
Cysts And Tumours Of The Orofacial Region Definition
Cyst: It is pathological cavity containing fluid, semi fluid or gas, which is usually lined by epithelium & is not formed by the accumulation of pus
Tumour: It is defined as an abnormal new, uncoordinated growth in the body which results from excessive, autonomous, purposeless proliferation of cells which continues even after cessation of stimuli
Cysts And Tumours Of The Orofacial Region Important Notes
1. Classification Of cyst
Epithelial Cyst:
- Odontogenic cysts
Developmental Cysts:
- Primodial cyst
- Gingival cysts of Infants
- Dentigerous cyst
- CEOC
Inflammatory Cysts:
- Radicular cyst
- Residual cyst
- Paradental cyst
Non-odontogenic Cysts
- Naso palatine cyst
- Globulomaxillary cyst
- Nasolabial cyst
Non-Epithelial Cyst:
- Simple bone cyst
- Traumatic bone cyst
- Solitary bone cyst
- Aneurysmal bone cyst
Read And Learn More: Oral and Maxillofacial Surgery Question and Answers
2. Classification Of Tumours:
- Benign Tumours:
- Epithelial Origin
- Ameloblastoma
- CEOT
- With Mesenchymal Origin
- Ameloblastic fibroma
- CEOC
- Odontoma
- With Epithelial & Mesenchymal Origin:
- Odontogenic fibroma
- Odontogenic fibroma
- Epithelial Origin
- Malignant Tumours:
- Odontogenic carcinoma
- Malignant ameloblastoma
- Primary intraosseous carcinoma
- Odontogenic sarcoma
- Ameloblastic fibrosarcoma
- Ameloblastic fibrodentinosarcoma
- Odontogenic carcinosarcoma
- Odontogenic carcinoma
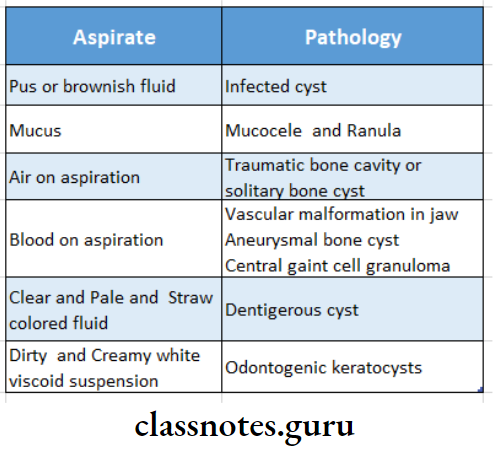
3. Aspirates In Different Cysts:
4. Methods Of Treatment Of Cysts:
- Enucleation
- Marsupialization
- Combination of enucleation and marsupialization
- Enucleation and curettage
5. Enucleation:
- Enucleation is shelling out of the entire cystic lesion without rupture
- The majority of smaller cysts are treated by enucleation
- By it pathological examination of entire cyst can be undertaken
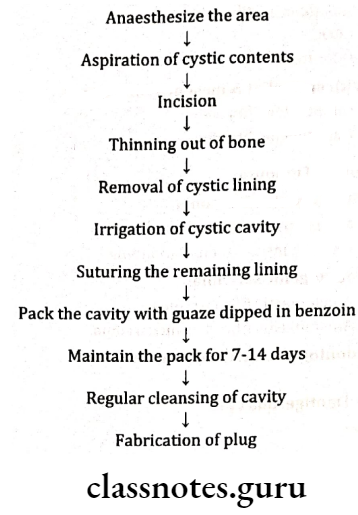
6. Marsupialization:
- Marsupialization refers to creating a surgical window in the wall of the cyst, evacuating the contents of cyst and maintaining continuity between the cyst and the oral cavity
- The only portion of the cyst that is removed is the piece removed to produce the window
- Marsupialization is simple procedure to perform
- The disadvantage is that pathologic tissue is left in situ without thorough histologic examination
7. Indications Of Marsupialization
- If the cyst is closer to vital structures
- If unerupted tooth is involved in the cyst
- In larger cysts
- In an unhealthy patient
- In young children
8. Combination Of Marsupialization And Enucleation:
- In this first marsupialization is performed followed by enucleation
- The advantage of this technique is the development of a thickened cystic lining which makes secondary enucleation an easier procedure
9. Enucleation And Curettage:
- After enucleation, a curette or bur is used to remove 1-2 mm of bone around the entire periphery of the cystic cavity to remove any remaining epithelial cells that are present in the periphery which may proliferate into a recurrency of the cyst
- Indications:
- Odontogenic keratocyst
- Any cyst that recurs after what was deemed a thorough removal
