
Orbital Cavity Definition
Orbits are two bony sockets which lodge the eyeballs and the associated structures.
Orbital Cavity Shape And Parts
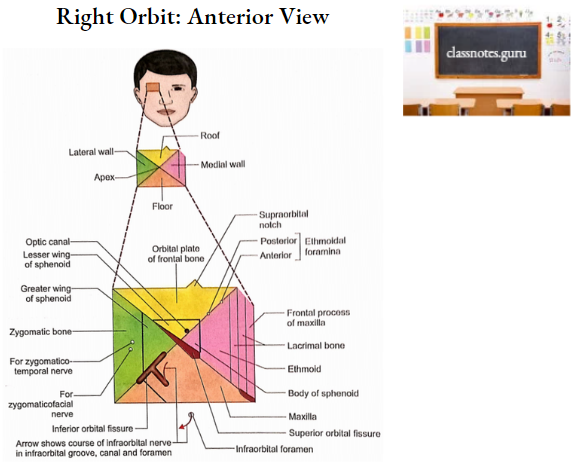
Each orbit is pyramidal in shape having an anterior base (orbital opening), posterior apex and four walls (medial, lateral, roof and floor).
Orbital Cavity Bony Contributions
- Orbital Opening (Base)
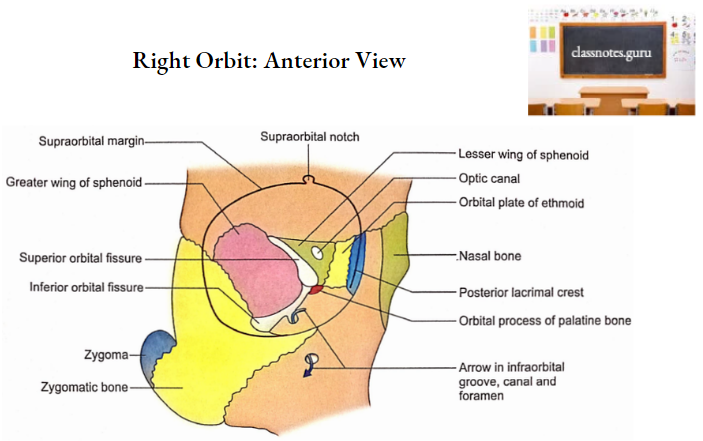
It consists of four margins (supraorbital, infraorbital, lateral and medial).
- Supraorbital Margin
- It is formed by the frontal bone.
- The supraorbital notch (or foramen) is situated at the junction of its medial 1/3rd. (rounded) and lateral 2/3rd (sharp) parts.
- Supraorbital notch transmits:
- Supraorbital nerve.
- Supraorbital artery.
- Communicating veins between angular and superior ophthalmic veins.
- Infraorbital Margin
- It is formed by maxilla medially and zygomatic bone laterally.
- Lateral orbital margin
- It is formed by the frontal process of the zygomatic bone below and the zygomatic process of the frontal bone above.
- Medial Orbital Margin
- It is formed by the frontal bone above and the lacrimal crest of the frontal process of the maxilla below.
- Supraorbital Margin
- Apex
- It forms the posterior end of the orbit.
- It is contributed by sphenoid.
- Usually, the medial end of the superior orbital fissure is said to mark the apex.
- Medial Wall
- It is formed by the following bones from anterior to posterior:
- Posterior part of the frontal process of the maxilla.
- Lacrimal bone.
- The orbital plate of ethmoid.
- Body of sphenoid.
- It is formed by the following bones from anterior to posterior:
- Lateral Wall
- It is contributed by:
- Greater wing of sphenoid bone posteriorly.
- Orbital surface of the zygomatic bone and medial aspect of its frontal process anteriorly.
- It is contributed by:
- Roof
- It is formed by:
- Orbital plate of frontal bone anteriorly.
- Lesser wing of sphenoid posteriorly.
- It is formed by:
- Floor
- It is formed by:
- Orbital surface of maxilla medially. It is the major contribution.
- Orbital surface of the zygomatic bone.
- Orbital process of the palatine bone. It is an insignificant contribution near the posterior end at the junction of the medial wall and floor.
