
Diseases Of Oral Cavity And Salivary Glands Important Notes
1. Developmental defects of the tongue
- Macroglossia
- Aglossia
- Fissuredtonghe
- Hairy tongue
- Tongue-tie
- Bifidtongue
2. Leukoplakia is defined as a white patch or plaque on oral mucosa exceeding 5mm India meter which cannot be rubbed off nor can be classified into any other disease
3. Sequele of dental caries
- Pulpitis-acute, chronic
- Apicalgranuloma
- Apical abscess
Diseases Of Oral Cavity And Salivary Glands Short Essays
Question 1. Cancrum oris
Answer:
- Cancrum oris or noma or necrotizing stomatitis is an inflammatory disease of the oral cavity.
- It occurs more commonly in poorly nourished children like in kwashiorkor, infectious diseases such as measles, immune deficiencies, and emotional stress.
- The lesions are characterized by necrosis of the marginal gingiva and may extend onto oral mucosa, causing cellulitis of the tissue of the cheek.
- The overlying skin becomes inflamed, edematous, and finally necrotic, the commencement of gangrene is noted
- The appearance of blackening of skin and extremely foul odor.
- Patients may have a high temperature during the course of the disease, may suffer secondary infections, and may die from toxemia and pneumonia.
- Cancrum oris Treatment: Antibiotics should be administered before the patient reaches the final stages of the disease.
Read And Learn More: Pathology Question And Answers
Question 2. Adenocarcinoma(or)Leukoplakia
Answer:
Leukoplakia Definition: Leukoplakia may be clinically defined as a white patch/plaque on the oral mucosa, exceeding 5 mm in diameter, which cannot be rubbed off nor can be classified into any other diagnosable disease.
Leukoplakia Etiology:
- Smoking especially pipe and cigar smokers
- Chronic friction example, ill-fitting dentures
- Local irritants like.
- Alcohol
- Very hot and spicy food.
- Beverages
Leukoplakia Morphology:
- Lesions may appear white, whitish yellow, or red velvety of more than 5 mm in diameter and variable in appearance.
- Usually circumscribed, slightly elevated, smooth/wrinkled, speckled nodular.
Leukoplakia Histology:
Microscopic examination reveals two types:
- Hyperkeratotic
- Dysplastic type.
1. Hyperkeratotic type: This is characterized by orderly and regular hyperplasia of squamous epithelium with hyperkeratosis on the surface.
2. Dysplastic type:
- Shows irregular stratification of the epithelium, focal areas of increased and abnormal mitotic figures, hyperchromatism, pleomorphism, loss of polarity, and individual call keratinization.
- Subepithelial tissue shows inflammatory infiltration of lymphocytes and plasma cells.
- Mild dysplasia reverts to normal but severe dysplasia indicates progression to carcinoma.
Leukoplakia Treatment:
- Elimination of irritating factors and includes:
- Administration of Vit A, Vit B, and estrogens.
- X-ray therapy
- Fulguration
- Surgical excision
- Topical chemotherapy.
Question 3. Epulis
Answer:
- Epulis is also known as peripheral giant cell granuloma
- It is an unusual inflammatory lesion of the gingiva
Epulis Clinical Features:
- Age- young to middle-aged adults
- It begins during the middle trimester of pregnancy
- Nonpathological soft swelling of gums occurs
- Size-1-1.5 cm, hemispherical
- It is covered by intact or ulcerated mucosa
- On the cut section, it appears grey to brown
Epulis Microscopic Appearance:
- It shows an aggregation of multinucleated foreign bodies like giant cells separated by scanty fibro angiomatous stroma
- There may be foci of hemosiderin deposits or an inflammatory infiltrate secondary to mucosa ulceration
Epulis Differential Diagnosis:
- True central giant cell tumours
- Intraosseous reparative giant cell granuloma
Epulis Treatment:
- Removal of underlying etiology
- Surgical excision
Question 4. Ameloblastoma
Answer:
- Ameloblastoma is the most common benign but locally invasive epithelial odontogenic tumor.
- It occurs in both the maxilla and mandible, but the posterior mandible in the molar ramus is the most common location.