10. Segmental Resection Of The Mandible:
- For it, a combination of Hinds and Risdon incisions are placed at least 2 cm below and parallel to the inferior and posterior borders of the mandible
- Care should be taken to prevent the damage of mandibular branch of the facial nerve
11. Moore And Weber Fergusson Incision:
- Moore And Weber Fergusson Incision is given for hemimaxillectomy
- The incision starts from the inner canthus of eye runs along the area of the nose and then drops down the midline upto the philtrum of the lip
- If there is involvement of lymph nodes, radial neck dissection or commando operation is carried out
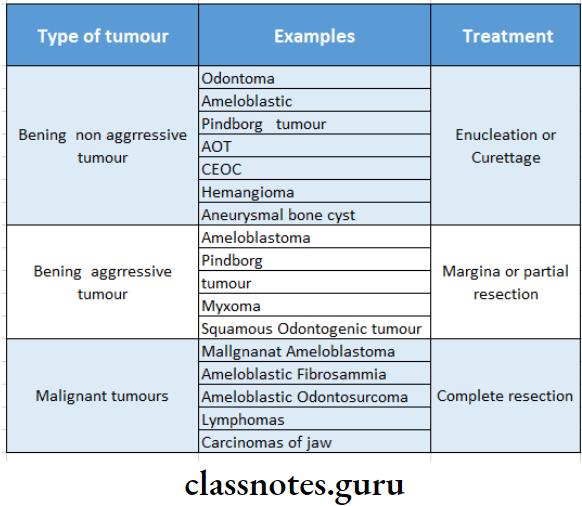
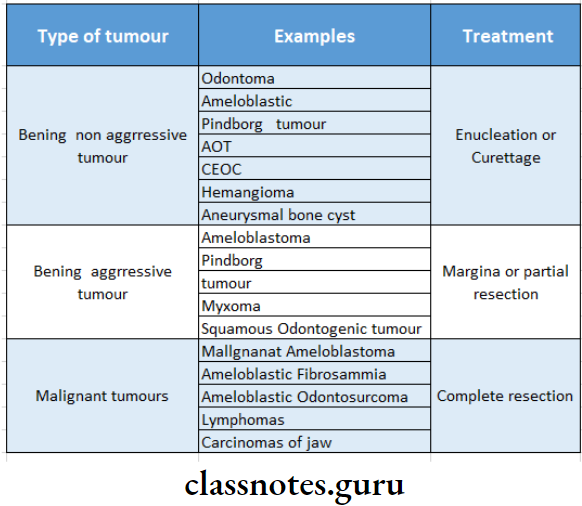
12. Tumours:
Cysts And Tumours Of The Orofacial Region Long Essays
Question 1. Classification of odontogenic tumours. Describe in detail ameloblastoma.
Or
Define and classify Ameloblastoma. Discuss in detail the management of Ameloblastoma of the right body of the mandible.
Or
Define tumours & classify odontogenic tumours
Answer:
Classification Of Odontogenic Tumours:
1. Benign Tumours:
- Epithelial origin:
- Ameloblastoma
- CEOT
- With mesenchymal origin:
- Ameloblastic fibroma
- CEOC
- Odontoma
- With epithelial & mesenchymal origin:
- Odontogenic fibroma
2. Malignant Tumours:
- Odontogenic Carcinoma:
- Malignant ameloblastoma
- Primary intraosseous carcinoma
- Odontogenic Sarcoma:
- Ameloblastic fibrosarcoma
- Ameloblastic fibrodentinosarcoma
- Odontogenic carcinosarcoma:
Definition Of Ameloblastoma :
Ameloblastoma is a benign, but locally invasive polymorphic neoplasms consisting of proliferating odontogenic epithe- lium which is usually in a follicular or plexiform pat- tern lying in a fibrous stroma
Clinical Features of Ameloblastoma:
- Sex: Both sex
- Age 1st to 7th decade
Types Of Ameloblastoma:
- Solid Or Multicystic Ameloblastoma:
- Slow-growing locally invasive tumours
- High recurrence rate
- Unicystic Type:
- The lesion can be enucleated Rarely seen in maxilla
- The recurrence rate is low
- Peripheral Ameloblastoma:
- Does not invade bone
- Treated in the early stages of development
Features Of Ameloblastoma:
- Swelling & pain in the region
- Inflammation
- Tension
- Dental trauma
- Ulceration of mucosa
- Loosening of teeth
- Epistaxis
- Nasal obstruction
Radiological Features Of Ameloblastoma:
- Unilocular or multi locular radiolucency
- Soap bubble appearance of the lesion
- Border is clear
- Resorption of the teeth
Management Of Ameloblastoma:
- For intraosseous marginal resection
- Segmental resection
- Aggressive resection
Jackson’s Guidelines:
- Tumour confined to maxilla without orbit floor i involvement-Partial maxillectomy
- Tumour involving orbital floor-Total maxillectomy
- Tumour involving orbital contents – Total maxillae tomy with exenteration
- Tumour involving skull bone-Neurological procedure
Question 2. Classify cysts of oral cavity. Describe in detaill about clinical features, radiological features & management of OKC,
Or
Classify jaw cysts. Describe clinical features, radiological features, pathogenesis and management of odontogenic keratocyst.