- It is formed by:
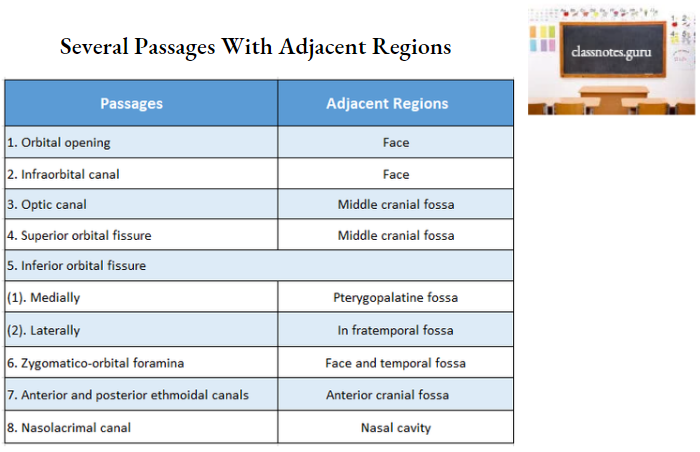
Orbital Cavity Communications
The orbit communicates through several passages with adjacent regions as shown
below.
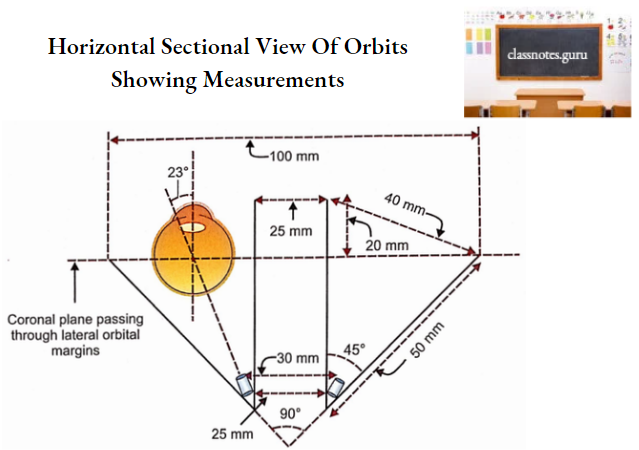
Orbital Cavity Measurements
- Length of medial wall – 50 mm.
- Length of lateral wall – 50 mm.
- Width of orbital opening, i.e. the distance between medial and lateral orbital margins – 40 mm.
- Distance between two lateral orbital margins – 100 mm.
- Distance between two medial orbital margins – 25 mm.
- The angle between two lateral walls – 90°.
- The angle between the lateral and medial walls of each orbit is – 45°.
- The angle between the long axis of the orbit and the anteroposterior axis of the eyeball – 23.
- Distance between medial orbital margin and coronal plane passing through lateral orbital margins – 20 mm.
- Measurements of the optic canal:
- Length – 3 – 9 mm.
- Diameter – 5 mm.
- Distance between orbital openings of optic canals – 30 mm.
- Distance between cranial openings of optic canals – 25 mm.
Orbital Cavity Features
1. The anterolateral part of the roof is slightly hollowed out to form a fossa for the lacrimal gland.
2. The anteromedial part of the roof near the orbital opening is marked by the trochlear fovea or spine for the attachment of a fibrocartilaginous pulley meant for the tendon of the superior oblique muscle.
3. The optic canal is present at the posterior end of the junction of the roof and medial wall. The optic nerve and ophthalmic artery pass through the optic canal.
4. The posterior part of the junction of the lateral wall and floor is marked by an inferior orbital fissure. It transmits the following structures:
- Maxillary nerve.
- Infraorbital vessels.
- Zygomatic nerve.
- A branch from an inferior ophthalmic vein.
- Some twigs (orbital branches) from the pterygopalatine ganglion.
Boundaries of the inferior orbital fissure are as follows:
- Superiorly – Greater wing of sphenoid.
- Inferiorly – Body of maxilla and orbital process of palatine bone
- Laterally Zygomatic bone.
5. The maxillary part of the floor is marked by a groove (infraorbital groove) in the posterior part.
- This groove is directed forward and continues with the infraorbital canal in the anterior part of the floor and ultimately opens on the face as an infraorbital foramen.
- The infraorbital groove, canal and foramen are meant for the passage of infraorbital nerve and vessels.
6. In the anterior part of the medial wall, the posterior part of the frontal process of the maxilla (behind the anterior lacrimal crest).
- Anterior part of lacrimal bone (anterior to posterior lacrimal crest) form a vertical fossa called lacrimal fossa.
- This fossa continues down with the beginning of the nasolacrimal canal. The fossa and canal are meant for the lacrimal sac and nasolacrimal duct respectively.
7. Anterior lacrimal crest provides attachments to:
- Lacrimal fascia.
- Medial palpebral ligament.
- Orbicularis oculi.
8. Posterior lacrimal crest gives attachments to:
- Lacrimal fascia.
