
Pediatric Consideration For Oral Surgery Important Notes
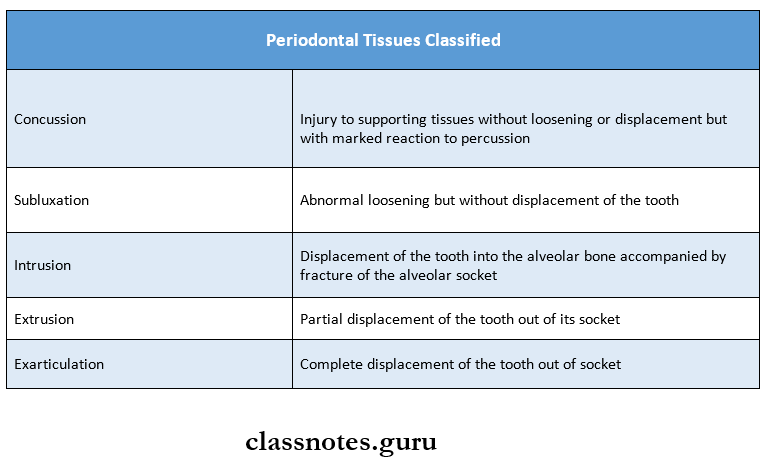
1. Injuries to the periodontal tissues are classified as:
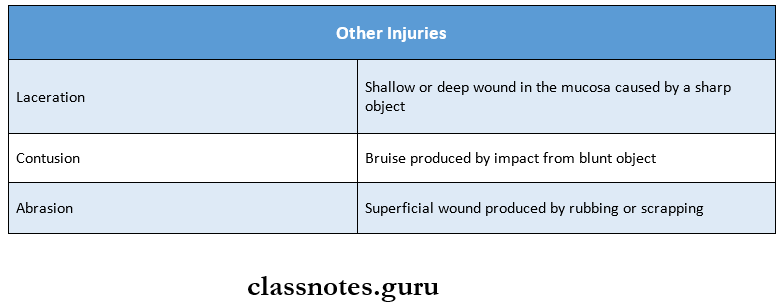
2. Other injuries
3. Sequel of trauma to a tooth
- Internal hemorrhage
- Hyperaemia
- Internal resorption
- Pulpal necrosis
- Canal calcifications
Read And Learn More: Pedodontics Short Essays Question And Answers
4. Balanced Hank’s solution (HBSS)
- It is one of the media for preserving the avulsed tooth
- It is an isotonic salt solution
- Available as a “SAVE A TOOTH” solution
5. Drugs
- The safe dose of local anesthesia in a child
- With adrenaline – 7 mg/kg body weight
- Without adrenaline – 4.5 mg/kg body weight
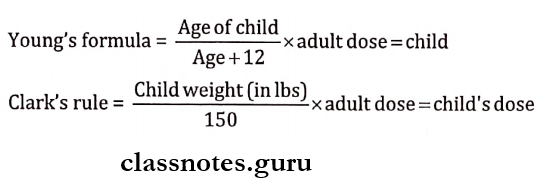
6. Drug dosage
Pediatric Consideration For Oral Surgery Long Essays
Question 1. Classify traumatic injuries. Write in detail about the management of Ellis Class 3 fracture of the maxillary right central incisor.
(or)
A 7-year-old child reported trauma on the central incisor. Explain the investigation and treatment options based on the diagnosis.
