries activity varies between individuals
- Caries incidence increases with increased frequency of intake of carbohydrate
- Other dietary constituents like vitamin A, D, K, B complex, calcium, fluoride, etc. has an inhibitory effect on dental caries.
Question 7. Steps in diet counseling
Answer:
Diet counseling Steps:
- Introduce diet diary
- 24-hour diet record is prepared
- A six days diet diary is advised
- Analyse complete records
- Isolating the sugar factors
- Patients education
- Consumption of sugar substitutes
Diet counseling Visits:
- First appointment:
- A diet diary of 6 consecutive days is prepared
- Form of particular food taken, its approximate amount along with snacks, candies, syrups, chewing gums consumption is recorded
- Identify the sugar-containing food items
- Mark such items with red Xs while others with blue Xs
- Explain the patient the harmful effects of sugar-containing substances and explain to decrease the red Xs items while increasing blue Xs items
- Teach him as a game
- Suggest the sugar substitute like peanuts, walnuts
- Recall Visits
- Recall appointments are carried out at regular intervals during the next months
- During these visits evaluate the patient’s progress and provide reinforcement
Question 8. Affected vs infected dentin
Answer:
Infected Dentin
- Irreversible denatured collagen
- Infiltrated with bacteria
- Not remineralize
- Should be removed
- Darker
- Softer
- Lacks sensation
- Indistinct cross bands
- Stained with:
- 0.2% propylene glycol
- 10% acid red solution
- 0.5% basic Fuschia
Affected Dentin
- Reversible denatured collagen
- Not infiltrated
- Remineralize
- Left behind while cavity preparation
- Lighter
- Harder
- It is sensitive
- Distinct cross bands
- Cannot be stained with any solution
Dental Caries Short Answers
Question 1. Stephen’s curve.
Answer:
- Within 2-4 minutes of rinsing with a solution of glucose or sucrose, plaque pH is reduced from about 6.5 to 5 and gradually returns to its original value within 40 minutes
- This when graphically plotted is the curve called as Stephan curve
Question 2. Caries tetralogy.
Answer:
Caries tetralogy consists of
1. Tooth:
- Composition:
- Highly mineralized-less caries formation
- High solubility leads to more caries formation
- Increased permeability of enamel surfaces causes increased caries
- An increase in mineral content leads to increased resistance to caries
- Morphology:
- The presence of deep, narrow, and retentive pits and fissures leads to high caries incidence
- Position:
- Malaligned, rotated teeth are more prone to caries due to more plaque accumulation
2. Saliva:
- pH:
- A rise in pH neutralizes acid attacks on the tooth surface during caries progression
- Composition:
- Bicarbonate ions- cause neutralization
- Ammonia- causes rise in pH
- Quantity:
- Reduction of saliva leads to
- Rampant caries
- Exacerbation of aeries
- Viscosity:
- Extremely viscous saliva leads to caries-free mouth
- Abundant, thin, watery saliva exhibit ram¬pant caries
- Antibacterial properties:
- Lysozyme- lyses cariogenic and non-cariogenic bacteria
- Salivary peroxidase- inactivates bacterial enzymes
- Immunoglobulin- IgA protects against caries
3. Diet:
- Fibrous food
- Keep teeth clean
- Stimulates salivary flow
- Reduces caries incidence
- Soft and sticky food increases caries incidence
- Dietary constituents that reduce incidence of car¬ies are
- Phosphates
- Traces of molybdenum and vanadium
- Vegetables
- Vitamins
- Minerals
- Fats
4. Saliva:
- Under normal conditions, the saliva is supersaturated in terms of calcium and phosphorous with respect to the enamel surface
- This prevents the hydroxyapatite from dissolving in the oral environment
Question 3. Pre-eruptive caries.
Answer:
- Occasionally, defects on the crowns of developing permanent teeth are evident radiographically even though no infection of the primary tooth or the surrounding area is apparent
- Muhler referred to this condition as pre-eruptive caries
- Such a lesion often does resemble caries when it is observed clinically and the destructive lesion progresses if it is not restored
- As soon as the lesion is reasonably accessible, the tooth should be uncovered by removal of the overlying primary tooth or by surgical exposure
- The caries-like dentine is then excavated and the tooth is restored with a durable temporary or permanent restorative material
- In some cases, the lesion may be so extensive that indi¬rect pulp therapy is justified
Question 4. Hopewood House Study.
Answer:
- By Sullivan in 1958
- This study was conducted among children between 3 and 14 years of age residing at Hopewood House for longitudinally 10 years.
Hopewood House Study Features:
- Absence of meat
- Rigid restriction of refined carbohydrate
Hopewood House Study Results:
- 53% of children at Hopewood House were caries-free
- 0.4% children of state were caries-free
- 75% of children had gingivitis and poor oral hygiene.
Question 5. Critical pH.
Answer:
- It represents the demineralization-remineralization cycle
- At critical pH of 5.5 or below
- Hydrogen ions (H+] react with the phosphate group present in the oral cavity
- Results in the formation of hypophosphate
- Due to this, hydroxyapatite crystals dissolve and is termed as demineralization
- At neutral pH
- With the adequate presence of Calcium and phosphorus, dissolution is inhibited
Question 6. DMFI Index.
Answer:
- Used for measuring dental caries
- D – Decayed
- Indicates the number of permanent teeth that are decayed
- M – Missing
- Indicates the number of missing permanent teeth due to decay
- F – Filled
- Indicates the number of permanent teeth that have been attacked by caries due to which have been re¬stored
DMFI Calculation:
Total DMFT = D+M+F
Question 7. Incipient Caries.
Answer:
- Early carious lesions present on smooth surfaces
- It is seen as a ‘white spot’
- Only sub-surface demineralization is involved
- It cannot be diagnosed radiographically
- However, it can be diagnosed with DIAGNOdent
- It should be differentiated from the developmental effects of enamel formation
- On wetting, the carious lesion disappears
Question 8. Alban’s test
Answer:
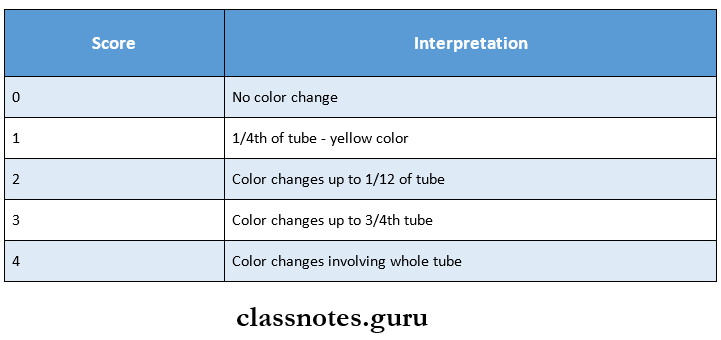
Alban’s test Procedure:
- A 5 ml of agar is removed from the refrigerator but not heated
- Unstimulated saliva is added to it
- The tube is then incubated for 4 days and color change is noted
- Color changes are scored 0 to 4
Alban’s test Result:
- 0- Indicates no color change
- 1- The color changes to yellow in the top l/4th of the tube
- 2 – Color changes to half of the tube
- 3 – Color changes to 3/4th of tube
- 4 – The entire length of the agar has changed to yellow
Dental Caries Viva Voce
- The critical pH at which demineralization starts is about 5.2 to 5.5
- Caries triad involves the tooth, microflora, and a suit-able local substrate
- Caries tetralogy includes a fourth-factor time
- Trace elements like selenium, cadmium, lead, and barium have been found to increase the caries experience