
Occipital Bone
Occipital Bone Terminology
The word ‘occipital’ is derived from the Greek words ‘ob’ (meaning back) and ‘cipit’ (meaning head). Hence referred to the back of the head.
Occipital Bone Location
The occipital bone occupies the posterior part of a skull and plays a major role in the formation of the posterior cranial fossa.
Occipital Bone Features And Attachments
The largest foramen of the skull called foramen magnum, is located in the occipital bone. The components of occipital bone are better described in relation to this foramen.
It consists of 1 basilar part (above and in front of the foramen magnum), 2 lateral parts (lateral to the foramen magnum), and 1 squamous part (above and behind the foramen magnum).
Foramen Magnum
1. It is located on the floor of the posterior cranial fossa.
2. It provides communication between the posterior cranial fossa and vertebral canal.
3. Its margins provide attachments to the following structures:
- Anterior margin: Anterior atlanto-occipital membrane.
- Posterior margin: Posterior atlanto-occipital membrane.
- Lateral margins: Alar ligament.
4. Structures passing through the foramen magnum are as follows:
- Anterior Part
- Apical ligament of dens.
- Superior longitudinal band of cruciform ligament.
- Membrana tectoria.
- Posterior Part
- Medulla oblongata.
- Meninges.
- Spinal roots of accessory nerves.
- Meningeal branches of upper cervical nerves (C1-3)
- Vertebral arteries.
- Sympathetic plexuses around vertebral arteries.
- Anterior and posterior spinal arteries.
Basilar Part
It extends upwards and forwards to meet the body of the sphenoid. Before 25 years of age growth cartilage intervenes between the sphenoid and basilar part of the occipital bone but after this period the two bones fuse. The basilar part has two surfaces (superior and inferior) and two lateral margins.
- Superior Surface
- It is smooth.
- It forms a clivus with the body of the sphenoid.
- It is related to medulla oblongata.
- Its lower part receives attachments of the following structures from above downwards:
- Membrana tectoria.
- Superior longitudinal band of cruciform ligament.
- Apical ligament of dens.
- Its lateral margins are grooved by inferior petrosal sinuses.
- Inferior Surface
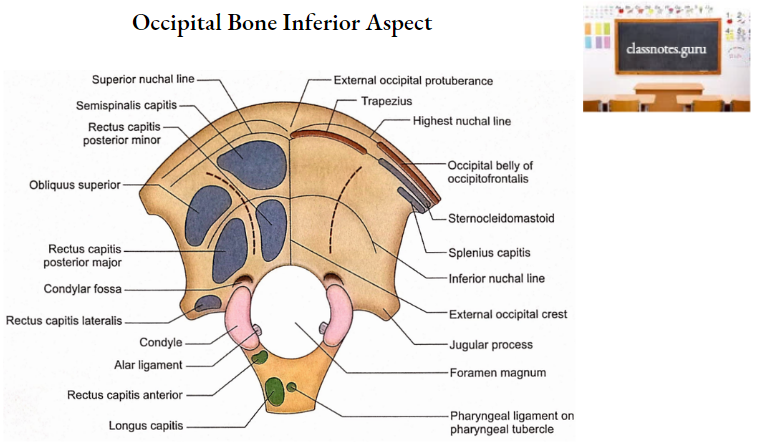
- Its middle is marked by a tubercle called the pharyngeal tubercle. This tubercle is approximately 1 cm anterior to the foramen magnum.
- Attached to this tubercle is the upper part of the pharyngeal raphe (pharyngeal ligament).
- The anterolateral to pharyngeal tubercle is the area for longus capitis.
- Posterolateral to pharyngeal tubercle (just in front of condyle) is the attachment of rectus capitis anterior.
- Lateral Margins
- These are rough and articulate with petrous parts of the temporal bones.
Lateral Parts (Right And Left)
Each can be divided into a broader medial portion (adjacent to the foramen magnum) and a narrower lateral portion (jugular process).
1. Medial Portion
- Inferior surface
- It is marked by an articular occipital condyle.
- The articular surface of the occipital condyle is oval and convex to articulate with the concave superior articular process of the atlas.
- The occipital condyle is located lateral to the anterior half of the foramen magnum.
- Behind the condyle is the condylar fossa which may have a condylar canal for the emissary vein from the sigmoid sinus.
- Lateral to the anterior part of the condyle is the outer opening of the hypoglossal canal.
- Medial aspect
- It has got a tubercle and a foramen.
- The tubercle is situated on the medial aspect of the condyle and provides attachment to the alar ligament.
- The foramen located just above the tubercle forms the inner opening of the hypoglossal canal.
- The following structures pass through the hypoglossal canal:
- Hypoglossal nerve.
- Meningeal branch of ascending pharyngeal artery.
- Superior surface
- It is marked by an oval eminence called a jugular tubercle.
- The jugular tubercle overlies the hypoglossal canal.
- The posterior part of the jugular tubercle often presents a shallow groove for 9, 10, and 11 cranial nerves.
2. Jugular Process
- Its lateral end presents a rough area that joins the jugular surface of the temporal bone by a growth cartilage. The cartilage ossifies at the age of 25 years.
- Its anterior margin is notched and completes the jugular foramen with a similar notch on the posterior border of the petrous part of the temporal bone.
- Its superior surface is marked by a deep groove that lodges the terminal part of the sigmoid sinus.
- Its inferior surface provides attachment to rectus capitis lateralis.
Squamous Part
It has two surfaces (external and internal), three angles (one superior and two lateral), and four borders (two lambdoid and two mastoid).
1. Surfaces
- External Surface
- The middle of the external surface is marked by a projection called external occipital protuberance.