(or)
Classify traumatic injuries to teeth and supporting structures. Explain Ellis Class 3 in detail
Answer:
Traumatic Injuries Classification:
1. Ellis Classification:
- Class 1 – Simple crown fracture involving enamel
- Class 2 – Crown fracture involving enamel and dentin
- Class 3 – Crown fracture involving enamel, dentin, and pulp
- Class 4 – Nonvital tooth due to trauma with or without loss of crown structure
- Class 5 – Teeth lost due to trauma
- Class 6 – Root fracture
- Class 7 – Displacement of a tooth without fracture
- Class 8 – Fracture of crown en masse and its replacement
- Class 9 – Traumatic injuries to primary teeth
2. WHO Classification:
1. Injuries to the Hard Dental Tissues and Pulp:
- Crown infraction
- Uncomplicated crown fracture
- Complicated crown fracture
- Uncomplicated crown root fracture
- Complicated crown root fracture
- Root fracture
2. Injuries to the Periodontal tissues:
- Concussion
- Subluxation
- Intrusive luxation
- Extrusive luxation
- Lateral luxation
- Exarticulation
3. Injuries of the Supporting Bone:
- Comminution of alveolar socket
- Fracture of the alveolar socket wall+
- Fracture of the alveolar process
- Fracture of the mandible and maxilla
4. Injuries to Gingiva or oral mucosa:
- Laceration
- Contusion
- Abrasion
Management Of Ellis Class 3 Fracture:
Assess the extent of the injury
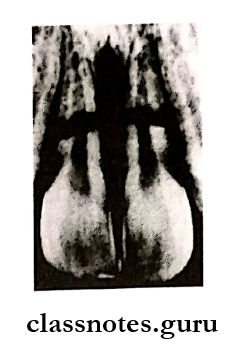
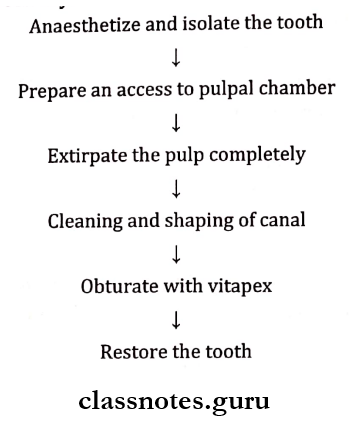
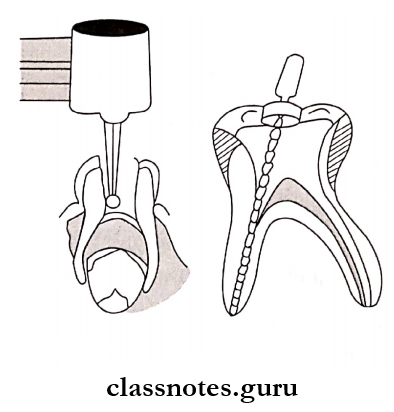
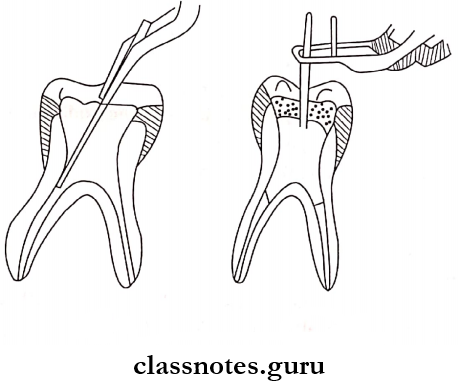
1. Pulpectomy:
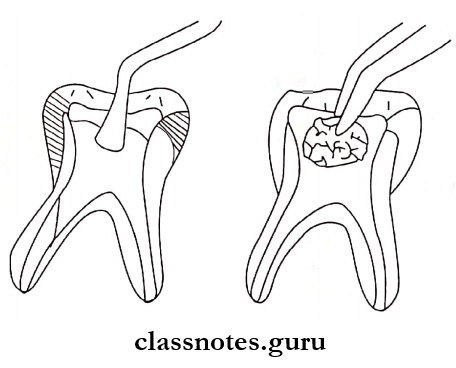
2. Extraction of tooth:
In the presence of periapical pathology
Question 2. Classify traumatic injuries and describe in detail about the management of Ellis class 2 fracture injuries.
