Morphology Of Cell Injury Important Notes
1. Types of necrosis
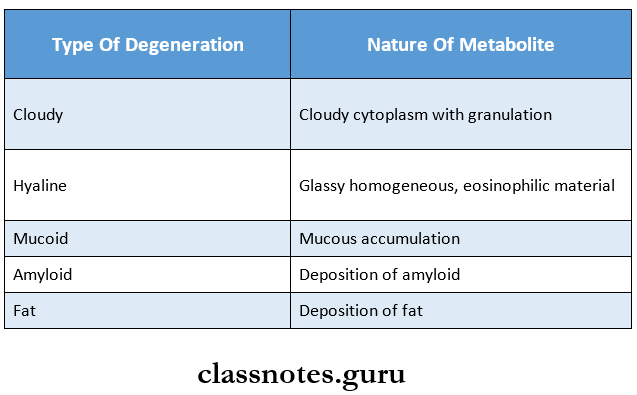
2. Types of degeneration
- Cloudy swelling – a most common type
- Hydropic
- Hyaline
- Mucoid degeneration
3. Morphological forms of cell injury
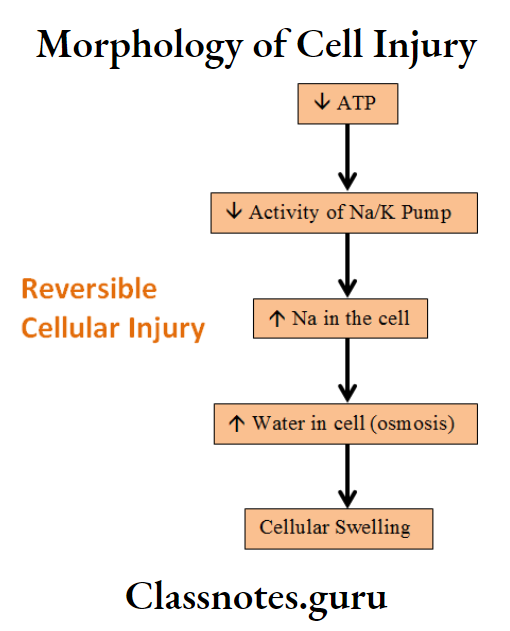
- Reversible
- Cellular Swelling
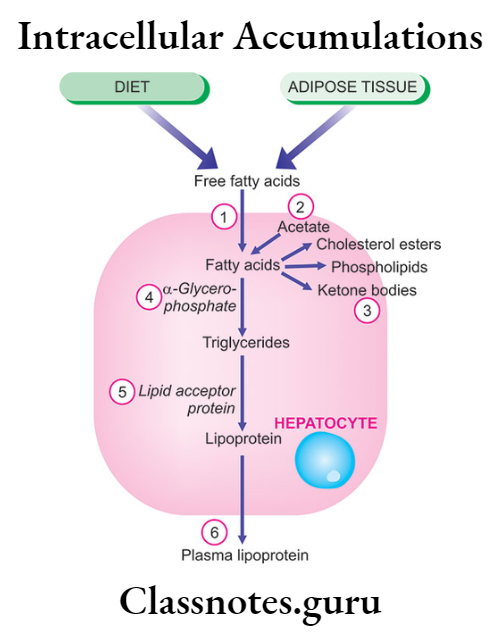
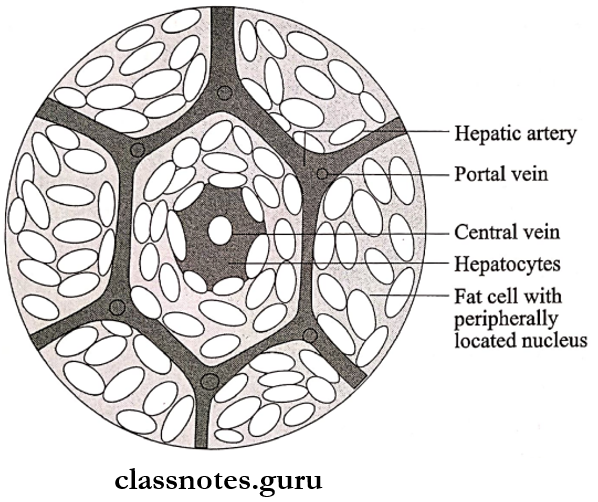
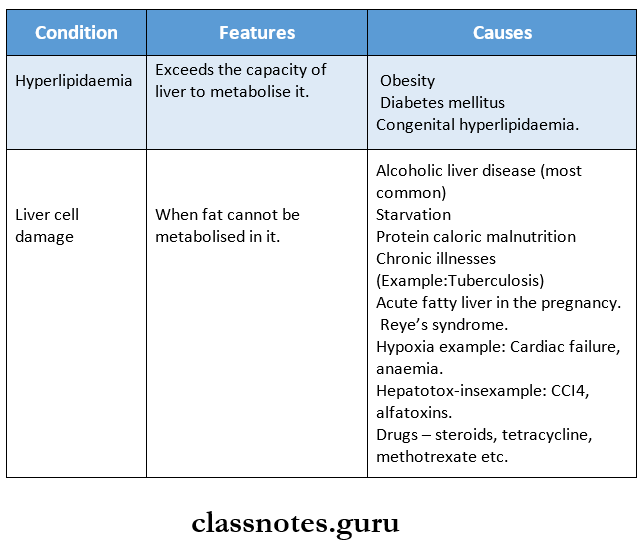
- Fatty change
- Hyaline change
- Mucoid change
- Irreversible
- Apoptosis
- Autolysis
- Necrosis
4. Apoptosis
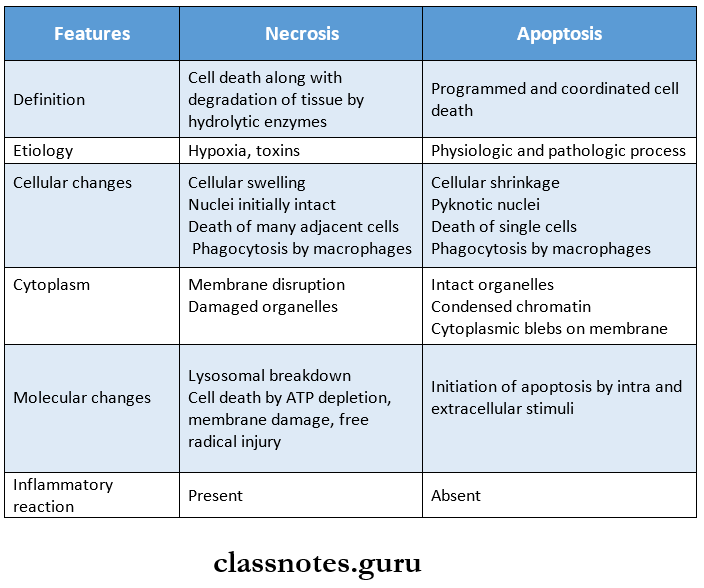
- Apoptosis is physiological or programmed cell death
- It eliminates cells that are genetically altered or injured beyond repair without eliciting a severe host reaction
- It prevents the development of epithelial dysplasia by programmed cell death
- It is usually single-cell death and undergoes coagulative necrosis.
Morphology Of Cell Injury Long Essays
Question 1. Classify necrosis. Discuss its nuclear changes.
Answer:
Necrosis Classification:
Necrosis is classified into the following types:
1. Coagulative necrosis
- Caused by irreversible focal injury
2. Liquefaction necrosis
- Occurs due to ischaemic injury and bacterial or fungal infections
Read And Learn More: Pathology Question And Answers
3. Caseous necrosis
- Found in the center of foci of tuberculous infections
4. Fat necrosis
- Occurs at two anatomically different locations
5. Fibrinoid necrosis
- Deposition of fibrin-like material occurs
Nuclear Changes In Necrosis:
1. Pyknosis
- It is a condensation of nuclear chromatin
2. Karyolysis
3. Karyorrhexis
Question 2. Define necrosis. Classify and discuss different types of necrosis.
(or)
Define necrosis. Discuss etiopathogenesis and morphology of various types of necrosis.