- Lacrimal part of orbicularis occuli.
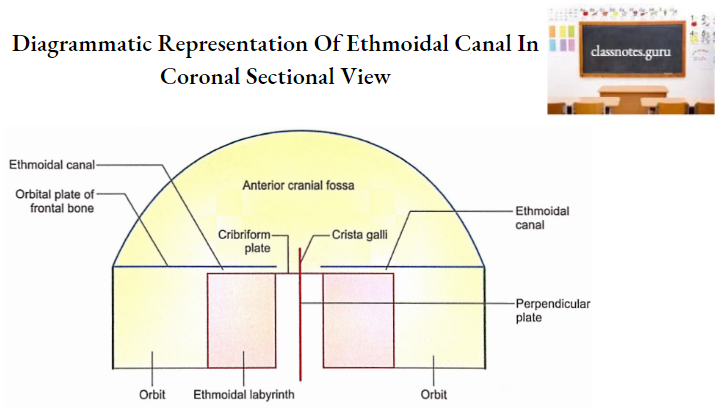
9. The junction of the orbital plate of the frontal bone (roof) and an orbital plate of the ethmoid (medial wall) shows two openings which lead into anterior and posterior ethmoidal canals. These transmit corresponding ethmoidal nerves and vessels.
10. The orbital surface of the zygomatic bone in the lateral wall possesses zygomatic-orbital foramina meant for the passage of zygomaticotemporal and zygomaticofacial nerves and zygomatic branches of the lacrimal artery.
11. Superior Orbital Fissure
- Location
- It is located at the junction of the roof and lateral wall of the orbit.
- Shape
- It is triangular in shape with a base medially and apex laterally.
- Communication
- It connects the orbit with the middle cranial fossa.
- Boundaries
- Medial: Body of sphenoid bone.
- Apex: Frontal bone.
- Superior: Lesser wing of sphenoid.
- Inferior: Greater wing of sphenoid.
- Common annular tendon
- The lower margin of the fissure presents a bony projection for the attachment of the common tendinous ring (common annular tendon) for the attachment of the recti of the eyeball.
- Structures passing through
- The common annular tendon divides the fissure into three compartments for the passage of a number of structures as shown below.
- Lateral part
- Lacrimal nerve.
- Frontal nerve.
- Trochlear nerve.
- Superior ophthalmic vein.
- Meningeal branch of the lacrimal artery.
- Orbital branch of the middle meningeal artery.
- Part within the tendinous ring
- Upper and lower divisions of the oculomotor nerve.
- Nasociliary nerve.
- Abducent nerve.
- The part below the tendinous ring
- Inferior ophthalmic vein
- Sympathetic twigs.
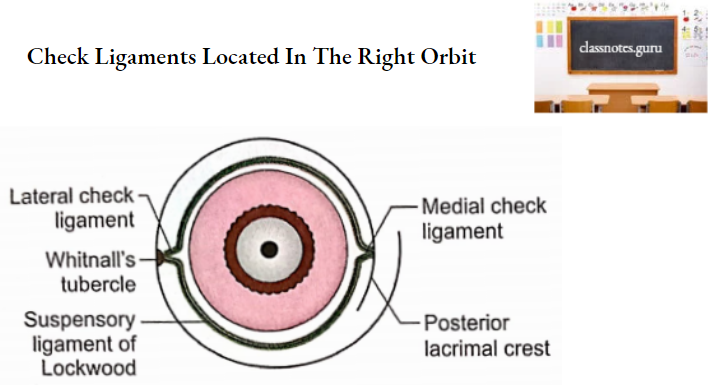
12. The lateral wall of the orbit near the lateral orbital margin presents an ill-defined Whitnall’s tubercle.
- It is located on the orbital surface of the frontal process of the zygomatic bone about 1 cm below the frontozygomatic suture.
- The following structures are attached to this tubercle:
- Lateral palapebral ligament.
- Lateral check ligament.
- Suspensory ligament of the eyeball.
- Aponeurosis of levator palpebrae superioris.
Orbital Cavity Applied Anatomy
1. Maxillectomy should be performed below the attachments of check ligaments to avoid the sagging of the eyeball.
2. A normal amount of orbital fat stabilizes the eyeball from behind. An increase in the orbital fat as observed in hyperthyroidism, will push the eyeball forward leading to exophthalmos (bulging of the eye).
3. The floor and medial wall of the orbit are relatively thin therefore tumours arising from ethmoidal and maxillary sinuses may push into the orbital cavity and displace the eyeball.