Or
Define OKC
Answer:
Classification Of Keratocyst:
1. Epithelial Cysts
- Odontogenic Cysts:
- Developmental cysts:
- Primordial cyst
- Gingival cysts of infants
- Dentigerous cyst
- CEOC
- Inflammatory Cysts:
- Radicular cyst
- Residual cyst
- Paradental cyst
- Developmental cysts:
- Non odontogenic Cysts:
- Naso palatine cyst
- Globulomaxillary cyst
- Nasolabial cyst
2. Non-Epithelial Cyst:
- Simple bone cyst
- Traumatic bone cyst
- Solitary bone cyst
- Aneurysmal bone cyst
Odontogenic Keratocyst:
- Pathogenesis:
- Odontogenic keratocyst arises from
- Dental lamina
- The primordium of developing tooth germ
- The basal layer of oral epithelium
- Odontogenic keratocyst arises from
- Develops due to cystic degeneration of cells of stellate reticulum in developing tech germ
Clinical Features Of Keratocyst:
- Age: 23 decades
- Sex: Common in males
- Site: Mandible
Features Of Keratocyst:
- Asymptomatic
- Secondary infection, causes expansion of cortical pilates
- Mobility of teeth
- Pattu & tenderness of the site
Radiological Features Of Keratocyst:
- Unilocular or multilocular radiolucency
- Margitus: Well-defined sclerotic margins
- Expansion of cortical plates
- Soap bubble appearance
Management Of Keratocyst:
1. Enucleation Of cyst:
- Smaller single cyst through intraoral approach
- Unilocular lesions through marginal excision
- Large multilocular lesions
Question 3. Define cyst. Describe the pathogenesis, clinical features, radiographic appearance of radicular cyst , Treatment, Aetiology
Or
Radicular cyst
Answer:
Definition Of Cyst:
Cyst is a pathological cavity containing fluid, semi-fluid or gas, which is usually lined by epithelium & is not formed by the accumulation of pus
Radicular Cyst:
- Pathogenesis:
- Phase Of Initiation:
- Bacterial infection
- Leads to stimulation of cell rest of Malassez
- Phase of proliferation:
- Excessive & exuberant proliferation of cell rests
- Phase Of Mystification:
- Deprivement of nutrition of central cells
- Results in necrosis
- Formation of cyst
- The Phase Of Enlargement: Enlargement Of The Cavity Due To:
- Higher osmotic tension of the cystic fluid
- Release of bone-resorbing factors
- Phase Of Initiation:
Clinical Features Of Cyst:
- Sex: Common in males
- Age: Young age
- Site: Common in maxillary anterior
- Non-vital tooth
- Smaller cysts are asymptomatic
- Larger lesions produce slow enlarging, bony hard
swelling - Expansion & distortion of cortical plates
- Severe bone destruction
- The springiness of jaw bones
- Pain if secondary infected
- Intraoral or extraoral pus discharge
- Pathological fractures
- Formation of abscess called “cyst abscess”
Radiological Features Of Cyst:
- The unilocular radiolucent area around the apex of nonvital tooth
- Border: Sclerotic
- Diameter: Less than 1 cm
- Discontinuity of lamina dura
Treatment Of Cyst:
- Non-vital tooth
- Extraction
- RCT
- Smaller cyst
- Removed through socket
- Larger cyst
- Marsupalization
Aetiology Of Cyst:
- Dental caries
- Fractured tooth
- Thermal/Chemical injury to the pulp
- Latrogenic injury to pulp
Question 4. Differentiate between benign & malignant tu- mours.