Answer:
Ellis class 2 fracture Class 2 Fracture:
It is a fracture of the crown involving enamel and dentin without pulp exposure
Ellis class 2 fracture Management
- Thorough cleanse the area
- Examine the fractured teeth
- Assess the extent of exposed dentin
- Place calcium hydroxide on the exposed dentin
- Restore the tooth with a temporary restoration
- Wait for the reattachment of the crown fragment
- Once it is achieved, restore with a permanent restoration like composite resin or full coverage crown
Pediatric Consideration For Oral Surgery Short Essays
Question 1. Root Fracture.
Answer:
Root fractures are relatively uncommon in permanent dentition
Root Fracture Diagnosis:
- Clinical examination reveals a slightly extruded tooth often displaced lingually
- Radiographs will show a rot fracture on the proper angulation of the X-ray beam
Management Of Root Fracture:
- Determine the position of fracture radiographically
- If the fracture is present in the apical third no treatment is required
- It resorbs on its own
- Fractures involving the middle third of the root are extracted
- Fractures that communicate with the gingival margin are extracted
- While extraction, avoid damage to the underlying tooth germ
Question 2. Mucocele.
Answer:
It is an extravasation type of cyst
Mucocele Cause: Trauma to the minor salivary gland
Mucocele Features:
- Superficial lesion – small, raised, bluish
- Deep-seated lesions – small but diffuse, covered by normal mucosal color
- The lower lip is commonly affected.
Mucocele Treatment: Excision of the lesion
Question 3. Luxation Injuries and their Management.
Answer:
Luxation Injuries:
- This leads to the displacement of teeth
- It can be
- Intrusive
- Extrusive
- Lateral
Luxation Injuries Management:
1. Mild injury:
- No occlusal interference
- The child is kept on soft diet
- Maintain oral hygiene
2. Palatally luxated teeth: Teeth is positioned palatally manually and splinted
3. No improvement present: Extract the tooth
4. Buccally luxated teeth: Extract the teeth
Question 4. Anesthetic preparation of Child.
Answer:
- Patients should be told about the procedure in a less threatening manner
- The instrument tray should be kept behind the chair, away from the sight of the patient
- The needle should be hidden with a finger
- Explain to the child the sensation of pinching that is experienced after an LA injection
- Explain to the child the difference between pressure and pain
- Explain the sensation of numbness
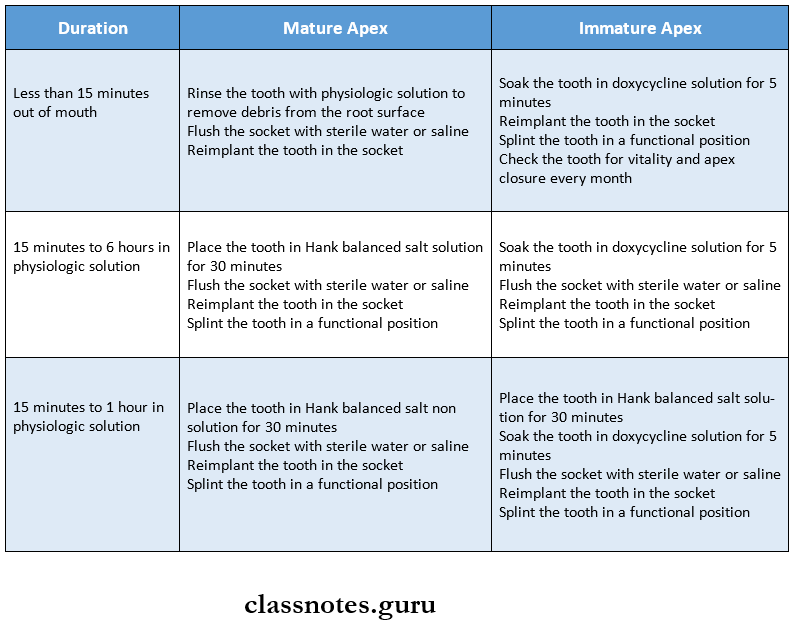
Question 5. Treatment of avulsion of permanent teeth.