4. In Graves’ disease there is hypertrophy of extraocular muscles which is responsible for increased intraorbital pressure and exophthalmos.
5. Eyeball occupies the anterior half of the orbit and it is joined by the optic nerve from behind. The optic nerve runs a tortuous course to allow the movements of the eyeball without being damaged. Inflammation of the optic nerve is called retrobulbar neuritis.
6. There may be an isolated fracture of a single orbital margin or wall or there can be involvement of multiple margins or walls in different combinations.
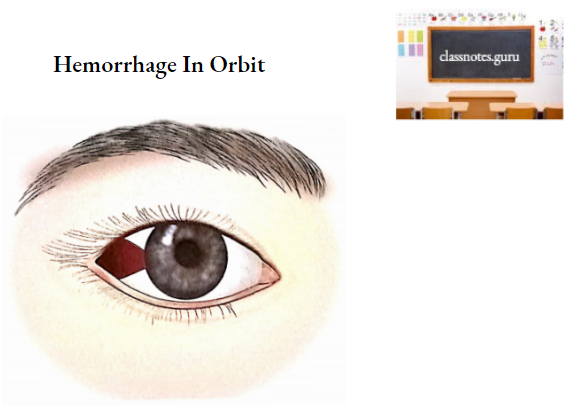
7. Fracture of the orbital plate of the frontal bone causes haemorrhage into the orbit. The haemorrhage acquires a triangular shape under the conjunctiva whose apex is towards the corneoscleral junction and base towards the orbital margin.
8. A severe impact on the nasal bridge may involve the medial wall of the orbit. The involvement of the lacrimal bone will damage the lacrimal passage.
9. A fracture of the sphenoid may lacerate the optic nerve in the optic canal resulting in blindness.
10. Frontozygomatic suture located in the lateral orbital margin forms an important landmark in the treatment of maxillofacial injuries.
11. Fracture of the frontal process of the zygomatic bone may occur in conjunction with a comminuted fracture of the orbital rim and frontal bone.
12. Orbit is an anatomical region which is of great clinical and surgical interest due to many disciplines in its surrounding relations.
13. The floor of the orbit is very thin and further weakened by the presence of an infraorbital groove. A fracture which is common in this part, invariably involves the infraorbital nerve and vessels.
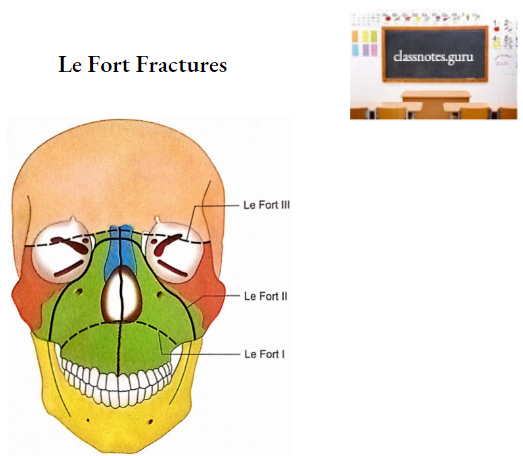
14. Le Fort (2 and 3) fractures of the midfacial skeleton involve the walls of the orbit. The fracture line in the case of Le Fort 2 fracture crosses the lower part of the frontal process of the maxilla and lacrimal bone. In Lé Fort 3 fracture both medial and lateral walls are involved near the roof.
15. For optic nerve decompression in the optic canal, the posterior lacrimal crest, ethmoid and sphenoid are infractured to reach the medial wall of the optic canal.
16. Lacrimal bone is very fragile therefore an extra precaution should be taken to avoid trauma in cases of surgery of the lacrimal system.
17. A penetrating object will enter the orbit through an orbital opening and damage the adjacent regions depending upon its directions, for example:
- Directed upwards and medially: It will enter the frontal sinus in the anterior part and anterior cranial fossa more posteriorly.
- Directed towards the floor: It will enter the maxillary sinus.
- Directed backwards: It will enter the middle cranial fossa through the superior orbital fissure and damage the temporal lobe.
18. Ethmoidal malignancy may erode the optic canal and compress the optic nerve.
19. Tumours in the adjacent regions may enter the orbit through large communications. From the middle cranial fossa, it passes through the superior orbital fissure while from the temporal fossa, it traverses the inferior orbital fissure.
20. An orbital tumour will push the eyeball forward producing exophthalmos.
21. Since the lateral orbital margin lies relatively more posteriorly than the medial orbital margin, a lateral approach is preferred for the operations on the eyeball.