Answer:
Differentiate Between Benign & Malignant Tumours
Cysts And Tumours Of The Orofacial Region Short Essays
Question 1. Dentigerous cyst.
Answer:
Clinical Features Of Dentigerous Cyst:
- Sex: Common in males
- Age: 1& 3rd decade
- Site: Mandibular 3rd molar, maxillary canines, maxillary 3rd molar
- Expansion of bone
- facial asymmetry
- Displacement of adjacent teeth
- Resorption of adjacent teeth
Radiological Features:
- Unilocular, well-defined radiolucency
- Margins – Sclerotic
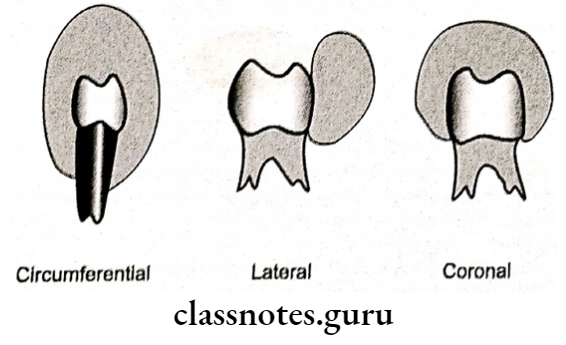
Types Of Dentigerous Cyst:
- Central covering the crown of an unerupted tooth
- Circumferential covering the crown from all the sides
- Lateral covering crown from side
Management of Dentigerous cyst:
- Marsupialization in children
- Enucleation in adults
Question 2. CEOC.
Answer:
Clinical Features Of CEOC:
- Age: Second decade of life
- Sex: Both sexes
- Site: Mandibular premolars
- Anterior of maxilla
- Features: Bony hard swelling of the jaw
- Expansion & distortion of cortical plates
- Vital tooth
- Gingival swelling
- Causes perforation of cortex
- Pain is rarely present
Radiological Features Of CEOC:
- Unilocular or multilocular radiolucent area
- Border: well corticated
- Internal structure: radiopaque calcified foci present
Treatment Of CEOC:
- Simple enucleation
Question 3. Marsupialization.
Answer:
Marsupialization
Marsupialization refers to creating a surgical window in the wall of the cyst & evacuation of the cystic contents
Indications Of Marsupialization:
- Young age
- Proximity to vital structures
- In case of eruption of teeth
- In larger cyst
- In vital teeth
Advantages Of Marsupialization:
- Simple
- Spares vital structures
- Allows eruption of teeth
- Prevents OAF
- Prevents fractures
- Less time
- Reduces blood loss
- Bone formation
Disadvantages Of Marsupialization:
- Prolonged healing
- Prolonged follow up Periodic irrigation
- Periodic changing of pack
- Risk of new cyst formation
The technique of Marsupialization:
Question 4. Enucleation:
Answer:
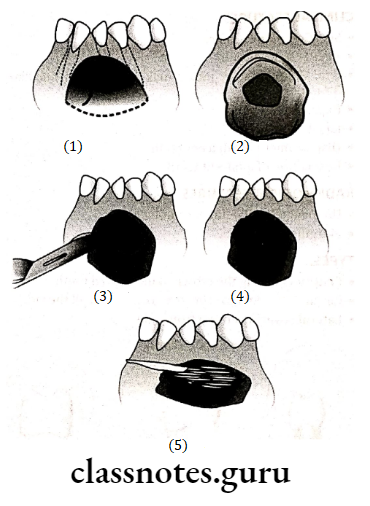
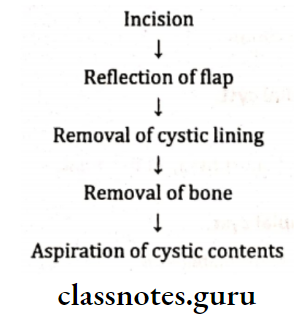
Enucleation
Enucleation allows for the cystic cavity to be covered by a mucoperiosteal flap & the space is filled with a blood clot which organizes & forms normal bone
Indication Of Enucleation:
- OKC
- Recurrent cyst
Advantages Of Enucleation:
- Primary closure Rapid healing
- Postoperative care is less
Disadvantages Of Enucleation:
- Weakens the mandible
- Damage vital structures
- Pulpal necrosis
Technique Of Enucleation:
Question 5. Osteoma.