Answer:
Question 6. Inferior alveolar nerve block in children.
Answer:
- When deep operative or surgical procedures are undertaken for the mandibular primary or permanent teeth, the inferior alveolar nerve must be blocked
- The mandibular foramen is situated at a level lower than the occlusal plane of the primary teeth of the pediatric patient
- Therefore, the injection must be made slightly lower and more posteriorly than for an adult patient
Inferior alveolar nerve block Technique:
- The thumb is laid on the occlusal surface of the molars with the tip of the thumb resting on the internal oblique ridge and the ball of the thumb resting on the retromolar fossa
- The ball of the middle finger is rested on the posterior border of the mandible for firm support
- The Barrel of the syringe is directed between the two primary molars on the opposite side of the arch
- Inject the solution
- Depth of insertion- about 15 mm
- Solution deposited-1 ml approx
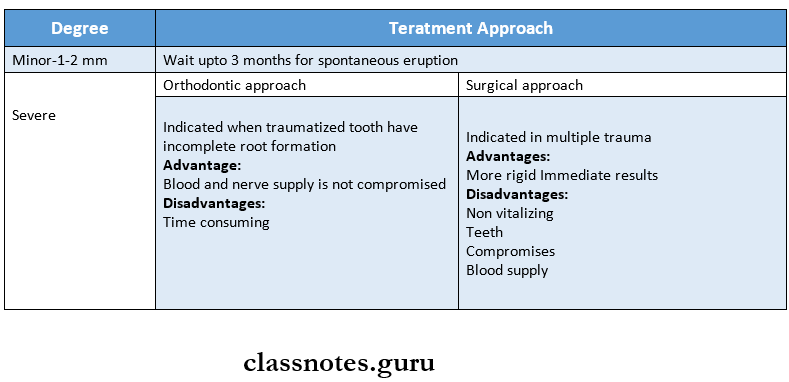
Question 7. Treatment of intrusion of the permanent central incisor
Answer:
Management of intrusion depends on the degree of intrusion which has been taken place
- After the desired approach is carried out, suture the gingival laceration
- Splint for 2-3 weeks after the tooth has come to normal position
- Soft diet for 14 days
- Follow-up period of 1 year
Question 8. Local anesthetic drug delivery systems.
Answer:
- Local infiltration
- LA is deposited near small nerve endings
- Field block
- LA is deposited near a large branch of peripheral nerve
- Nerve block
- LA is deposited near the main trunk
- Intraligamentary
- Most commonly used for single tooth o LA needs to be given under high pressure
- Intraseptal
- Used to reinforce analgesia produced by infiltration
- Used for mandibular primary molars
- Intrapapillary
- Produces analgesia of palatal/ lingual tissues
- Intrapulpal
- Used in pulp therapy
Pediatric Consideration For Oral Surgery Short Question And Answers
Question 1. Inferior Alveolar Nerve Block.
Answer:
- Move your finger over mesiobuccal fold up to the coronoid process of the mandible
- Feel the pterygomandibular depression
- Insert a syringe with a 15/8 inch 25 gauge needle parallel to the occlusal plane of the mandibular teeth
- Penetrate tissues of pterygomandibular depression
- Aspirate
- Slowly deposit 1-1.8 ml of solution
Question 2. Topical Anaesthesia.
Answer:
- It is anesthesia that is obtained by the application of a suitable agent to an area of either skin or mucous membrane.
- Topical Anaesthesia Methods:
- Spraying the area with 10% lignocaine hydrochloride
- Ointments containing 5% lignocaine hydrochloride and emulsions containing 2% lignocaine hydrochlo¬ride are used
Question 3. Antibiotics in Pediatric Dentistry.