- Clinically ameloblastoma presents as slow enlarging, painless, bony hard swelling of the jaw.
- Histologically, ameloblastoma shows many distinct patterns.
- Follicular pattern
- Plexiform pattern
- Acanthomatous pattern
- Basal cell pattern
- Granular cell pattern
- Treatment is complete surgical excision and long-term follow-up of the patient.
Question 5. Vincent’s angina
Answer:
Vincent’s infection primarily involves the free gingival margin, the crest of the free gingiva, and the interdental papillae, when such lesions spread to the soft palate and tonsillar areas it is known as Vincent’s angina.
Vincent’s Etiology: Vincent’s bacilli [fusiform bacilli) and borrelia vincentis are the causative organisms.
Vincent’s Clinical Features:
- This is a painful condition of the throat characterized by local ulceration of the tonsils, mouth, and pharynx.
- It is insidious in onset, with less fever and less discomfort in the throat.
- Membrane which usually forms over the tonsil can be easily removed revealing an irregular ulcer on the tonsil.
- It may occur as an acute illness with diffuse involvement of tissue/as a chronic illness consisting of ulceration of the tonsil.
Vincent’s Treatment:
- In the early acute stage, superficial cleansing of the oral cavity.
- In many cases, prompt regression of diseases results even without medication.
Question 6. Pleomorphic adenoma
Answer: Pleomorphic adenoma also called the mixed salivary tumor is the most common tumor of major [60 – 75%) and minor [50%) salivary glands.
Pleomorphic Adenoma Clinical features:
- The parotid gland is most commonly affected.
- More common in women and the 3rd – 5th decades of life.
- A tumour is a solitary, smooth surface but sometimes nodular, painless, and slow-growing.
- Often located below and in front of the ear and does not show fixation.
Pleomorphic Adenoma Morphology:
- Grossly, it is circumscribed, pseudo-encapsulated, rounded
- It may be a multilobulated, firm mass, 2 -5 cm in diameter, with a bosselated surface.
- Consistency is soft and mucoid.
Pleomorphic Adenoma Histology features: Characterised by the mixed appearance in which there are epithelial elements present in a matrix of mucoid, myxoid, and chondroid tissue.
- Epithelial component: Forms various patterns like ducts, acini, tubules, sheets, and strands of cells of ductal/myoepithelial origin.
- Ductal cells are cuboidal/columnar
- Myoepithelial cells are polygonal/spindle-shaped.
- Focal areas of squamous metaplasia and keratitis- -station may be present.
Pleomorphic adenoma Treatment:
- Surgical excision
- However, recurrence is much more common due to
- Incomplete surgical removal,
- Multiple foci of tumor,
- Pseudo encapsulation.
Diseases Of Oral Cavity And Salivary Glands Short Question And Answers
Question 1. Dentigerous cyst
Answer:
- A dentigerous cyst also called a follicular cyst arises from the enamel of an unerupted tooth
- Most commonly involved are mandibular 3rd molars and maxillary canines.
- Occurs more commonly in children and young individuals.
- Histologically, the dentigerous cyst is composed of a thin fibrous tissue wall lined by stratified squamous epithelium
- This cyst may resemble a radicular cyst, except that chronic inflammatory changes characteristic of radicular cyst, are usually absent in dentigerous cysts.
Dentigerous cyst Treatment:
- Large cysts are treated by marsupialization in young individuals
- Smaller lesions can be surgically removed entirely.
Question 2. Dental caries
Answer: Dental caries is the most common disease of dental tissues, destroying the calcified tissues of teeth.
Dental Caries Etiology:
- A diet rich in carbohydrates which is soft and sticky.
- If the plaque is not removed it leads to tooth decay.
- Caries occur chiefly in pits and fissures of molars and premolars
- The earliest change is the appearance of a small, chalky white spot on enamel which enlarges and becomes yellow/brown and forms various cavities.
- Pulpitis and necrosis of the pulp take place.
- If left untreated, caries may progress from pulpitis to apical granuloma and apical abscess.
