Environmental And Nutritional Disorders Important Notes
1. Vitamins
- Fat-soluble vitamins
- Water soluble vitamins
Environmental And Nutritional Disorders Long Essays
Question 1. Classify vitamins. Discuss the role of vitamin D in rickets.
Answer:
Vitamins:
- Vitamins are organic substances which cannot be synthesized with the body and are essential for the maintenance of the normal structure and function of cells.
Vitamins Classification: Vitamins are divided into 2 groups.
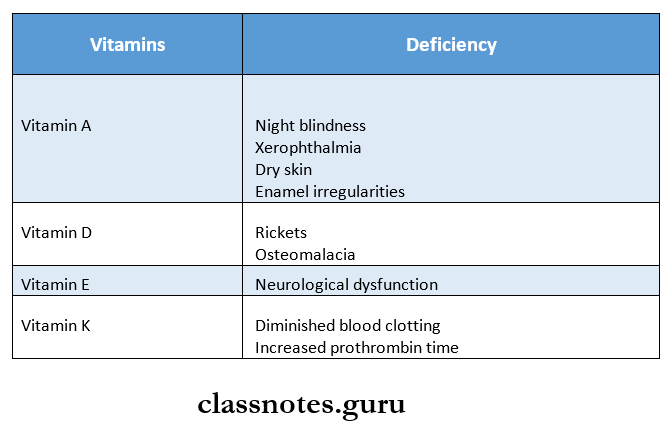
1. Fat-soluble vitamins – A, D, E, K
- They are absorbed from the intestine in the presence of the bile salts and intact pancreatic function.
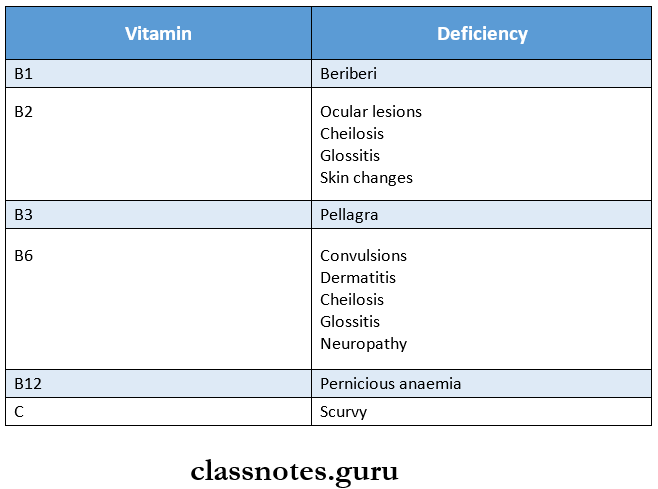
2. Water-soluble vitamins – B and C
- They are more readily absorbed from the small intestine.
Vitamin D: (Calcitriol):
- Vitamin D is a fat-soluble vitamin, commonly known as anti-rachitic vitamin
- Deficiency of vitamin D results in
- Rickets in children
- Osteomalacia in adults
Rickets:
Rickets a clinical disorder seen in growing children from 6 months to 2 years of age due to a deficiency of Vit. D.
Pathogenesis of rickets occurs in the following sequence:
1. Endochondral ossification is long tubular bones.
- Overgrowth of epiphyseal cartilage due to proliferation of cartilage cells at the epiphyseal cartilage due to proliferation of cartilage cells at the epiphyses followed by inadequate provisional calcification/mineralization.
- Persistence and overgrowth of epiphyseal cartilage, deposition of osteoid matrix on inadequately mineralized cartilage resulting in enlargement and lateral expansion of the osteochondral junction.
- Deformation of the skeleton due to loss of struc-tural rigidity of the developing bones.
- Irregular overgrowth of small blood vessels in disorganized and weak bones.
Read And Learn More: Pathology Question And Answers
2. Intramembranous ossification in flat bones. Mesenchymal cells differentiate into osteoblasts with lying down of osteoid matrix which fails to get mineralized resulting in soft and weak feat bones.
Rickets Clinical Features:
- The gross skeletal changes depend on the severity of the rachitic process, its duration, and in particular the stresses to which individual bones are subjected.
- Craniotabes, the earliest bony lesion occurring due to small round unossified areas in the membranous bones of the skull.
- Harrison’s sulcus which occurs due to in drawing of soft ribs on inspiration.
- Pigeon chest deformity
- Bow legs occur in ambulatory children due to weak bones of the lower legs.
- Knocked knees may occur due to enlarged ends of the femur, tibia, and fibula.
- Lower epiphyses of the radius may be enlarged.
- Lumbar lordosis due to involvement of the spine and pelvis.