- Two lines extend laterally on each side from the external occipital protuberance.
- A superior faint line is called the highest nuchal line. This provides attachment to the occipital belly of occipitofrontalis
- An inferior well-defined line is called a superior nuchal line. This receives attachments of the trapezius and sternomastoid in its medial and lateral parts respectively.
- A midline ridge extends from the external occipital protuberance to the foramen magnum. This is called the external occipital crest. It gives attachment to ligament nuchae.
- Running laterally on each side from the middle of the external occipital crest is another ridge called the inferior nuchal line.
- There are two muscles attached between the superior and inferior nuchal lines on both sides, i.e. semispinalis capitis (medially) and obliquus capitis superior (laterally).
- Similarly, there are two muscles attached to each side of the midline below the inferior nuchal line, i.e. rectus capitis posterior major (laterally) and rectus capitis posterior minor (medially).
- Note: Remember that the rectus capitis muscles are named after their relations with the occipital condyle. The one lying anterior to the condyle is rectus capitis anterior.
- The muscle lying lateral to the condyle is called rectus capitis lateralis. Rectus capitis posterior will naturally be located behind the condyle.
- Since the latter muscle is two in number, these are further qualified by adding ‘major’ and ‘minor’ to their names.
- It is interesting to note that rectus capitis anterior, lateral, and posterior are attached to three components of the occipital bone, i.e. basilar part, lateral part, and squamous part respectively.
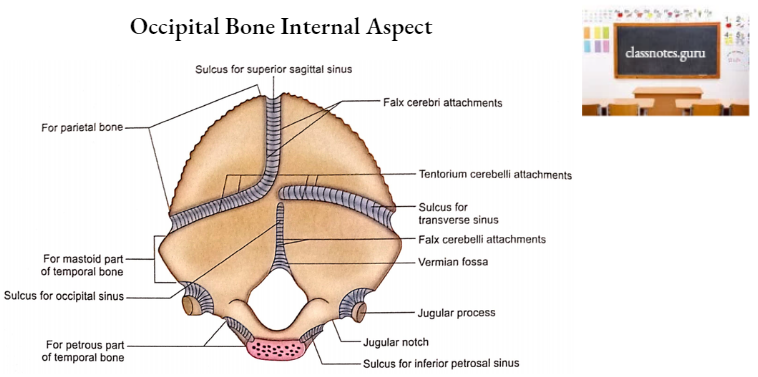
- Internal Surface
- Its middle is marked by an elevation called internal occipital protuberance which corresponds with the external occipital protuberance on the external surface.
- Four grooves diverge from the internal occipital protuberance, one upwards, one downwards, and two laterally whose margins provide attachments to falx cerebri, falx cerebelli, and tentorium cerebelli respectively.
- The groove running upwards is produced by the superior sagittal sinus.
- The groove running downwards is occupied by the occipital sinus.
- The groove extending laterally is produced by the corresponding transverse sinus.
- The internal surface is marked by a depression in the midline near the posterior margin of the foramen magnum. This is vermian fossa related to inferior vermis of cerebellum.
- Midline elevation extending from internal occipital protuberance to the posterior margin of foramen magnum is called internal occipital crest. Falx cerebelli is attached to it.
- On each side of the internal occipital crest, a hollow is related to the cerebellar hemisphere.
- The internal surface above the grooves for part of the corresponding temporal bone to form transverse sinuses is related to the occipital lobes of the cerebrum.

2. Angles
- The superior angle reaches lambda which during intrauterine life is membranous (posterior fontanelle).
- The lateral angle on each side meets with the mastoid part of the corresponding temporal bone to form an asterion.
3. Borders
- Lambdoid Border
- It extends on each side from the superior angle to the lateral angle and articulates with the posterior margin of the corresponding parietal bone to form the lambdoid suture.
- Mastoid Border
- It extends on each side from a lateral angle to the jugular process and articulates with a mastoid occipitomastoid suture.
Occipital Bone Ossification
- Origin
- Part of the occipital bone above the highest nuchal line develops in the membrane.
- The rest of the occipital bone ossifies in cartilage.
- Appearance Of Centres
- Usually, seven centers appear in the 8th week of intrauterine life as follows:
- Four for the squamous part (one for each half of the membranous and cartilaginous parts).
- Two for lateral parts.
- One for the basilar part.
- Fusion
- Membranous and cartilaginous portions fuse with each other when the baby starts holding the neck, i.e. 3rd month.
- Squamous part fuses with lateral parts when primary dentition is completed, i.e. at 2 years.
- Lateral parts fuse with the basilar part when the permanent dentition begins, i.e. at 6 years.
- The basilar part fuses with the sphenoid and the lateral part fuses with the temporal bone at the age of 25 years.
- Note: Remember, the occipital condyle is contributed partly from the lateral part and partly from the basilar part of the occipital bone.
Occipital Bone Applied Anatomy
The squamous part of the occipital bone contributing to the vault is prone to both fissured and depressed fractures but the portions lying in the base of the skull always show a linear fracture.
- Margins of the foramen magnum form natural thick bony buttresses at the base of the skull, therefore, the fracture lines often converge towards the foramen magnum.
- A crack in the inner table of the squamous part of the occipital bone may damage the large diploic vein and produce a small epidural hematoma.
- Almost invariably fractures of the squamous part of the occipital bone in children are associated with rupture of the dura mater.
- Basal fracture of the skull involving the hypoglossal canal will damage the hypoglossal nerve.
- A gap in the squamous part of the occipital bone forming the cranial vault is usually filled with tantalum or titanium due to a lack of regeneration in this part whose periosteum is devoid of the cambium layer.