Answer:
Osteoma
Benign neoplasm of osseous origin
Clinical Features Of Osteoma:
- Age: Second-fifth decade
- Sex: Common in females
- Site: Jawbones, soft tissues
Presentation Of Osteoma:
- Nodular, exophytic growth. Either solitary or multiple
- Expansion of cortical plates
- Displacement of teeth
- Predispose to sinusitis Nasal discharge
- Syndrome associated
Radiographic Features Of Osteoma:
- Well circumscribed
- Round or oval dense radiopacities
Treatment Of Osteoma:
- Surgical excision
Question 6. Myxoma.
Answer:
Myxoma
- True neoplasm
- Made up of tissues that often resemble primitive mes enzyme
Clinical Features Of Myxoma:
- Age: At any age
- Sex: Both
- Site: Iaw bones, salivary gland
Presentation Of Myxoma:
- Non-descript, firm, nodular growth
Treatment Of Myxoma:
- Radical surgery
Question 7. AOT
Answer:
AOT
Origin: Reduced enamel epithelium
Clinical Features Of AOT:
- Age: Young age
- Sex: Female
- Site: Maxillary anterior region
Presentation Of AOT:
- Slow enlarging, small, bony hard swelling
- Elevation of upper lip
- Displacement of teeth
- Expansion of cortical plates
- Asymptomatic
- Nodular swelling over gingiva
Treatment Of AOT:
- Surgical enucleation
Question 8. Pinborg tumour
Answer:
Clinical Features Of Pinborg:
- Age: Middle age
- Sex: Both
- Site: Mandible , over gingiva
Presentation Of Pinborg Tumour:
- Slow enlarging bony hard swelling Expansion of cortical plates
- Displacement of teeth
- Pain
- Paresthesia.
- Maxillary lesions lead to nasal airway obstruction Nodular swelling over gingiva
Radiographic Features Of Pinborg Tumour:
- Well-defined, unilocular, radiolucent area
- Interior small radiopaque foci
Treatment of AOT:
- Surgical enucleation
Question 9. Globulomaxillary cyst.
Answer:
Globulomaxillary Cyst
- A common type of developmental cyst
- Arises in the bone suture, between maxilla & pre maxilla
Clinical Features Of Globulomaxillary Cyst:
- Asymptomatic
- If secondary infected, causes pain & discomfort
- Small swelling between canine & premolar
- Vital teeth
Radiographic Features Of Globulomaxillary Cyst:
- Inverted pear-shaped radiolucent area between roots of the upper lateral incisor & canine
- Divergence of the roots
Treatment Of Globulomaxillary Cyst:
- Surgical excision
Question 10. Traumatic bone cyst.
Answer:
Traumatic Bone Cyst
- Pseudo cyst
- Lined by fibrous tissue
Clinical Features Of Traumatic Bone Cyst:
- Ages: Young age
- Sex: Common in males
- Site: Mandibular body, symphysis or ramus Maxillary anterior region
Presentation Of Traumatic Bone Cyst:
- Asymptomatic
- Painful, bony hard swelling Expansion of cortical plates
- Displacement of teeth
- Pain
- Paresthesia of lip
- Vital teeth
Radiographic Features Of traumatic Bone Cyst:
- Unilocular or multilocular radiolucent lesion
- Well demarcated
- Scalloping between roots
Treatment Of Traumatic Bone Cyst:
- Surgical exploration
Question 11. Nasolabial cyst.
