
Complete Dentures Short Answers
Question 1. Parts of a complete denture
Answer:

Question 2. Steps in the fabrication of a complete denture
Answer:
- Diagnosis and treatment planning
- Making diagnostic casts
- Mouth preparation
- Primary impression
- Primary cast
- Fabrication of custom trays
- Secondary impression
- Master cast
- Fabrication of occlusal rims
- Recording jaw relations
- Articulation
- Arrangement of artificial teeth
- Try in
- Processing of denture
- Insertion
- Post-insertion review and maintenance
Read And Learn More: Prosthodontics Question And Answers
Question 3. Effects of aging.
Answer:
- Young people have lighter teeth due to translucent enamel
- Old people have dark & opaque teeth due to secondary dentin formationShiny teeth in old people
- Teeth with a brownish tinge in older people. Certain diseases are limited to certain ages
- Thus, age can be used to rule out certain systemic conditions
- Age also determines the prognosis.
Complete Dentures: Short Questions and Answers
Question 4. Metal dentures.
Answer:

Question 5. Gagging
Answer:
The gag reflex is a normal, healthy defense mechanism to prevent foreign bodies from entering the trachea
Causes of Gagging:
- Over-extended denture borders
- Unstable occlusal conditions
- Systemic conditions
- Alcoholism, smoking
Dental Prosthodontics MCQs
Features of Gagging:
- Causes the displacement of the denture
- Triggered by tactile stimulation of the soft palate, the posterior part of the tongue, and the fauces
Site of Gagging:
- Posterior part of the maxillary denture
- Distolingual part of mandibular denture
Gagging Treatment:
- Correction of overextended dentures
- Correction of occlusal vertical dimensions and occlusal prematurities
Question 6. Angular cheilitis.
Answer:
Angular Cheilitis Etiology:
- Angular Cheilitis occurs at the angle of the mouth among persons having deep commissural folds secondary to the overclosure of the mouth
- Angular Cheilitis can occur among persons with lip-licking habits, denture-wearing, or deficiency of riboflavin, vitamin B12, and folic acid

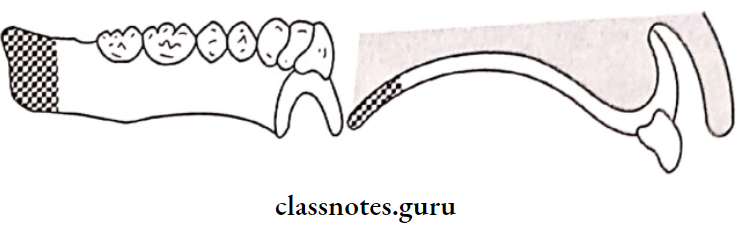
Question 7. Kelly’s combination syndrome.
Answer:
Kelly’s Combination Syndrome was identified by Kelly in 1972 in patients wearing a maxillary complete denture opposing a mandibular distal extension prosthesis
Complete Denture FAQs
Kelly’s Combination Syndrome Pathogenesis:
- It occurs in a sequential manner
- The patient tends to concentrate the occlusal load on the remaining natural teeth
- Results in more force acting on the anterior portion of the maxillary denture
- Increased resorption of the anterior part of the maxilla
- The labial flange will displace and irritate the labial vestibule
- Posteriorly, there will be fibrous overgrowth in the maxillary tuberosity
- The shift of the occlusal plane posteriorly downwards processes resorption in the mandibular distal extension denture-bearing area
- Mandible shifts anteriorly during occlusion
- There is
- Decrease in vertical dimension at occlusion
- Decrease in retention and stability of a denture
- Disocclusion of lower anterior
- Reduced periodontal support of anterior teeth
Question 8. Infection control
Answer:
Infection Control Methods:
- Immunization:
- Vaccination for Hepatitis B for all dental personnel
- Personal Barrier:
- Hand washing before gloving and after degloving
- Gloves protect against contamination
- Changed between patients and for the same patient, is torn or worn out
- Face Mask:
- Protects from inhalation of aerosols
- Prevents spatter from the patient’s mouth
- Prevents droplets from the contaminated solution
- Protective clothing
- Gown with long sleeves, high neck & long knee length
- Eyewear:
- Prevention of bacterial/viral contact
- Face Mask:
- Surgical Asepsis:
- Preparation of the surgical site
- Draping the patient
- Isolation
- Surface Asepsis:
- Sterilization of instruments
- Use of disposable instruments
- Disposal Of Waste: Methods
- Incineration
- Burial in a landfill
- |Sterilization
Question 9. Hypermobile ridge tissue.
Answer:
Hypermobile Ridge Tissue Cause:
- Due to excessive residual ridge resorption, Management:
- Small tissues that do not interfere with tissue functioning:
- Left Untreated: Impression is made using the mucositis technique
- Large Tissues: removed surgically
Denture Objective Questions
Question 10. Polished surface.
Answer:
- The Polished Surface is defined as that portion of the surface of a denture that extends in an occlusal direction from the border of the denture and includes the palatal surfaces
- The Polished Surface is the part of the denture base that is usually polished, and it includes the buccal and lingual surfaces of the teeth
- Polished Surface refers to the external surfaces of the lingual, buccal, and labial flanges and the external palatal surface of the denture
- The Polished Surface should be well polished and smooth to avoid the collection of food debris
- The Polished Surface should be harmonious with the oral structures
- They should not interfere with the action of oral mus- culture
Question 11. Denture irritation hyperplasia.
Answer:
The hyperplastic reaction of mucosa over the borders of the denture