Answer:
- Penicillin: Amoxycillin – 20 – 40 mg/kg/day
- Cephalosporin: Cephalexin – 50 – 100 mg/kg/day
- Macrolides: Erythromycin – 30 – 50 mg/kg/day
- Metronidazole: 5 mg/kg TID
Question 4. Composition of LA solution.
Answer:
- Local anesthetic- ester or amide
- Vasoconstrictor- Epinephrine
- Anti-oxidant- Sodium metabisulphite
- Preservative- Methylparaben
- Fungicide- Thymol
- Salt- Sodium chloride
- Vehicle- Distilled water or Ringer’s lactate solution
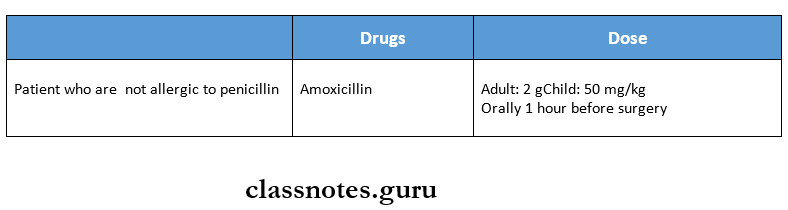
Question 5. Antibiotic prophylaxis for endocarditis.
Answer:
Question 6. Mouth guards.
Answer:
- American Dental Association and the Academy for Sports Dentistry recommend properly fitted mouth guards for a variety of sports and recreational activities which predispose the participants to oral injuries
- Mouth guards are designed to protect the lips and intraoral soft tissues from bruises and lacerations
- They also protect the teeth from any kind of fractures or luxation injuries and the jaws from any dislocation and fractures
Mouthguards Classification:
- Type 1- Stock mouthguards
- Type 2- Mouth-formed mouthguards
- Type 3- Custom fabricated mouthguards
Mouth guards Other forms:
- Jaw joint positioner
- Anatomically designed mouthguard
Question 7. Non-accidental injury.
Answer:
- Nonaccidental injuries are nothing but child abuse and neglect
- These are not accidental injuries but they are inflicted by people who are responsible for the care of the child
- The child is considered to be abused if they are treated in a way that is unacceptable in a given culture
Question 8. Drugs used for conscious sedation.
Answer:
Various agents used for conscious sedation are
1. Inhalation: Nitrous oxide
2. Oral route:
- Hydroxyzine oral or IM- 0.6 mg/kg and 1.1 mg/kg
- Promethazine- oral/IM- 0.5 mg/kg and 1.1 mg/kg
- Diazepam- oral 0.2-0.5 mg/kg, rectal 0.25 mg/kg
3. Intramuscular:
- Ketamine- IM/IV-1-5 mg/kg
- Midazolam- oral – 0.25-1 mg/kg, IM 1-1.15 mg/kg
4. Intravenous: Midazolam
Question 9. Eruption hematoma
Answer:
- It is also known as an eruption cyst
- It is a dentigerous cyst occurring in the soft tissues
- Eruption hematoma Clinical Features
- Occurs more frequently and ruptures spontaneously
- Seen in children of different ages
- Deciduous and permanent teeth may be involved
- Common in anterior and first permanent molar
- The lesion appears circumscribed, fluctuant, often translucent swelling of the alveolar ridge over the site of the erupting tooth
Pediatric Consideration For Oral Surgery Viva Voce
- Re-eruption potential is high in young permanent teeth
- Partially intruded primary teeth should be left undisturbed as they usually re-erupt naturally
- Luxation injuries are more common in the first 3 years of life
- Fractures occurring in the apical third have the best prognosis
- Isotonic saline/ pasteurized whole bovine milk are favorable storage media
- If an intruded tooth is found to be impinging on permanent tooth bud, extraction of a tooth is indicated
- Water is hypotonic media
- If the tooth is not reimplanted immediately in a dental office, HBSS is the best storage media
- If more than 1 hour is the extra-oral dry time, the avulsed tooth should be immersed in 2% sodium fluoride solution for 20 minutes