Question 3. Cancrum oris
Answer:
- It occurs commonly in poorly nourished children or with immune deficiencies and emotional stress.
- Oral mucosae like marginal gingiva, lips, and cheeks are affected by necrosis and gangrene
- Patients may have high temperatures and may die from toxemia and pneumonia.
- Malnutrition must be treated and antibiotics may be useful in the early stages of the disease.
Question 4. Microscopic picture of Warthin’s tumor.
Answer:
- It is a benign tumor of the parotid gland comprising about 8% of parotid neoplasms, seen more commonly in men.
- Grossly, the tumor is encapsulated, round/oval with a smooth surface.
- The cut surface shows characteristic slit-like/cystic spaces, containing milky fluid and having papillary projections.
Microscopically, the tumour shows 2 components.
- Epithelial parenchyma and
- Lymphoid stroma
- Epithelial parenchyma: This is composed of glandular and cystic structures having papillary arrangement and is lined by characteristic eosinophilic epithelium.
- Lymphoid stroma is present under the epithelium in the form of prominent lymphoid tissue, often with germinal centers.
Question 5. Typhoid ulcer
Answer:
- Typhoid ulcer occurs in the jejunum and colon
- It is aligned with their long axis along the length of the bowel
- The base of the ulcer is black due to sloughed mucosa
- Margins are slightly raised due to inflammatory edema and cellular proliferation
- Regional lymph nodes are enlarged
Typhoid ulcer Complications:
- Perforation of ulcers
- Hemorrhages
Systemic Hypertension Important Notes
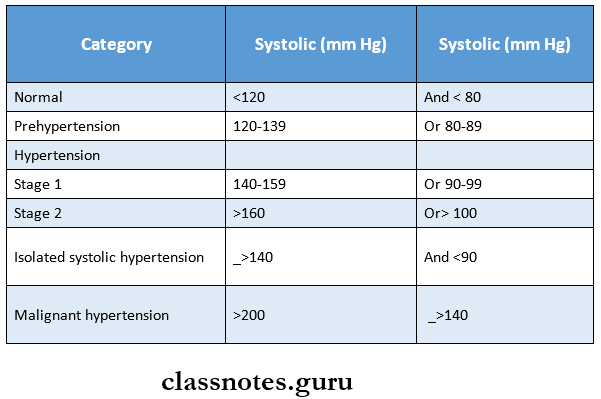
1. Values
- Systolic-140-159mmHg
- Diastolic-90-99mmHg
2. Effects of hypertension
- Nephrosclerosis
- Hypertensive heart disease
- Retinopathy
- Intracranial hemorrhage
3. Types of aneurysms affecting larger Intracranial arteries
- Berry
- Mycotic
- Fusiform
4. Features of hypertensive retinopathy
- Arteriolar narrowing
- Flame shaped hemorrhages
- Macular star
- Cotton wool spots
- Microaneurysms
- Arteriovenous nicking
- Hard exudates
Systemic Hypertension Short Essays
Question 1. Hypertension
Answer:
- Hypertension is the sustained resting blood pressure of more than 160/95 mm Hg.
- It is the most common cause of cardiac failure and a major risk factor for atherosclerosis and cerebral hemorrhage
Hypertension Classification:
1. Clinical classification
2. General classification
- Primary or essential hypertension
- Occurs due to unknown cause
- Secondary hypertension
- Occurs due to the presence of renal, endocrine, or other diseases
3. According to the clinical course
- Benign hypertension
- Moderate elevation of blood pressure occurs
- Rise is slow over the years
- It is often asymptomatic
- Malignant hypertension
- It is a marked and sudden increase in blood pressure
- Occurs in patients with evidence of previous benign hypertension
- Often results in severe and acute renal, retinal, and cerebral damage
4. Etiological classification
- Essential or primary hypertension
- Hereditary
- Racial and environmental factors
- Risk factors modifying the course
- Secondary hypertension
- Renal diseases
- Endocrine disorders
- Coarctation of aorta
- Neurogenic
Effects of Hypertension:
- Nephrosclerosis
- Heart diseases
- Retinopathy
- Intracranial hemorrhages