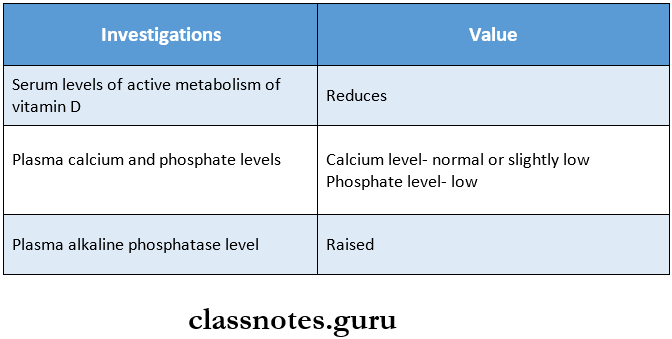
Rickets Biochemical changes:
- Lowered levels of active metabolites of vitamin D.
- Normal or slightly low plasma calcium levels, low plasma phosphate levels and raised plasma alkaline phosphatase levels.
Environmental And Nutritional Disorders Short Essays
Question 1. Pellagra
Answer:
- Niacin deficiency causes Pellagra i.e., rought skin.
- The cardinal manifestations of pellagra are referred to as the three D’s i.e., dermatitis, diarrhea, and dementia and if not treated may lead to 4th D i.e., death.
- Dermatitis: Sun-exposed areas of skin developed erythema resembling sun-burn which may progress to chronic type with blister formation.
- Diarrhea: This is seen along with stomatitis, glossitis, enteritis, nausea and vomiting.
- Dementia: Degeneration of neurons of the brain of the spinal tract results in neurological symptoms such as dementia, peripheral neuritis, ataxia, and visual and auditory disturbances.
- Oral findings include:
- The bald tongue of sandwich,
- Raw beefy tongue
- Mucosa becomes fiery red and painful
- Profuse salivation.
- Chronic alcoholics are at high risk of developing pellagra because in addition to dietary deficiency, niacin absorption is impaired in them.
Question 2. Osteomalacia
Answer:
- Osteomalacia is the adult manifestation of Vit. D deficiency is characterized by failure of mineralization of the osteoid matrix.
- Due to failure of mineralization, excess of persistent osteoid is produced which is a characteristic of osteomalacia.
- The contours of the bone is not affected, but the bone is weak and vulnerable to fractures.
- Other clinical features include
- Muscular weakness,
- Vague body pains,
- Fractures following trivial trauma,
- Losser’s zones/pseudofractures at weak places in bones.
- Biochemical changes include
- Normal/low serum calcium levels, low plasma phosphate levels, and raised serum alkaline phosphatase due to increased osteoblastic activity.
Question 3. Manifestations of vitamin A deficiency.
Answer:
Lesions in Vitamin A deficiency:
- Ocular lesions:
- Night blindness,
- Xerophthalmia, dry and scaly sclera, conjunctiva
- Keratomalacia due to infections of corneal ulcers,
- Bitot’s spots are focal triangular areas of opacities due to the accumulation of keratinized epithelium.
- Blindness due to infection, scarring, and opacities.
- Cuntaneous lesions :
- Xeroderma/toad-like appearance of skin because of papular lesions due to follicular hyperkeratosis and keratin plugging in the sebaceous glands.
- Other lesions:
- Squamous metaplasia of
- Respiratory epithelium,
- Pancreatic ductal epithelium,
- Urothelium
- Long-standing metaplasia may progress to anaplasia.
- Immune dysfunction.
- Pregnant women may have an increased risk of maternal infection, mortality, and impaired embryonic development
- Squamous metaplasia of
Question 4. Beriberi.
Answer:
Deficiency of Thiamine results in beriberi
Beriberi Symptoms:
- Loss of appetite
- Weakness
- Constipation
- Nausea
- Mental depression
- Peripheral neuropathy
- Irritability
- Numbness in the legs
Beriberi Types:
1. Wet beriberi
- Characterized by edema of legs, face, trunk, and serous cavities
2. Dry beriberi
- Associated with neurological manifestations
3. Infantile beriberi
