Sphenoid Bone
Sphenoid Bone Terminology
‘Sphenoid’ is derived from the Greek word ‘sphen’ which means ‘a wedge’. The bone is so named because it is wedged between the frontal bone in front and the occipital bone behind.
Sphenoid Bone Anatomical Position
- Hypophyseal fossa faces upwards.
- Pterygoid processes descend vertically downwards.
- Openings of sphenoidal sinuses are directed forward.
Sphenoid Bone Articulations
The Sphenoid is a key bone in the cranial skeleton as it articulates with the following eight bones:
- Frontal
- Parietal
- Temporal
- Occipital
- Vomer
- Zygomatic
- Palatine
- Ethmoid
Sphenoid Bone Shape
Sphenoid resembles a ‘bat’ with its wings stretched out.
Sphenoid Bone Features And Attachments
Sphenoid consists of a central body, four wings (two greater and two lesser), and two pterygoid processes (right and left).
Sphenoid Bone Body
It has six surfaces (superior, inferior, anterior, posterior, and two lateral) and a pair of air-filled cavities (sphenoidal sinuses).
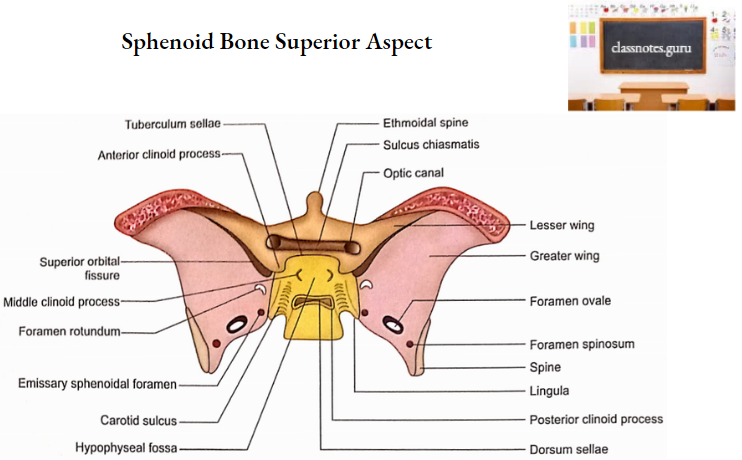
1. Surfaces
- Superior (cerebral) surface: It shows of following features from anterior to posterior.
- Jugum Sphenoidale
- It is smooth.
- It articulates with the posterior margin of the cribriform plate.
- It is related on each side to the gyrus rectus of the cerebral hemisphere and olfactor tract.
- Sulcus Chiasmatis
- It is a transverse groove behind the jugum sphenoidale
- Optic chiasma lies just above it.
- It leads laterally into the optic canal.
- Tuberculum Sellae
- It is an elevation just behind the sulcus chiasmatis.
- Sella Turcica
- It is a depressed area behind the tuberculum sellae.
- The hypophyseal fossa is the deepest part of the Sella turcica. It lodges the pituitary gland.
- The anterior part of Sella turcica is bounded on each side by an elevation called the middle clinoid process.
- Dorsum Sellae
- It is a square plate of bone behind the sella turcica.
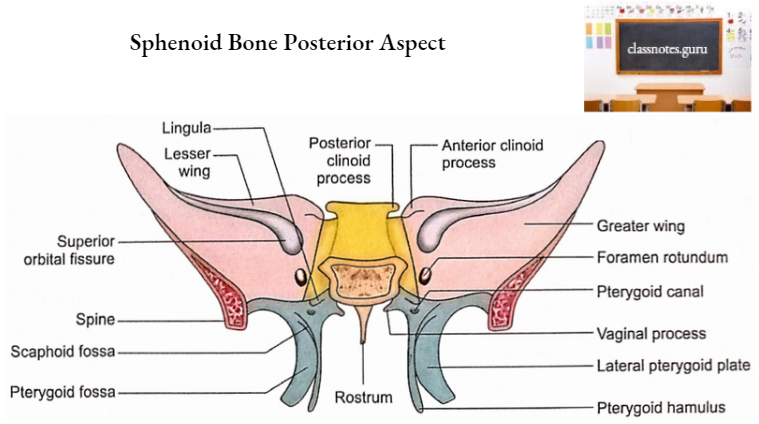
- Posterior Clinoid Process
- Superior angles of dorsum sellae project laterally into posterior clinoid processes.