Answer:
Definition:
Necrosis is defined as a localized area of death of tissue followed by degradation of tissue by hydrolytic enzymes liberated from dead cells, it is invariably accompanied by an inflammatory reaction
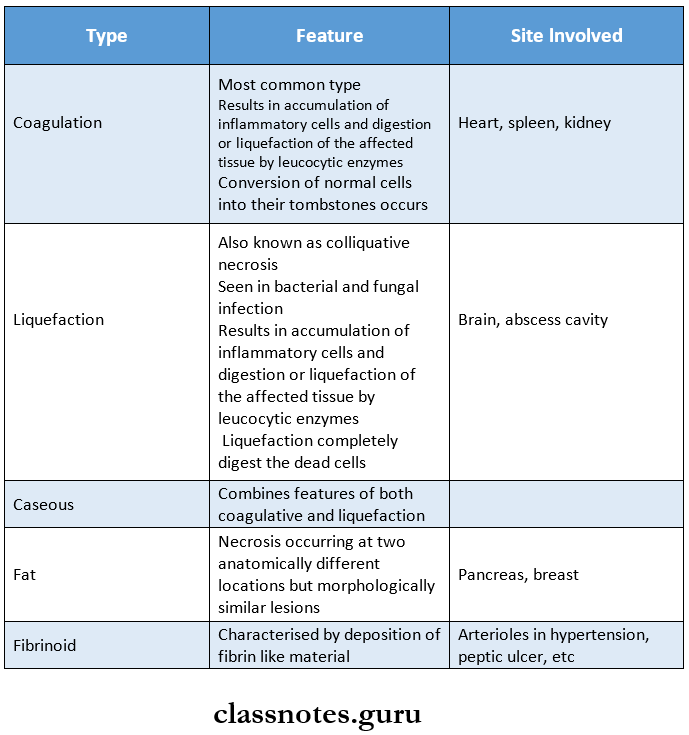
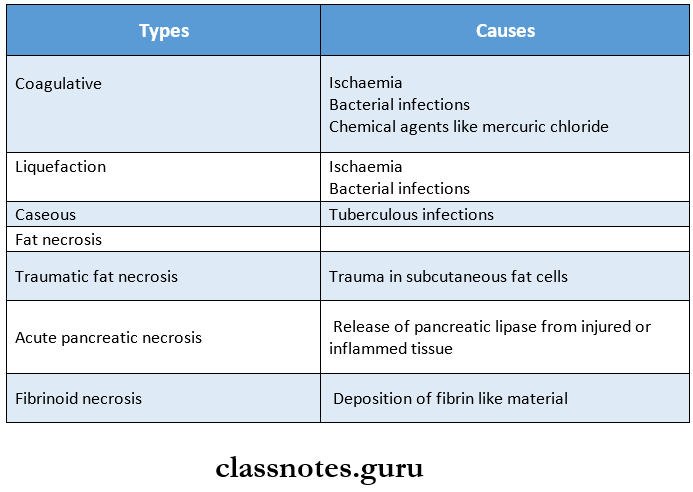
Necrosis Types:
There are five types of necrosis
1. Coagulative necrosis
- Causes:
- Ischaemia
- Bacterial infection
- Chemical agents like mercuric chloride
- Pathogenesis
- Irreversible cell injury
- Results in sudden cessation of blood flow
2. Liquefaction necrosis
- Causes:
- Ischaemia
- Bacterial infections
- Pathogenesis
- Bacterial and fungal infections produce hydro-lytic enzymes
- This causes the degradation of tissue
3. Caseous necrosis
- Occurs in the center of foci of Tuberculous infections
4. Fat necrosis
- Occurs at two anatomically different locations
- Types
- Acute pancreatic necrosis
- Traumatic fat necrosis
5. Fibrinoid necrosis
- Deposition of fibrin-like material occurs
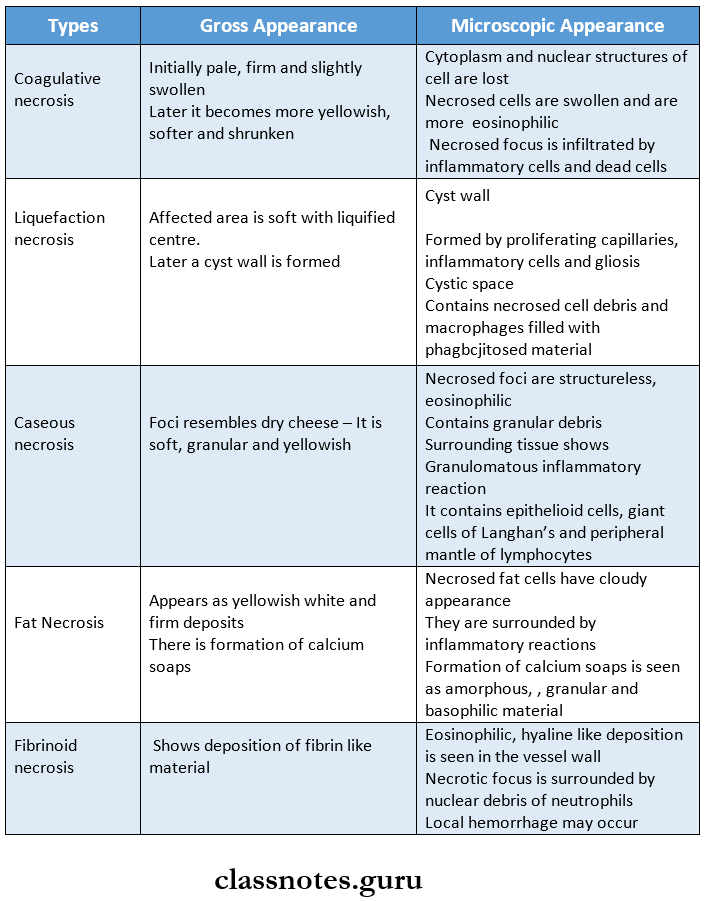
Morphology of types of Necrosis:
Question 3. Define and classify gangrene. Write the differences between dry and wet gangrene
Answer:
Definition:
- Gangrene is a form of necrosis of tissue with superadded putrefaction
Gangrene Classification:
- Gangrene is classified into two main types
- Dry gangrene
- Wet gangrene
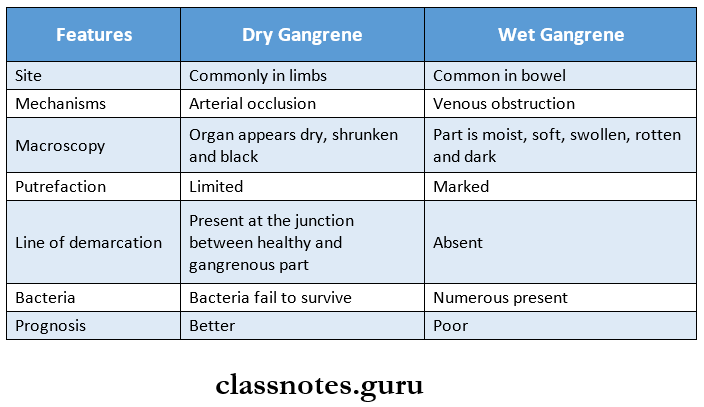
Difference Between Dry and Wet Gangrene:
Question 4. Write about wet gangrene.
Answer:
Wet Gangrene:
Wet gangrene usually occurs in moist tissues and organs
Site Involved:
- Mouth
- Bowel
- Lung
- Cervix
- Vulva
Wet Gangrene Cause:
Wet Gangrene Pathogenesis:
- The affected part is filled with blood
- It favors the rapid growth of Putrefaction bacteria
- Formation of toxic products by bacteria
- Absorption of toxic products
- Causes septicemia
- Finally causes death
Wet Gangrene Features:
1. Gross features
- The affected part appears soft, swollen, putrid, rotten, and dark
- Part is stained dark
2. Microscopic features
- Coagulative necrosis is seen
- There is ulceration of the mucosa and intense inflammatory infiltration
- Lumen shows mucus and blood
- There is no line of demarcation present.
Morphology Of Cell Injury Short Essays
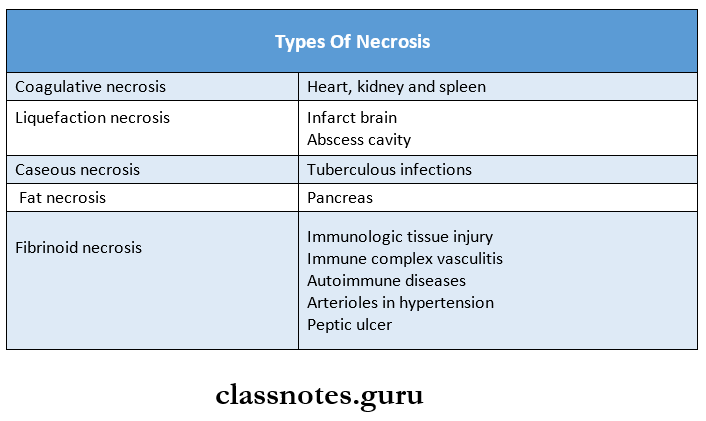
Question 1. Types of necrosis with examples
Answer:
Types of Necrosis:
Question 2. Dry gangrene
Answer:
Gangrene:
- Gangrene is a form of necrosis of tissue with super-added putrefaction
Dry Gangrene:
- It is a form of gangrene occurring due to Ischaemia
Dry Gangrene Causes:
- Ischaemia
- Atherosclerosis
- Buerger’s disease
- Raynaud’s disease
- Trauma
- Ergot poisoning
Dry Gangrene Features:
- Begins in the distal part of a limb
- Occurs in one of the toes which is farthest from the blood supply
- Here bacteria fail to grow in the necrosed tissue
- Gangrene spreads slowly upwards until it reaches an area with a good blood supply
- The line of demarcation is seen between the gangrenous part and the viable part
Dry Gangrene Gross Appearance:
- The affected part is dry, shrunken, and dark black
- It appears black due to the liberation of hemoglobin from hemolysed red blood cells which is acted upon by hydrogen disulfide produced by bacteria
- The line of demarcation is seen
Dry Gangrene Microscopic Appearance:
- Necrosis with smudging of the tissue is seen
- The line of demarcation contains inflammatory granulation tissue
Question 3. What is dystrophic calcification? Give two examples.
Answer:
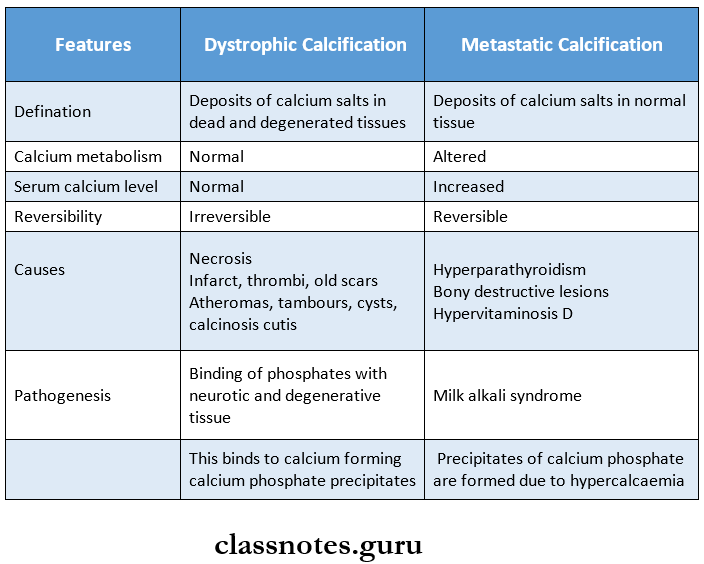
Dystrophic calcification is the deposition of calcium salts in dead and degenerated tissues with normal calcium metabolism and normal serum calcium levels
Dystrophic Types:
1. Calcification in dead tissue: Examples
- Caseous necrosis in tuberculosis
- Liquefaction necrosis in chronic abscess
- Fat necrosis
- Gamma Gandy bodies in chronic venous congestion
- Infarcts
- Thrombi in veins
- Haematomas in bones
- Dead parasites
- Calcification in breast cancer
- Congenital toxoplasmosis
2. Calcification in degenerated tissues
- Stroma of tumors
- Atheromas
- Dense old scars
- Cysts
- Calcinosis cutis
- Senile degeneration
Dystrophic Pathogenesis:
1. Initiation
- Precipitates of calcium and phosphate begin to accumulate both intracellularly and extracellularly
2. Propagation
- Mineral deposits propagate to form mineral crystals
Question 4. Differences between Necrosis and Apoptosis.
Answer:
Morphology Of Cell Injury Short Question And Answers
Question 1. Irreversible cell injury
Answer:
- Cell injury is defined as a variety of stresses a cell en-. counters as a result of changes in its internal and external environment
- When such an injury is severe and persistent, cell death occurs
- Such an injury is called irreversible cell injury
Irreversible cell injury Features:
- The inability of the cell to reverse mitochondrial dysfunction
- Disturbance in cell membrane functions
- Reduction in ATP
- Continued depletion of proteins
- Reduced intracellular pH
- Leakage of lysosomal enzymes
Question 2. Etiology of cell injury
Answer:
Cell injury occurs due to the following causes:
1. Genetic causes
2. Acquired causes
- Hypoxia and ischemia
- Physical agents
- Chemical agents
- Microbial agents
- Nutritional derangements
- Immunologic agents
- Aging
- Iatrogenic factors
- Idiopathic
Question 3. Free radical injury
Answer:
- The free radical injury occurs in situations like ionizing radiation
- Oxygen free radicals are produced within the mitochondrial matrix
- They are:
- Superoxide
- Hydrogen peroxide
- Hydroxyl radical
Free radical injury Effects:
- Lipid peroxidation
- Oxidation of proteins
- DNA damage
- Cytoskeletal damage
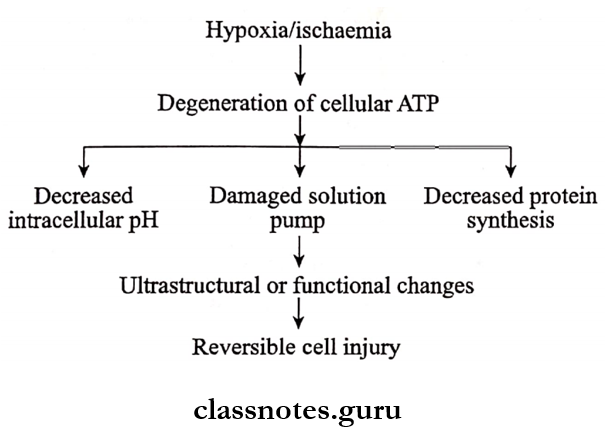
Question 4. Reversible cell injury
Answer:
- Cell injury is defined as a variety of stresses a cell encounters as a result of changes in its internal and external environment
- When the stress is mild to moderate, the injured cell may recover, it is called reversible cell injury
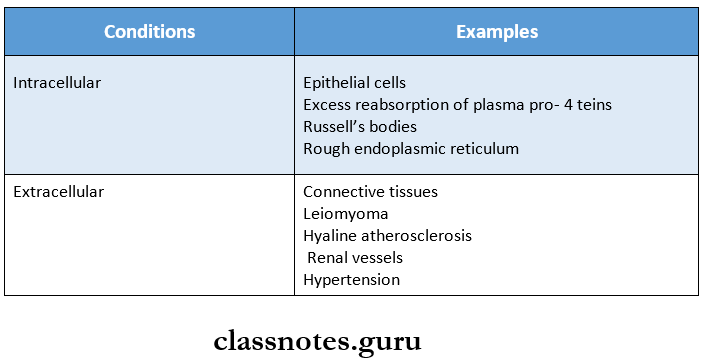
Question 5. Hyaline calcification
Answer:
- It describes the glassy, homogeneous, eosinophilic appearance of a material
- It is associated with pathological conditions that may be intracellular or extracellular
Question 6. Dystrophic and metastatic calcification.
Answer:
Question 7. Apoptosis
Answer:
Apoptosis is a form of coordinated and internally programmed cell death that has significance in a variety of physiologic and pathological conditions
1. Apoptosis in biological processes
- Organized cell destruction during the development of the embryo
- Physiologic involution of cells in hormone-dependent tissues
- Normal cell destruction
2. Pathologic process
- Cell death in tumors
- Cell death by cytotoxic T cells
- Cell death in viral infections
- Pathologic atrophy of organs