Amyloidosis Important Notes
1. Congo red stain
- All amyloid types have an affinity for it
- It stains amyloid orange in colour and when viewed in polarized light shows apple green birefringence
2. Primary and secondary amyloidosis
- Primary amyloidosis
- Most common form
- Occurs most commonly in plasma cell dyscrasias
- It occurs in the heart, skin and skeletal muscle
- Secondary amyloidosis
- Occurs as a complication of chronic infection or non-infectious inflammatory conditions
- Typically distributed in the kidney, liver, spleen and adrenals
3. Amyloidosis of the kidney
- The most common and most serious
- Affected kidneys may be normal-sized or enlarged
- The cut surface shows a pale, waxy and translucent appearance
4. Diagnosis of amyloidosis
- Biopsy
- FNAC of abdominal subcutaneous fat followed by Congo red staining
- Injection of congo red dye intravenously in a living patient
- Electrophoresis
- Bone marrow aspiration
Amyloidosis Long Essays
Question 1. Define amyloidosis. Discuss in detail the etiopathogenesis of amyloidosis. Add a note on its staining characteristics.
Answer:
Definition:
- Is the term used for a group of diseases characterised by extracellular deposition of fibrillar proteinaceous sub-stance called amyloid having a common morphological appearance, staining properties and physical structure but with variable protein composition.
Read And Learn More: Pathology Question And Answers
Pathogenesis:
- Irrespective of the type of amyloid, amyloidogenesis in vivo, occurs in the following sequence.
- The pool of amyloidogenic precursor protein is present in circulation or may be present in response to stimuli.
- A nidus of fibrillogenesis is formed which stimulates the deposition of amyloid protein
- Partial degradation or proteolysis occurs before the deposition of fibrillar protein
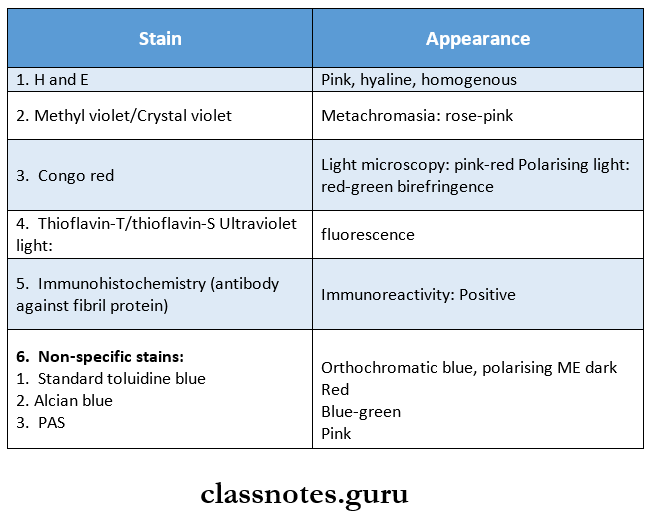
Staining characteristics of Amyloid:
Amyloidosis Short Essays
Question 1. Classification of amyloidosis
Answer:
1. Based on the cause:
- Primary – with unknown cause and deposition is in the disease itself.
- Secondary – As a complication of some underlying known disease.
2. Based on the extent of amyloid deposition:
- Syssniic (generalised) – Involving multiple organs.
- Localised – involving one/2 organs.
3. On histological basis:
- Peri collagenous-corresponding in distribution to primary amyloidosis.
- Perirectulin – corresponding in distribution to secondary amyloidosis.
4. Based on tissues:
- Mesenchymal – organs derived from mesoderm.
- Parenchymal – GFgafiS ueFiveu fFGfil ectoderm and
5. Clinicopathologic classification:
- Systemic (generalised) amyloidosis:
- Primary (AL)
- Secondary/reactive/inflammatory (AA)
- Heradofamilial (ATTR, AA, others)
- Localised amyloidosis:
- Senile cardiac (ATTR)
- Senile cerebral (AB, APP)
- Endocrine (hormone precursors)
- Tumour forming (AL)
Question 2. Microscopy of sago spleen
Answer:
- Sago’s spleen is a form of amyloidosis of the spleen
- In it splenomegaly is not marked
- The cut surface shows translucent, pale and waxy nodules resembling sago grains
- Microscopically it shows amyloid deposits in the walls of arterioles of the white pulp
- Later these deposits replace follicles
Question 3. Pathological changes in amyloidosis
Answer:
Gross Changes:
- The organ is usually enlarged, pale and rubbery
Cut Surface:
- It shows firm, translucent and waxy parenchyma
Microscopic Changes:
- Amyloid deposits are found in the walls of small blood vessels
- Later these deposits produce large macroscopic changes in the blood vessels
- Produces pressure atrophy
Amyloidosis Short Question And Answers
Question 1. Amyloidosis of liver
Answer:
It occurs in about half of the cases of systemic amyloidosis
Amyloidosis of Liver Pathology:
1. Gross features
- Liver is
- Enlarged
- Pale
- Waxy
- Firm
2. Microscopic features
- Initially
- Amyloid appears in the space of Disse
- Later
- Deposits increase
- It compresses cords of hepatocytes
- Liver cells get shrunken
- They become atrophic and are replaced by amyloid
- Hepatic function is normal
- Portal tracts and Kupffer cells are involved rarely.
Question 2. Source and nature of amyloid
Answer:
Amyloid is composed of 2 main types of complex proteins:
1. Comprises about 95% of amyloid.
- Comprises about 95% of amyloid.
- This consists of a meshwork of fibril proteins which are delicate, randomly dispersed, non-branching and having an indefinite length.
- Chemically 2 major types of amyloid proteins were identified.
- AL (Amyloid light chain) protein.
- AA (Amyloid-associated) protein.
- Other proteins which include Transthyretin
- β-Amyloid protein.
- Ap2 microglobulin.
- Amyloid from hormone precursor proteins.
- Immunoglobulin heavy chain amyloid (AH)
2. Non-fibrillae components.
- Comprises of about 5% of amyloid material.
- These include the amyloid P (AP) component
- Aglipoprotein – E (apoE)
- Sulphated glycosaminoglycans
- α – 1 anti chymotrypsin
- Protein X