- Attached margin of tentorium cerebelli is attached to this process on each side.
- The upper part of the clivus
- It is sloping behind the dorsum sellae.
- It is formed by the posterior parts of the body and dorsum sellae.
- It supports the pons.
- Posterior Surface
- It is rough.
- It articulates with the basilar part of the occipital bone.
- Anterior And Inferior Surfaces
- The midline of the anterior surface is marked by a triangular crest called a sphenoidal crest.
- The sphenoidal crest articulates with the upper part of the posterior border of the perpendicular plate of the ethmoid.
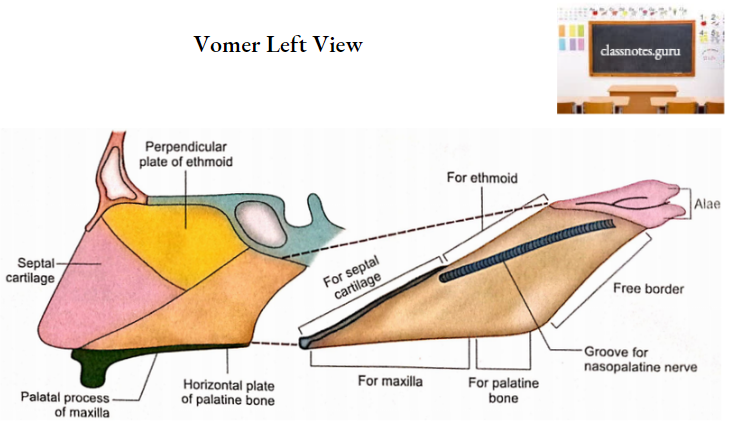
- The midline of the inferior surface is marked by a triangular spine called a sphenoidal rostrum. It fits into the groove between the alae of the vomer.
- Both anterior and inferior surfaces of the body on either side of the midline, are occupied by a thin plate of bone called sphenoidal concha.
- Each sphenoidal concha consists of an anterior part which is vertical and quadrangular and a posterior part which is horizontal and triangular.
- Anterior Part
- It consists of an upper and lateral depressed area which completes the posterior ethmoidal sinus and articulates below with the orbital process of palatine bone.
- Its lower and medial part forms part of the roof of the nasal cavity and is perforated above by the round opening through which the sphenoidal sinus communicates with the sphenoethmoidal recess of the nasal cavity.
- Posterior Part
- It forms part of the roof of the nasal cavity and completes the sphenopalatine foramen.
- Lateral Surface
- Its lower part unites with the greater wing and medial pterygoid plate.
- Its upper part is marked by a carotid sulcus which lodges the internal carotid artery and cavernous sinus.
- The lateral margin of the carotid sulcus at its posterior end projects backward into tongue-shaped lingula.
- The lingula lies just above the posterior opening of the pterygoid canal.
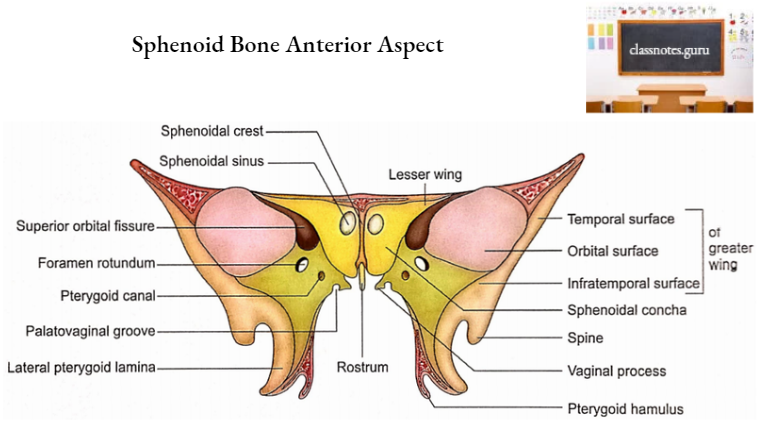
2. Sphenoidal Sinuses
- These are two large air spaces present in the body of the sphenoid.
- The two sinuses are separated by a septum and are rarely symmetrical.