Answer:
Nasolabial Cyst
Soft tissue cyst of the nasolabial fold
Origin Of Nasolabial Cyst:
- The lower part of the embryonic nasolacrimal duct
Clinical Features Of Nasolabial Cyst:
- Age: 30-50 years
- Sex: Common in females
- Site: Soft tissue of anterior maxillary vestibule
Presentation Of Nasolabial Cyst:
- Small, painless swelling of the upper lip
- Distorts the nostrils
- Projects into the floor of the nose
- Radiographic Features:
- Saucerization of the underlying bone
Treatment Of Nasolabial Cyst:
- Surgical excision
Question 12. Odontomes
Answer:
Odontomes
- Common hamartomatous odontogenic lesions with limited growth potential
Types Of Odontomes:
- Complex odontoma: Consists of a mass of haphazardly arranged enamel, dentin & cementum
- Compound odontoma: Consists of collections of numerous small, discrete, tooth-like structures
Clinical Features Of Odontomes:
- Age: Children & young adults
- Sex: Both
- Site: Compound in Maxilla Complex in the mandible
Presentation Of Odontomes:
- Small asymptomatic lesion Expansion of cortical plates
- Displacement of teeth Impacted or retained deciduous teeth
- Pain, inflammation
- Ulceration
- Fistula formation
Radiographic Features Of Odontomes:
- Compound – A bag of teeth appearance
- Complex – Sunburst appearance
Treatment Of Odontomes:
- Surgical enucleation
Cysts And Tumours Of The Orofacial Region Short Question And Answers
Question 1. Theories of cystic expansion.
Answer:
Theories Of Cystic Expansion
- Harris Theory:
- According to him, cystic expansion involves
- Mural Growth:
- Peripheral cell division.
- Accumulated contents
- Hydrostatic:
- Secretion
- Transudation & exudation
- Dialysis
- Bone Resorbing Factors:
Question 2. Gorlin’s syndrome.
Answer:
Clinical Features Of Gorlin’s Syndrome:
- Facial:
- Frontal bossing
- Prominent Supraorbital ridges
- Hypertelorism
- Mandibular prognathism
- Skeletal Anomalies Of :
- Bifid ribs
- Bifid spine
- Bridging of sella
- Shortening of metacarpals
- Calcification of falx cerebri
- Skin Lesions:
- Milia
- Dyskeratosis
- Basal cell nevi
- Cysts:
- Multiple keratocyst
- Soft Tissue Anomalies:
- Ovarian fibromata
- Lipomas
Question 3. Aneursymal bone cyst.
Answer:
Aneursymal Bone Cyst
An aneurysmal bone cyst is a cystic lesion involving hone anywhere in the body
Clinical Features Of Aneurysmal Bone Cyst:
- Age- Second decade of life
- Sex – Common in females
- Site Mandibular molar- Ramus area and maxillary posterior area
- Present as rapidly enlarging, diffuse, firm swelling of the Jaw
- Causes facial asymmetry
- Swelling is painful
- Expansion and thinning of bone results in egg- Shell crackling
- Perforation of cortical bone
- Pathological fracture of affected jawbone Paraesthesia of regional teeth
- Difficulty in mouth opening due to impingement on the capsule of TMJ
- Maxillary lesions cause nasal bleeding, pressure sensation in the eye and nasal obstruction
Question 4. Carnoy’s solution
Answer:
Carnoy’s Solution
- Carnoy’s Solution is a chemical cauterization agent
- Indicated in the treatment of keratocystic odontogenic tumours
- Carnoy’s Solution contains:
- 100% ethanol
- Chloroform
- The glacial acetic acid in a ratio of 6:3:1 with added ferric chloride
- Carnoy’s Solution provides a tissue fixation property used in histology and a tissue cauterization property utilized in chemical curettage
Cysts And Tumours Of The Orofacial Region Viva Voce
- Complete resection is done if the tumour invades the lower border of the mandible
- Marsupialization decreases intra-cystic pressure and promotes shrinkage of the cyst and bone fill
- Aspiration helps to distinguish between a cyst and tumour
- Large ranulas can be best treated by marsupialization
- Recurrent ranulas are best treated by sublingual gland excision
- Marsupialization is the best method to treat large cysts
- Bifid mandibular canal is common in neurofibroma- tosis
- Junctional nevus has the maximum potential to become melanoma
- Retention cysts are commonly seen in the lower lip
- Bohn’s nodules are cystic swellings in neonates
- The protein content of periapical and dentigerous cysts is 5-11 gm/dl
- Complete enucleation of cyst in the palatal area carries the danger of tear of the nasal mucosa
- During enucleation, the incision should be placed on the firm bony base
- Treatment of keratocyst is excision
- The global maxillary cyst occupies a bony region between the maxillary lateral incisor and canine
- Ranula is a retention cyst
- Mucocele should be treated by enucleation of the cyst and minor salivary gland
- A branchial cyst occurs on the lateral side of the neck.
- Pindborg’s tumour is treated by excision
- Adenoameblastoma is managed by enucleation
- Chondromas are radioresistant
- Keratocyst has the highest rate of recurrence