Question 12. Xerostomia.
Answer:
Xerostomia refers to a subjective sensation of a dry mouth, but is not always associated with salivary hypofunction
Xerostomia Etiology:
- Developmental:
- Salivary gland aplasia
- Water/metabolic Loss:
- Impaired fluid intake
- Hemorrhage
- Vomiting/diarrhea
- Iatrogenic:
- Medications:
- Antihistamines: Diphenhydramine
- Decongestants: Pseudoephedrine
- Antidepressants: Amitriptyline
- Antipsychotic: Haloperidol
- Antihypertensive: Methyldopa, CCB
- Anticholinergic: Atropine
- Medications:
- Radiation therapy of the head and neck:
- Both stimulated and unstimulated salivary flow decreases with increasing radiotherapy.
- Systemic Diseases:
- Sjogren’s syndrome
- Diabetes mellitus
- Diabetes insipidus
- HIV infections
- Psychological disorders.
- Graft-versus-host disease
- Local Factors:
- Decreased mastication.
- Smoking
- Mouth breathing
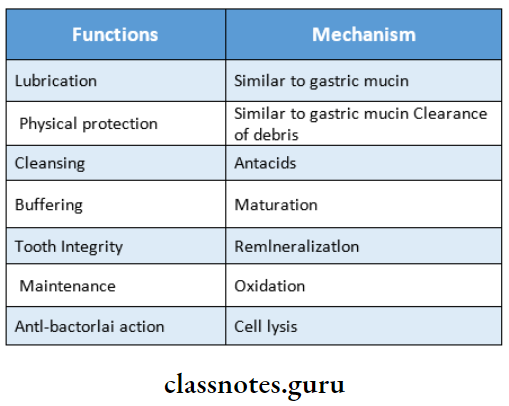
Question 13. Functions of saliva.
Answer:
Question 14. Combination syndrome.
Answer:
Combination Syndrome was identified by Kelly in 1972 in patients wearing a maxillary complete denture opposing a mandibular distal extension prosthesis
BDS Prosthodontics Viva Questions
Combination Syndrome Pathogenesis:
- Combination Syndrome occurs in a sequential manner
- The patient tends to concentrate the occlusal load on remaining natural teeth resulting in more force acting on the anterior portion of the maxillary denture
- Increased resorption of the anterior part of the maxilla
- The labial flange will displace and irritate the labial vestibule. Posteriorly, there will be fibrous overgrowth in the maxillary tuberosity
- The shift of the occlusal plane posteriorly downwards processes resorption in the mandibular distal extension denture-bearing area
- Mandible shifts anteriorly during occlusion
- Decrease in vertical dimension at occlusion
- Decrease in retention and stability of the denture
- Disocclusion of lower anterior
- Reduced periodontal support of anterior teeth.