- Relations
- Superiorly:
- Optic chiasma.
- Pituitary gland.
- Laterally
- Internal carotid artery.
- Cavernous sinus.
- Size
- Vertical height: 2 cm (a little less than 2 cm)
- Transverse breadth: 1.8 cm
- Anteroposterior depth: 2.1 cm (little more than 2 cm).
- Note: For simplification, students may consider all the measurements approximately as 2 cm.
- Each sinus communicates with the spheno-ethmoidal recess.
- Development
- Sphenoidal sinus starts developing as nasal mucosal evagination during intrauterine life.
- These are in the form of minute cavities at birth.
- It develops to its adult size in adolescence.
Sphenoid Bone Wings
1. Greater wings
There are two greater wings, a right and a left. Each has three surfaces (cerebral, lateral, and orbital) and several margins.
- Surfaces
- Cerebral Surface
- It is concave. It forms part of the middle cranial fossa. It is related to the temporal lobe of the cerebrum. It possesses the following foramina.
- Foramen rotundum
- It is situated in the anteromedial part. The maxillary nerve passes through it.
- Foramen ovale
- It is situated posterolateral to foramen rotundum. It transmits:
- Mandibular nerve.
- Accessory meningeal artery.
- Lesser petrosal nerve.
- Emissary vein.
- Emissary sphenoidal foramen
- It is an inconstant foramen present medial to foramen ovale. It transmits the emissary vein.
- Foramen spinosum
- It is lateral to foramen ovale. It transmits:
- Middle meningeal artery.
- Nervus spinosus.
- Canaliculus innominatus
- It is occasionally present between foramen ovale and foramen spinosum. If present, it transmits lesser petrosal nerve.
- Lateral Surface
- It is convex from above downwards.
- The infratemporal crest is an anteroposterior ridge that divides the lateral surface into upper temporal and lower infratemporal parts.
- The temporal surface forms part of the temporal fossa and gives origin to the temporalis muscle.
- The infratemporal surface forms the roof of the infratemporal fossa and gives origin to the upper head of the lateral pterygoid muscle. This surface possesses openings of foramen ovale and foramen spinosum.
- The spine of the sphenoid is a projection at the posterior end of the lateral surface. It shows the following relations and attachments:
- Tip gives attachment to spheno-mandibular ligament.
- Medially it is related to the chorda tympani nerve and auditory tube.
- Laterally it is related to the auriculotemporal nerve.
- Orbital Surface
- It is quadrilateral in shape.
- It forms the posterior part of the lateral wall of the orbit.
- Its upper serrated edge articulates with the orbital plate of the frontal bone.
- Its lateral serrated margin articulates with the zygomatic bone.
- Its inferior smooth border forms the posterolateral boundary of the inferior orbital fissure.
- Its medial sharp margin constitutes the lower boundary of the superior orbital fissure. A projection from this border provides attachment to a common tendinous ring.
- Below the medial end of the superior orbital fissure is a depressed area pierced by foramen rotundum.
- Margins
- The tip of the greater wing is called the parietal margin. It articulates with the sphenoidal angle of the parietal bone at the pterion.
- The posterior margin of the greater wing extends from the body of the sphenoid to its spine. Its medial half forms the anterior boundary of the foramen lacerum and receives the opening of the pterygoid canal. Its lateral half articulates with the petrous temporal.
- The lateral margin extends forward from the spine to the tip of the greater wing. This is also called the squamosal margin because it articulates with the squamous part of the temporal bone.
- Medial to the tip there is a triangular rough area for the frontal bone.
- The anterior angle of the triangular area continues with a serrated margin (lateral margin of the orbital surface) which articulates with the zygomatic bone.
2. Lesser Wings
It is a triangular bone extending laterally from the anterosuperior part of the body. It consists of a tip, two roots (anterior and posterior), two surfaces (superior and inferior), and two borders (anterior and posterior).
- Тір
- It is the lateral end of the lesser wing.
- It is situated near the lateral end of the superior orbital fissure.
- Roots
- The lesser wing is connected to the body by anterior and posterior roots.
- The two roots enclose the optic canal which transmits the optic nerve and ophthalmic artery.
- Surfaces
- Superior Surface
- It forms the posterior part of the floor of the anterior cranial fossa.
- Inferior Surface
- It forms the superior boundary of the superior orbital fissure and the posterior part of the orbital roof.
- Borders
- Anterior border
- It articulates with the posterior border of the orbital plate of the frontal bone.
- Posterior Border
- It is free.
- Its medial end forms the anterior clinoid process to which is attached the free margin of tentorium cerebelli.
3. Superior Orbital Fissure
- It is a triangular slit-like communication between the orbit and the middle cranial fossa.
- Boundaries
- Medial: Body of sphenoid Apex: Frontal bone
- Superior: Lesser wing of sphenoid.
- Inferior: Greater wing of sphenoid.
- It transmits the following structures:
- Structures that enter the orbit
- Upper and lower divisions of the oculomotor nerve.
- Trochlear nerve.
- Three branches (lacrimal, frontal, and nasociliary) of the ophthalmic division of the trigeminal nerve.
- Abducent nerve.
- Orbital branch of the middle meningeal artery.
- Sympathetic filaments.
- Structures that appear from the orbit
- Superior and inferior ophthalmic veins.
- Recurrent meningeal branch of the lacrimal artery.
Pterygoid Processes
- The pterygoid process on each side descends vertically downwards from the junction of the body and the greater wing of the sphenoid.
- Each consists of a lateral and a medial pterygoid plate.
- The plates unite anteriorly in the upper part to enclose a fossa called pterygoid fossa.
- The plates are not united in the lower portion to form a pterygoid fissure which is filled by the pyramidal process of palatine bone.
- The anterior surface of the pterygoid process forms the posterior boundary of the pterygopalatine fossa.
- The anterior opening of the pterygoid canal is located in this region. Some details of the two pterygoid plates are as follows:
1. Lateral pterygoid plate
It has two surfaces (lateral and medial) and two borders (anterior and posterior).
- Surfaces
- Lateral Surface
- It forms the medial wall of the infratemporal fossa and gives origin to the lower head of the lateral pterygoid muscle.
- Medial Surface
- It forms the lateral wall of the pterygoid fossa which gives origin to the deep head of the medial pterygoid muscle.
- Borders
- Anterior Border
- It forms the posterior boundary of the pterygomaxillary fissure.
- Posterior Border
2. Medial Pterygoid Plate
It has two surfaces (lateral and medial) and two borders (anterior and posterior).
- Surfaces
- Lateral surface
- It forms the medial wall of the pterygoid fossa and is related to the tensor palate muscle.
- Medial surface
- It forms the lateral wall of the corresponding posterior nasal aperture.
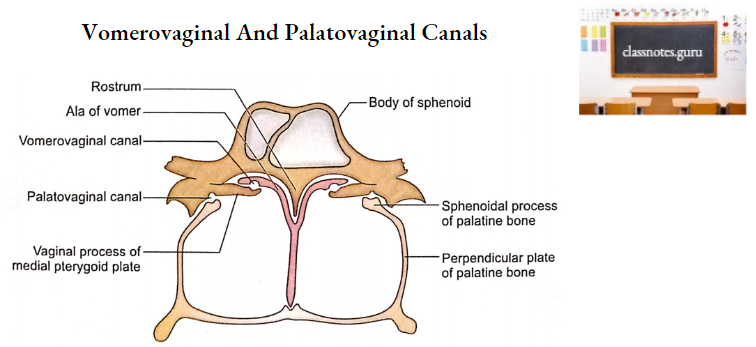
- Vaginal process is a thin lamina projecting medially from its upper part under the body of the sphenoid.
- A groove on the anterior part of the undersurface completes the palatovaginal canal with the sphenoidal process of the palatine bone.
- This canal transmits the pharyngeal branch of the maxillary artery and the pharyngeal branch of the pterygopalatine ganglion.
- The vaginal process articulates medially with ala of the vomer and forms vomero-vaginal canal between the two. This canal transmits branches of pharyngeal nerves and vessels.
- Borders
- Anterior border
- It articulates with the posterior border of the perpendicular plate of the palatine bone.
- Posterior border
- At its upper end, it splits to enclose the scaphoid fossa which gives origin to the tensor palati muscle.
- Its upper end shows a small projection called the pterygoid tubercle which lies immediately below the posterior end of the pterygoid canal.
- Pharyngobasilar fascia is attached to its whole extent while the superior constrictor arises from its lower part only.
- A hook-like process at its lower end is called pterygoid hamulus. Tondon of tensor palati winds around this process. Superior constrictor and pterygomandibular raphe are also attached to it.
- An angular process projecting from the middle of this margin is called processus tubarius.
- The posterior border above this process is called the notch of the auditory tube. This process and notch support the medial end of the auditory tube.
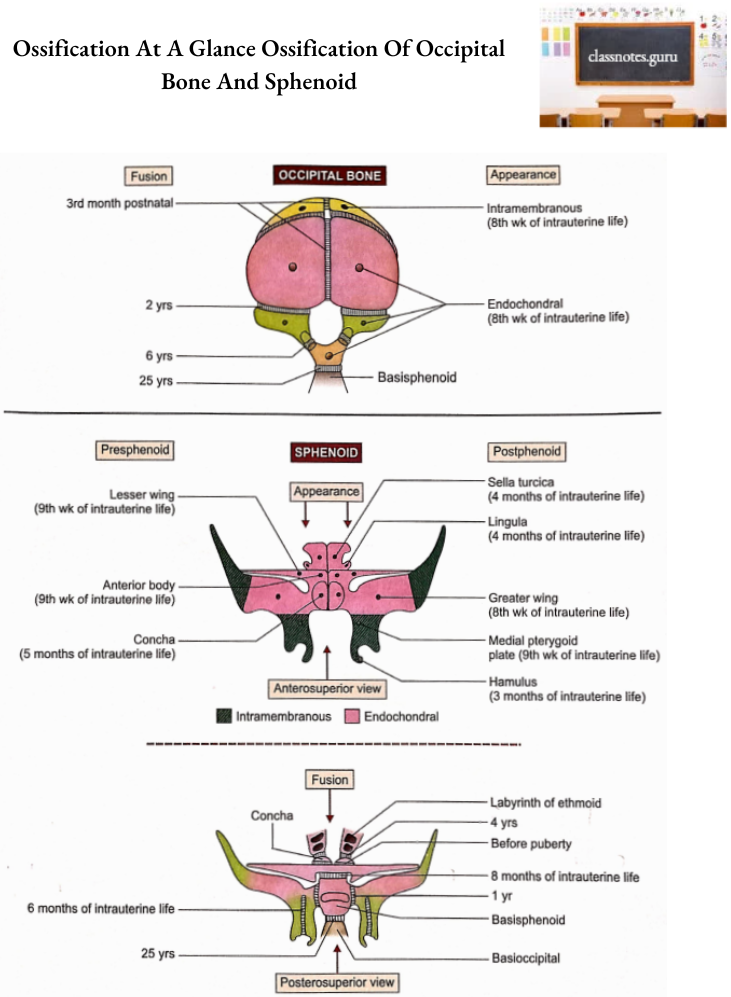
Sphenoid Bone Ossification
- Sphenoid ossifies partly in the membrane and partly in cartilage.
- Parts ossifying in the membrane are as follows:
- Greater wings except for their roots.
- Pterygoid processes except pterygoid hamuli.
- Parts ossifying in cartilage are as follows:
- Body of sphenoid.
- Lesser wings.
- Sphenoidal conchae.
- Roots of greater wings.
- Pterygoid hamuli.
- From an ossification point of view, the sphenoid is divided into presphenoidal and post-sphenoidal parts.
- The presphenoidal part is comprised of parts lying in front of tuberculum sellae, i.e. anterior part of the body, lesser wings, and sphenoidal conchae.
- Two centers appear for each of these components as follows:
- Anterior body-9th week of intrauterine life.
- Lesser wings-9th week of intrauterine life.
- Conchae-5th month of intrauterine life.
- Rest of the sphenoid is included in post sphenoidal part. Two centers appear for each of the following components of the post-sphenoidal part.
- Sella turcica-4th month of intrauterine life.
- Lingulae 4th month of intrauterine life. Greater wings (including lateral pterygoid plates)-8th week of intrauterine life.
- Medial pterygoid plates-9th week of intrauterine life.
- Hamuli-3rd month of intrauterine life.
- Fusions of different components of sphenoid take place as follows:
- Medial and lateral pterygoid plates fuse with each other at about 6th month of intrauterine life.
- The presphenoidal part of the body fuses with the postsphenoidal part of the body at about the 8th month of intrauterine life.
- At birth, the sphenoid is in three parts, a central part consisting of the body and lesser wings and two lateral parts, each consisting of the greater wing and the pterygoid process.
- Greater wing fuses with the body at about 1st year.
- Concha fuses with the ethmoidal labyrinth at about 4th year.
- Concha fuses with the body of the sphenoid before puberty.
- The body of the sphenoid fuses with the basilar part of the occipital bone at about the 25th year.
Sphenoid Bone Applied Anatomy
- In the anterior part of the hypophyseal fossa, there is occasionally a vascular foramen termed as craniopharyngeal canal. The canal sometimes extends inferiorly to the exterior of the skull and is said to mark the original position of Rathke’s pouch.
- Premature ossification of sutures between pre and post-sphenoidal parts and sphenoid and occipital bones is often observed in achondroplasia.
- Anomalous development of the pre-sphenoidal elements may lead to excessive separation of the two orbits (hypertelorism).
- Observation of the sella turcica and the hypophyseal fossa in radiographs is important clinically because they may reflect pathological changes such as a pituitary tumor or aneurysm of the internal carotid artery.
- Decalcification of the dorsum sellae is one of the signs of a generalized increase in intracranial pressure.
- The lateral wall of the optic canal is fractured during optic nerve decompression in the optic canal.
- A fracture of the sphenoid bone may lacerate the optic nerve resulting in blindness.
- Basilar fracture of the skull through the sphenoid bone may lacerate the internal carotid artery resulting in the carotid-cavernous fistula. This leads to pulsating exophthalmos.
- Collection of air in the cranial cavity (aerocele) may occur if the basilar fracture of the skull involves a sphenoidal sinus.
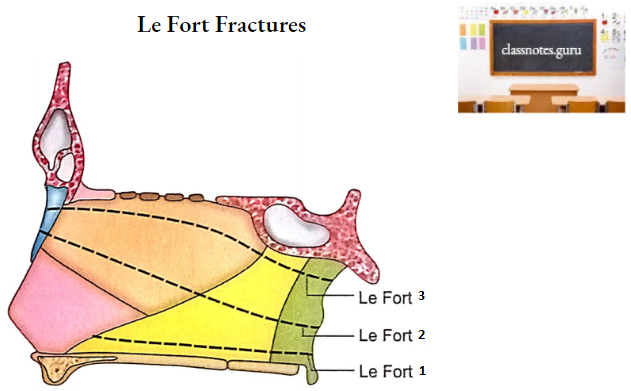
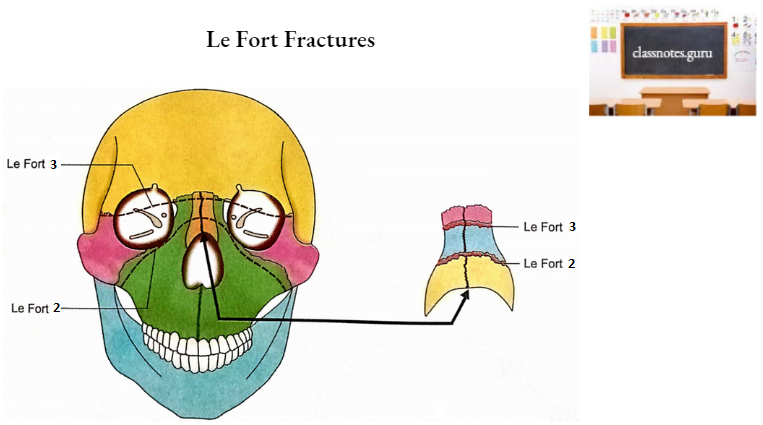
- Involvement of the pterygoid processes of the sphenoid is a constant feature in cases of Le Fort fractures of the mid-facial skeleton but the location of a fracture depends upon its type.
- In Le Fort 1 fracture, the lower 3rd of the pterygoid plates is involved while in Le Fort 3 fracture the roots of pterygoid plates are fractured.
- Large areas of the body and medial pterygoid plates are clothed in mucosa and, therefore, fractures of these parts of the sphenoid may open into the nasal cavity or sphenoidal sinus with potential risk of infection.