- Seen in infants
Environmental And Nutritional Disorders Short Question And Answers
Question 1. Microscopic picture of osteomalacia
Answer:
- Osteomalacia shows the following microscopic features
- Failure of mineralization of the osteoid matrix
- Decreased mineralization at the borders between osteoid and bone
- Osteoid remains unstained by von Kossa’s stain while calcified bone is stained black
- Increased osteoclastic activity and fibrosis of marrow is seen
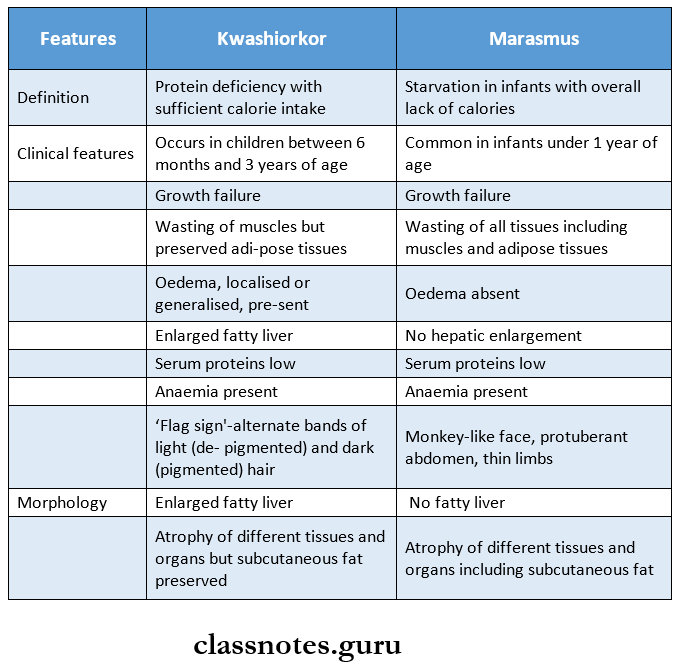
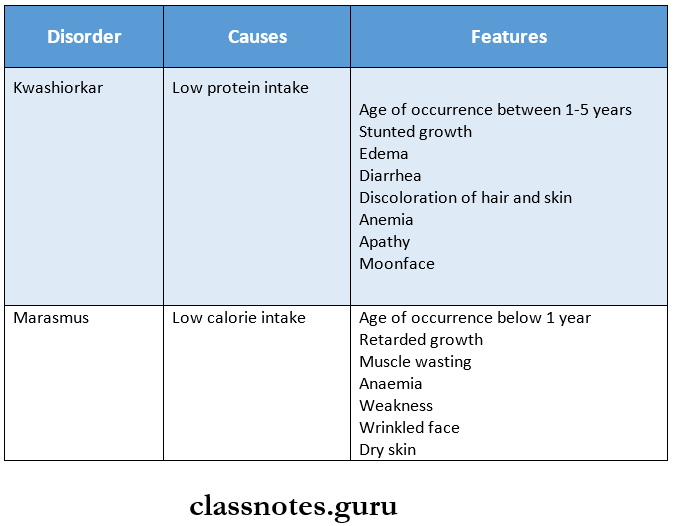
Question 2. Mention two differences between Kwashiorkar and marasmus
Answer:
Question 3. Scurvy
Answer:
- Vitamin C deficiency results in scurvy.
- Lesions and clinical manifestations of Vit. C deficiency are seen more commonly in two extreme age groups i.e., early childhood and geriatric patients.
Following manifestations are seen in vitamin C deficiency.
- Hemorrhage diathesis – A marked tendency to bleed which is characteristic of scurvy. There may be
- Skeletal lesions – There is a deranged formation of the osteoid matrix but not deranged mineralization. Growing tubular bones as well as flat bones are affected.
- Delayed wound healing.
- Anaemia – Normocytic normochromic type.
- Skin rash – Hyperkeratotic and follicular rash may occur.
- Lesions in teeth and gums – Scurvy may interfere with the development of dentin. The gums are soft and swollen, may bleed easily, and get infected commonly.
Question 4. Kwashiorkor
Answer:
- Protein deficiency with sufficient calorie intake is called as kwashioker.
- There is an enlarged fatty liver and atrophy of different tissues and organs but subcutaneous fat is preserved.
Kwashiorkor Clinical Features:
- Occurs in children between 6 months and 3 years of age.
- Generalized/localized edema is present.
- Anaemia.
- Wasting of muscles.
- Growth failure.
- Hair changes – Overall loss of color.
- A flag sign is seen – alternate bands of light and dark hair.
Question 5. Vitamin B12
Answer:
It is cyanocobalamine
Coenzyme Forms:
- 5′- Deoxyadenosyl cobalamin
- Methylcobalamin
Vitamin B12 Functions:
1. Synthesis of methionine from homocysteine
- Vitamin B12 is used as Methylcobalamin in this reaction
2. Isomerization of methymalonyl CoA to succinyl CoA
- It occurs in the presence of vitamin B12 Coenzyme, deoxyadenosine cobalamin
Vitamin B12 Dietary Requirements:
- Adults- 3 micrograms/day
- Children- 0.5-1.5 micrograms/day
- During pregnancy and lactation- 4 micrograms/day
Question 6. Vitamin B12 deficiency
Answer:
A deficiency of vitamin B12 leads to
- Pernicious anemia
- Characterized by low hemoglobin levels, decreased number of erythrocytes, and neurological manifestations
- Neuronal degeneration
- Demyelination of the nervous system
Question 7. Protein-energy malnutrition
Answer:
- It is the most common nutritional disorder of developing countries
- The two extreme forms of it are
- Kwashiorkor
- Marasmus
Question 8. Enumerate causes and investigations in vitamin D deficiency.
Answer:
Causes of Vitamin D Deficiency:
- Inadequate exposure to sunlight
- Dietary deficiency of vitamin D
- Malabsorption of lipids
- Derangement of vitamin D metabolism
- Resistance of end-organ to respond to vitamin D
Vitamin D Deficiency Investigations: